
Abstract
Background
Gadoxetic acid and diffusion-weighted imaging (DWI) is increasingly used for the diagnosis of hepatocellular carcinoma (HCC). It is relevant to refine the diagnostic parameters for HCC, using state-of-the-art imaging techniques.
Purpose
To validate usefulness of magnetic resonance imaging (MRI) criteria with gadoxetic acid-enhanced MRI and DWI for diagnosis of small HCC by differentiation from dysplastic nodule (DN) or regenerative nodule (RN) in cirrhotic patients with strongly suspected small HCC.
Material and Methods
One hundred and eight patients with 102 HCCs and 29 benign nodules including 21 DNs and two large RNs (≤ 2.0 cm), and 40 patients with no HCC underwent gadoxetic acid-enhanced MRI and DWI. All patients also underwent MDCT. Index MR criteria for HCC were: (i) arterial hyperenhancement and hypointensity on hepatobiliary phase (HBP) with hyperintensity on DWI; (ii) hypovascular nodule with hyperintensity on DWI; (iii) arterial hyperenhancement and hypointensity on HBP without hyperintensity on DWI; (iv) arterial hyperenhancement and either iso- or hyperintensity on HBP, with hyperintensity on DWI; and (v) hyperintensity only on DWI. According to these criteria, MRI findings for HCCs and benign nodules were independently classified by two reviewers.
Results
On multidetector-row computed tomography, 64 HCCs (62.7%) showed typical features for HCC while 13 (12.8%) were not identified. On MRI, 84 HCCs (82.4%) showed arterial hyperenhancement and hypointensity on HBP, and hyperintensity on DWI. Eight HCCs were regarded as hypovascular HCCs with hyperintensity DWI (category 2). One HCC (0.6 cm in diameter) was demonstrated only by DWI. For each observer, 101 (99.0%) and 100 HCCs (98.0%) were discernible when applying all MRI criteria for HCC, respectively. Three DNs also fit the HCC criteria, thus the specificity was 90.9% for both observers.
Conclusion
With the HCC criteria based on combined gadoxetic acid-enhanced MRI and DWI, it is possible to reliably diagnose small HCC including hypovascular HCCs.
Keywords
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and is the third leading cause of cancer-related mortality worldwide. The incidence of HCC has markedly increased in recent decades, especially in Western countries (1). With the advances in curative therapies, including surgical treatment and locoregional treatment, the early stage of small HCC has the highest likelihood for cure (2, 3). Therefore, the importance of early detection of HCC is being emphasized.
Since most HCCs develop in patients with chronic liver disease, a surveillance program incorporating imaging modalities has become more important. In this context, non-invasive imaging criteria allowing diagnosis of HCCs based on their vascular profile have been proposed by study groups, such as the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD) (4, 5). However, with the currently available HCC criteria, a diagnosis of malignancy is achieved only for nodules
With the recent introduction of gadoxetic acid (Gd-EOB-DTPA; Primovist, Bayer Healthcare, Berlin, Germany) and diffusion-weighted imaging (DWI) in liver magnetic resonance imaging (MRI), MRI has the potential to improve both the detection and characterization of hepatic tumors. Gadoxetic acid is a dual-acting agent that has the characteristics of an extracellular agent during the early vascular-interstitial phases and that of liver-specific agent during the delayed phase (7-9). With the expanded use of gadoxetic acid in HCC work-up, the expectation has been raised that HCCs showