
Abstract
Background
As bacterial attachment and subsequent biofilm formation on the surface of a stent lumen may be important in initiating sludge formation and subsequent stent blockage, there is a need for antibiotic-eluting stents to prevent sludge formation by bacterial attachment and colonization.
Purpose
To evaluate the antimicrobial effects of cefotaxime-eluting covered self-expandable stents (CE-CSEMS) in a canine biliary model by using scanning electron microscopy (SEM) to analyze biofilm formation on the inner surface of the stents.
Material and Methods
Three 10% (wt/vol) CE-CSEMS, three 20% (wt/vol) CE-CSEMS, and three control stents (CS) were endoscopically inserted into the bile ducts of nine mongrel dogs, which were followed up for 8 weeks. Gross and SEM examinations were performed to access the development and degree of biofilm formation in dogs with CS and CE-CSEMS.
Results
All stents were successfully inserted into canine bile ducts without any procedure-related complications. All nine dogs remained in good health without jaundice over the next 8 weeks. The degree of biofilm was similar in dogs implanted with CS and CE-CSEMS using two concentrations of cefotaxime either by gross inspection or SEM. All stent types showed a similar biofilm structure with relatively uniform thickness on SEM.
Conclusion
Cefotaxime does not prevent biofilm development in a canine biliary model. Biofilm formation on the inner surface of biliary stents may be prevented by using broad-spectrum antimicrobial agents and stents that maintain a steady release of these agents for a long time, thus prolonging stent patency.
Transhepatic or endoscopic placement of self-expandable metallic stents (SEMS) has become an established palliative treatment in the relief of malignant biliary obstructions (1,2). Although SEMS prolong survival, shorten hospital stay, and improve patient quality of life (2), they can occlude over time because of tumor ingrowth, proximal and distal tumor overgrowth, sludge formation, food debris, or tissue hyperplasia resulting from chronic irritation (1, 3–5). Tumor ingrowth may be prevented by implantation of covered self-expandable metallic stents (CSEMS); several covering materials have been found to prevent tumor ingrowth, thereby avoiding the need for re-intervention (6–13). Comparisons of CSEMS covered with silicone or polyurethane and uncovered stents have yielded conflicting results on the efficacy and safety of these CSEMS (14–18). Although expanded polytetrafluoroethylene (ePTFE)-covered SEMS have been found effective in preventing tumor ingrowth and are associated with relatively low rates of stent occlusion (19), the pores on the ePTFE may allow bacterial attachment, increase the amount of bile sludge formation, and potentially decrease the long-term patency rate of these stents (10).
As bacterial attachment and subsequent biofilm formation on the surface of a stent lumen may be important in initiating sludge formation and subsequent stent blockage (20–22), there is a need for antibiotic-eluting stents that prevent sludge formation resulting from bacterial attachment and colonization. These antibiotics may kill free-floating bacteria before they attach to the stent surface, thus preventing biofilm formation. Cefotaxime, a third generation cephalosporin that has antimicrobial activity against Gram-positive and Gram-negative organisms, has been shown to be effective in the prophylaxis of biliary tree infections after endoscopic retrograde cholangiopancreatography (23,24). Cefotaxime-eluting CSEMS (CE-CSEMS) may therefore prevent bacterial attachment and growth, thus reducing biofilm build-up and subsequent sludge formation. To our knowledge, the effects of antibiotic-eluting stents on animal bile ducts have not yet been reported. We therefore evaluated the antimicrobial effects of CE-CSEMS in a canine biliary model by utilizing scanning electron microscopy (SEM) to analyze biofilm formation on the stent surface.
Material and Methods
Preparation of cefotaxime-eluting CSEMSs
Control stents (CSs) (Mapssy covered stent, S&G Biotech Inc., Seoungnam, Gyunggi, Korea), 6 mm in diameter and 30 mm long when fully expanded and mounted onto an 8.5-F stent introducer set, were covered with ePTFE, except for their proximal and distal 2 mm ends. The resulting CE-CSEMS were coated with a membrane consisting of three layers, an inner polyurethane layer, middle drug eluting layer, and an outer ePTFE layer (Fig. 1). The drug-eluting layer was formed by dissolving polyurethane into an organic solvent, with 10% or 20% (wt/vol) cefotaxime (Hanmi, Seoul, Korea) incorporated into the poly-urethane solution. The ePTFE layer was coated onto the drug-eluting layer using a dip-coating technique. After the middle layers dried, the pure polyurethane layers were coated using the same coating technique. The pure poly-urethane layers were utilized to prolong the period of cefotaxime release because their biodegradation would have to occur prior to the biodegradation of the drug-eluting layers. The three layered membranes were subsequently everted, such that the ePTFE layer was on the outside and the pure polyurethane layer was on the inside. Each resulting CE-CSEMS (Fig. 2) was made in the company laboratory (S&G Biotech Inc.) and subsequently mounted onto an 8.5-F stent introducer set.
View of the covering membrane. The covering membrane consists of three layers, an inner pure polyurethane layer, a middle drug eluting (cefotaxime-polyurethane mixture) layer, and an outer ePTFE layer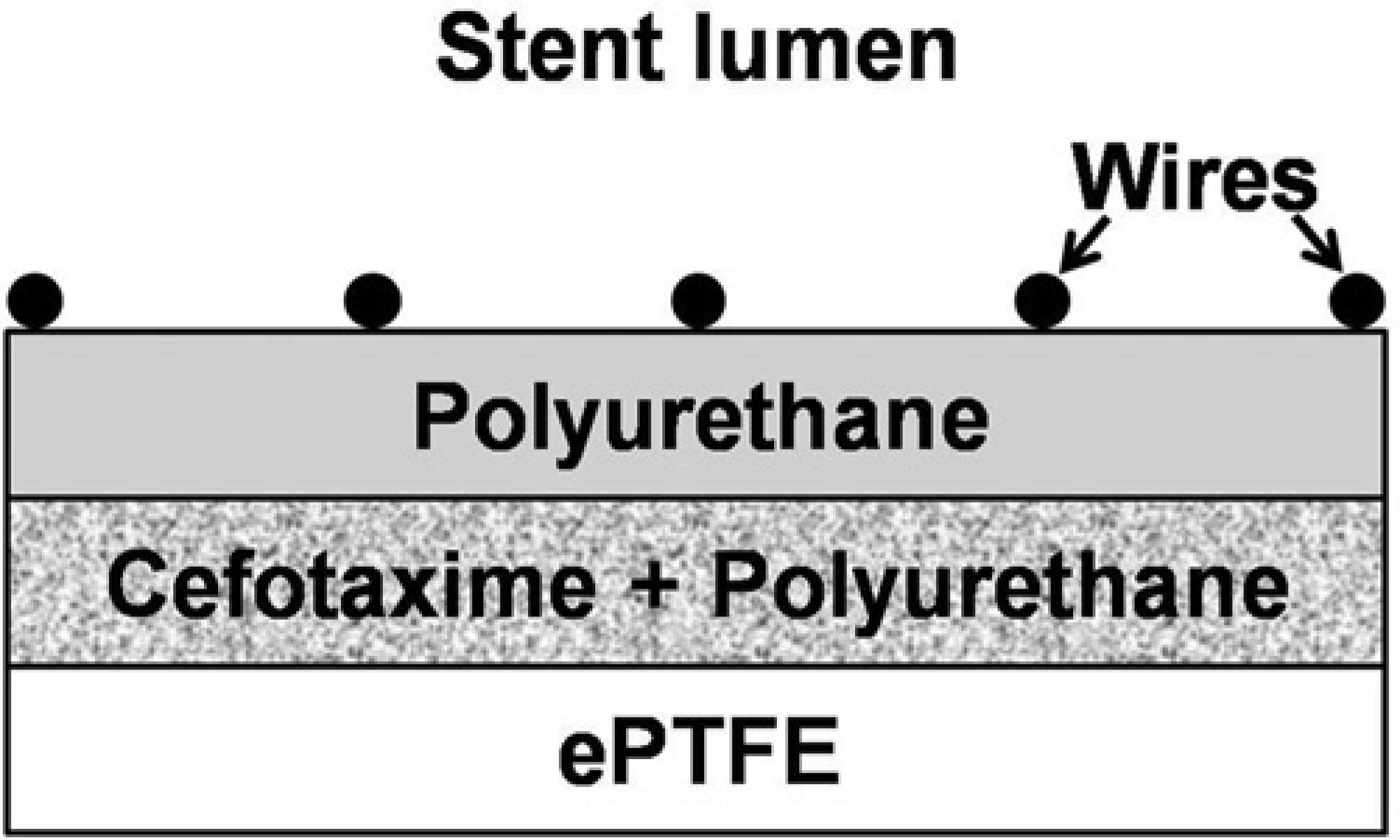
The control stents (CS) and cefotaxime eluting covered self-expandable metallic stents (CE-CSEMS) used in this study. CE-CSEMS-10, partially PTFE-covered stents containing 10% wt/vol cefotaxime. CE-CSEMS-20, partially PTFE-covered stents containing 20% wt/vol cefotaxime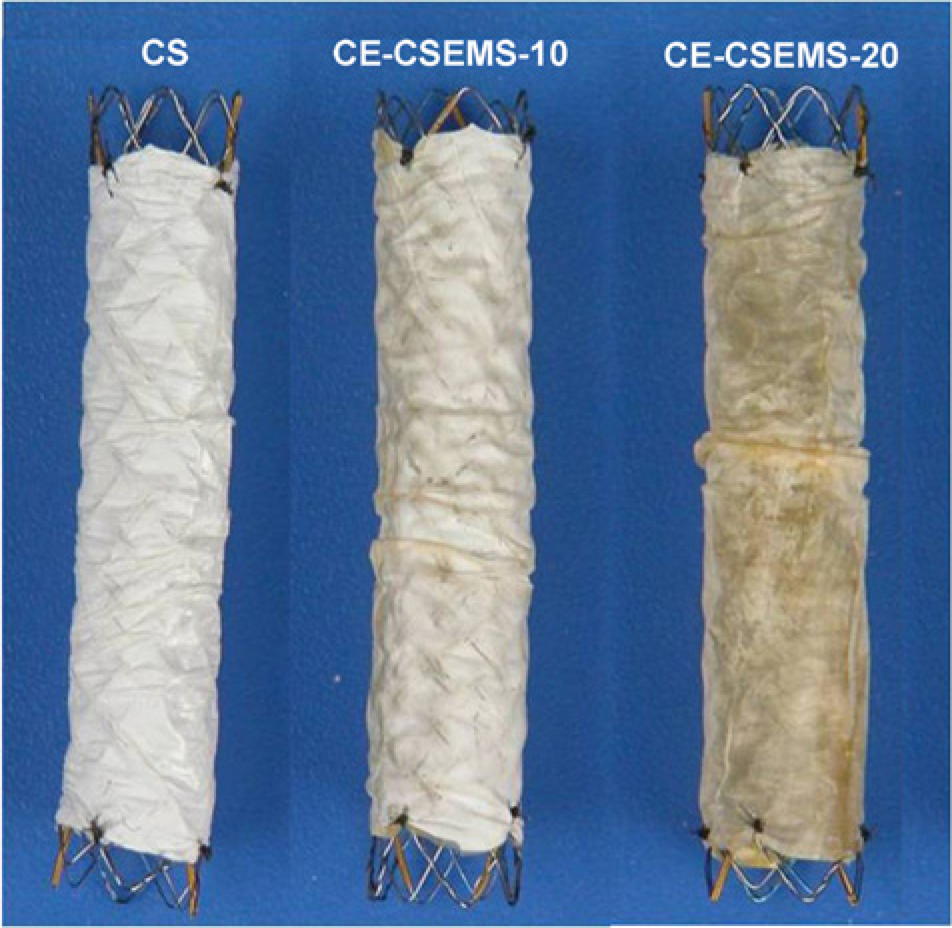
In-vitro study
To assess the efficacy of drug release, CE-CSEMSs were placed in phosphate buffered saline solution for 8 weeks, and cefotaxime release was measured by high-performance liquid chromatography. High percentages of cefotaxime (28–30% of the amount incorporated) were continuously released over 1 week, regardless of the cefotaxime concentration incorporated. However, small amounts of cefotaxime continued to be detected during the next three weeks (9–11% of the amount incorporated) and the next 4 weeks (7–8% of the amount incorporated). The total amount of drug released by 20% (wt/vol) cefotaxime-eluting SEMS was much greater than that released by 10% (wt/vol) CE-CSEMS (Fig. 3).
Cumulative release of cefotaxime in vitro. A CE-CSEMS-20 released a greater amount of cefotaxime than a CE-CSEMS-10 in a dose-dependent manner
Animal study
All experimental procedures were performed in accordance with the National Institutes of Health guidelines for humane handling of animals and were approved by the Committee on Animal Research at our institution.
Nine male mongrel dogs weighing 15–18 kg were randomly divided into a control group (n = 3), a 10% (wt/vol) CE-CSEMS group (CE-CSEMS-10, n = 3), and a 20% (wt/vol) CE-CSEMS group (CE-CSEMS-20, n = 3). Because it is difficult to make biliary strictures in dogs, we utilized a normal biliary model. All dogs were fasted for 24 h before stent placement. Anesthesia was induced by intramuscular injection ketamine hydrochloride (Yuhan, Seoul, Korea) and atropine sulfate (Daewon, Seoul, Korea), and was maintained throughout the procedures with intravenous ketamine hydrochloride. Each dog was placed in the left lateral decubitus position and covered with drapes for stent placement. Stents, prepared 2 days before the procedure (S&G Biotech Inc.), were inserted via an oral transpapillary approach using a 3.8-mm endoscope. After the papilla was located, the bile duct was cannulated with a catheter and a cholangiogram was obtained. Because reflux of intestinal contents into the stent may also cause sludge formation, we inserted all stents above the papilla under endoscopic and fluoroscopic guidance (Fig. 4). Postprocedural abdominal radiographs were obtained.
Stent insertion procedure under endoscopic and fluoroscopic guidance. (a) Fluoroscopic image showing positioning of the stent introducing system over a guide wire under endoscopic guidance; (b) Fluoroscopic image showing a fully expanded stent in the bile duct
Follow-up and scanning electron microscopic examination
Following stent placement, all dogs continued to be fed on a standard commercial diet without antibiotics. The dogs were sacrificed 8 weeks after stent placement, and the common bile duct and duodenum of each were excised en bloc. Bile ducts were incised longitudinally and the stents were removed and fixed in 10% formalin for SEM examination. The stents were then washed twice in PBS, their proximal and distal ends were cut with scissors, and the stent wires were carefully removed. Each remaining polymeric membrane was bisected along its long axis, dehydrated in ethanol, and critical-point dried. The surface was coated with platinum and examined by field emission SEM (Hitachi S-4700, Japan). The quantities of adherent microorganisms on the surfaces of covering membranes were compared among the three groups using repeated-measures one-way analysis of variance. The degree of biofilm formation was graded as none, mild (<30% of the membrane surface), moderate (30–60% of the membrane surface), or severe (>60% of the membrane surface).
Results
Stent placement and follow-up
All stents were successfully placed in canine bile ducts without any procedure-related complications. None of the stents migrated, either immediately after stent placement or during follow-up. The mean body weight of all nine dogs increased by 1.1 kg, and all dogs remained in good health without jaundice until they were euthanized 8 weeks after stent placement.
Gross and scanning electron microscopic findings
Gross inspection of the external surface of the stents revealed no perforation and all analyzed stents were visually patent. In both the CS and CE-CSEMS groups, white to yellowish amorphous materials (biofilm) were observed on the inner surface of the polymeric membrane. However, no food materials were observed in the stents.
SEM examination of all stents showed biofilms, of relatively uniform thickness (range, 2–7μm) on the inner surface of the polymeric membranes, with most of the bio-films closely bound to the polymeric membranes (Fig. 5). Both CS and CE-CSEMS showed similar biofilm structures, consisting of coccoid or rod-shaped micro-organisms and colonies. The colonies varied in size, from approximately 1–5 μm, but there was no between group difference in the degree of biofilm, either by gross inspection or SEM. Severe biofilm formation was observed in two stents in the CS group and one of the CE-CSEMS-20 group. Moderate biofilm formation was observed in one stent of the CS group, all three of the CE-CSEMS-10 group, and two stents of the CE-CSEMS-20 group (Table 1; Fig. 6).
Scanning electron microscopic view of the covering membrane of CE-CSEMS-20-9, showing biofilms of relatively uniform thickness (range, 3.5-7 μm) on inner surface of the polymeric membrane (*). The biofilms were closely bound to the polymeric membrane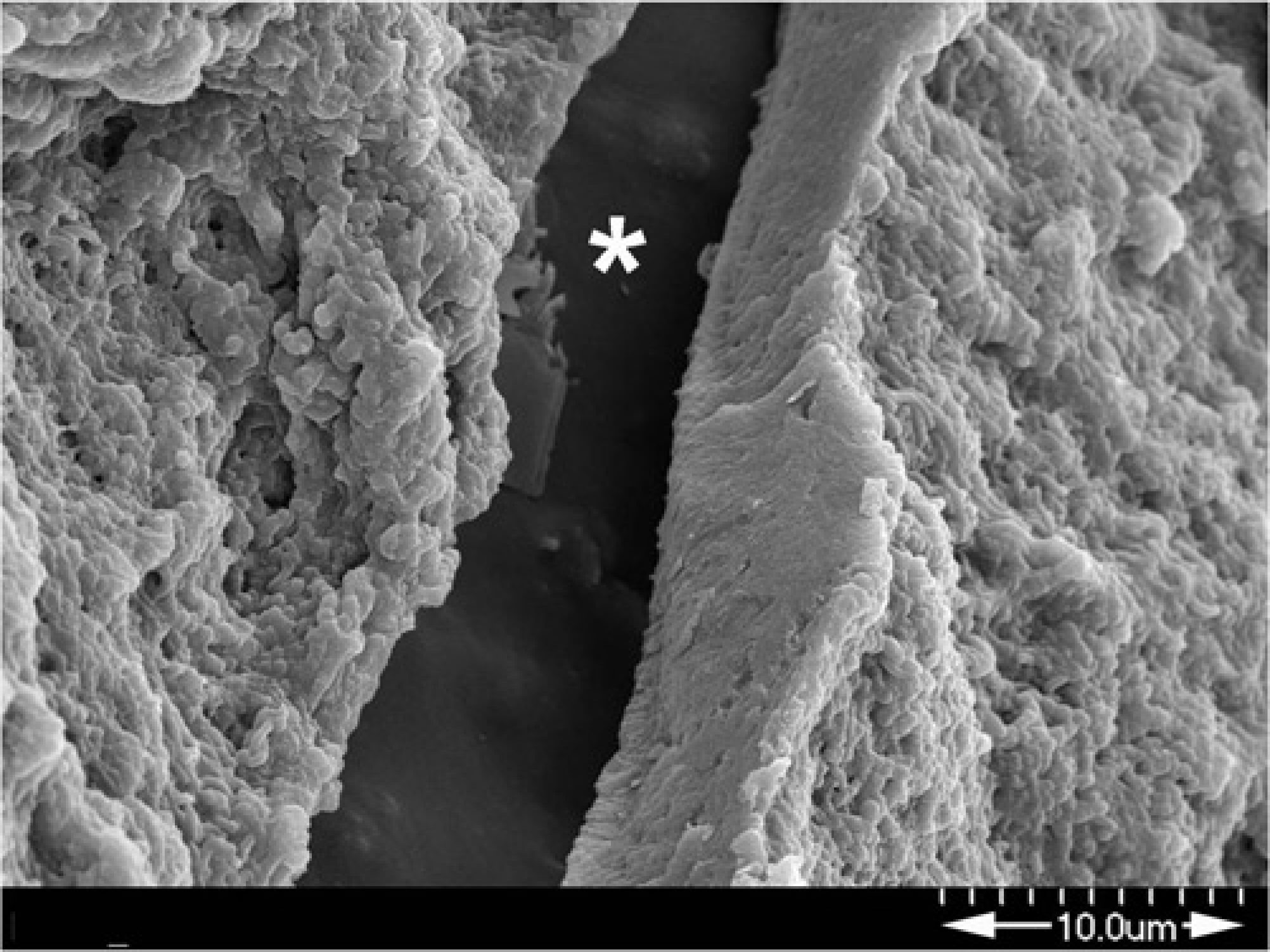
Scanning electron microscopic images of the covering membranes of CS and CE-CSEMS. (a) A CS showing an amorphous layer (biofilm) of relatively uniform thickness deposited on the covering membrane (original magnification, × 100); (b) ACS showing multiple colonies with rod-shaped micro-organisms (original magnification, × 5000); (c) ACE-CSEMS-10 showing an amorphous biofilm deposited on the covering membrane (original magnification, × 100). The dehydration procedures for sample caused cleavages (*) at the interface between the biofilms; (d) ACE-CSEMS-10 showing multiple round or ovoid-shaped colonies (original magnification, × 5000); (e) ACE-CSEMS-20 showing an amorphous biofilm deposited on the covering membrane (original magnification, × 100); (f) A CE-CSEMS-20 showing multiple round-shaped colonies of variable size (original magnification, × 5000)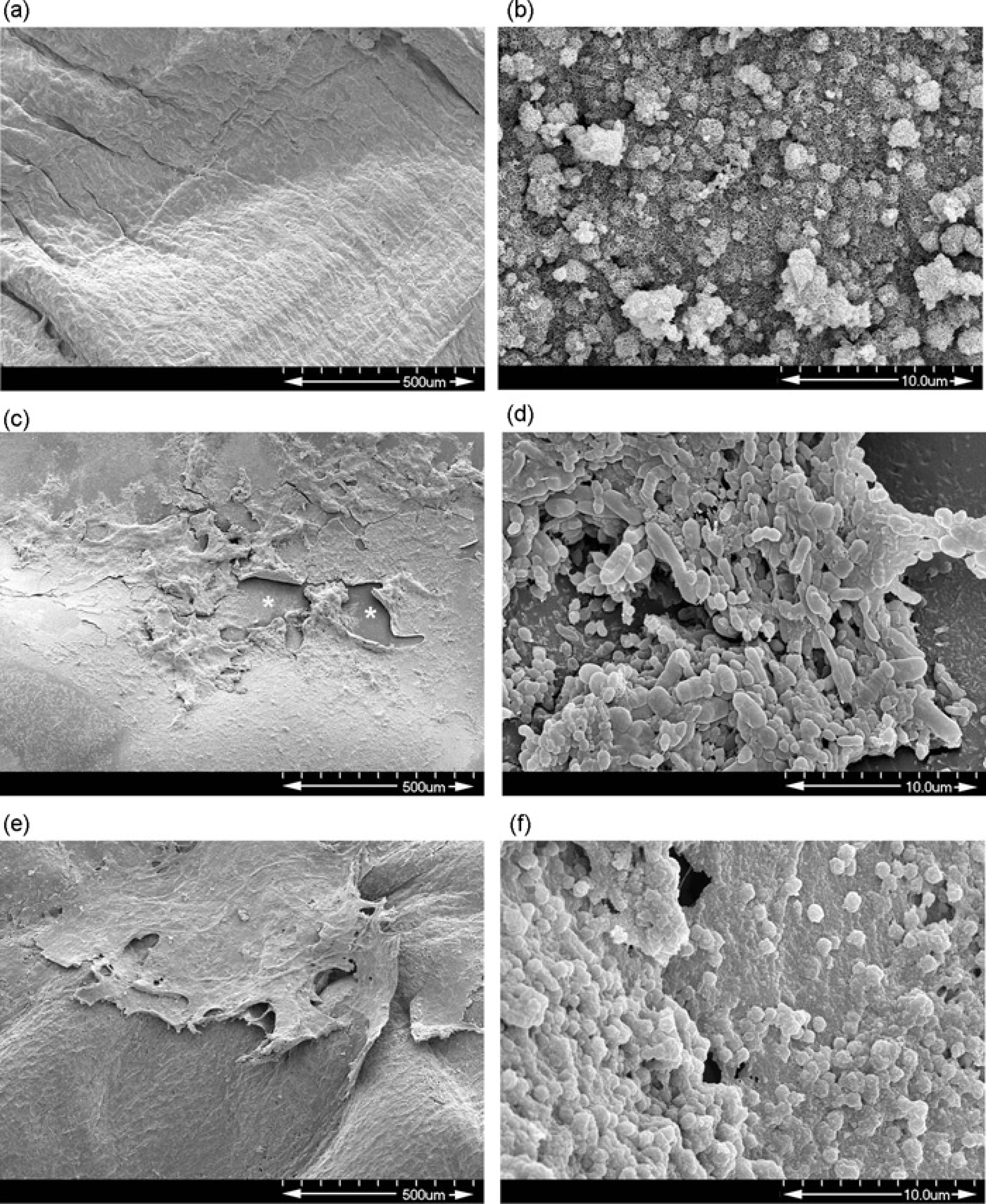
Scanning electron microscopic findings of the nine stents

CE-CSEMS, cefotaxime-eluting covered self-expandable metallic stent; CS, control stent
Discussion
Stent occlusion induced by the deposition of biliary sludge – composed of cholesterol crystals, calcium bilirubinate and palmitate, cholesterol, bacteria and/or fungi, microbial byproducts, proteins, dietary fibers, and glyco-proteins – is a major cause of stent malfunction (20–22). The biochemical activities of bacterial enzymes in the biofilm growing on the inner surface of the stents cause bile sludge deposition, followed by sludge accumulation within the biliary stent and stent occlusion. Since, in bio-films, living bacteria are usually surrounded by extracellular matrix and dead bacteria, antimicrobials may not fully penetrate a biofilm (20,22,25). To prevent complications and improve the effectiveness of biliary stents, especially when placed above the ampulla, it is crucial to control bacterial infection before biofilm develops on the inner surface of stents. This has led to the evaluation of antimicrobial agents effective in preventing bacterial attachment and biofilm formation (25–28). For example, perfusion of polyethylene and silicone-covered stents with ampicillin-sulbactam prevented bacterial adherence and biofilm formation, thereby prolonging stent patency (26,27). However, a prospective randomized study, comparing patients treated with polyethylene stents, with or without long-term prophylactic protection with ciprofloxacin, showed no differences in stent patency (29). To date, no agents have proven satisfactory in animal or clinical studies.
Our in-vitro experiments showed that cefotaxime was rapidly released from the CE-CSEMS immediately after deployment, with low levels of cefotaxime released over the next several weeks. We therefore hypothesized that the released antibiotic may kill micro-organisms before biofilm development. Although CE-CSEMS could be safely implanted in the normal canine bile duct, these stents did not prevent biofilm development, with no differences observed in degree of the biofilm formation among the three stent groups. Because sludge formation may also be caused by the reflux of intestinal contents into stents, we inserted all stents above the papilla, and we did not observe any food materials in the stents after sacrifice. We therefore hypothesized that biofilm formation in these animals was caused primarily by microbial attachment to the surfaces of the stents.
Although we did not culture the micro-organisms, one possible reason for the inability of these covered stents to prevent biofilm formation may be due to multi-organism involvement in biofilm formation. In one study, biofilms may be colonized by a mixed microbial population, including aerobic and anaerobic bacteria and fungi (20). Thus, cefotaxime would be unable to prevent biofilm development. Another possible reason may be insufficient release of cefotaxime. The concentration of cefotaxime released may have been too low to kill the micro-organisms, and early release of cefotaxime from the membrane may have delayed microbial attachment. Further studies are therefore needed to select more appropriate antimicrobial agents. Furthermore, it is important to develop covering membranes that retain antimicrobial agents sufficiently to allow a steady, long-term release of these agents.
This study had several limitations. First, there were too few experimental animals to allow us to draw statistical conclusions. However, we were able to assess biofilm formation in each group. Second, we did not culture the microorganisms prior to fixation in formalin. However, we were able to utilize SEM to observe micro-organisms and colonies on the biofilms, enabling our evaluation of the efficacy of the CE-CSEMSs.
In conclusion, our finding that biofilm formation was similar in dogs implanted with CS and CE-CSEMS using two concentrations of cefotaxime, suggests that cefotaxime does not prevent biofilm development in biliary stents. Biofilm formation on the inner surface of biliary stents may be prevented by using broad-spectrum antimicrobial agents and stents that maintain a steady release of these agents for a long time, thus prolonging stent patency.
Footnotes
Acknowledgements
This work was supported by a grant (2010-372) from the Asan Institute for Life Sciences, Seoul, Korea.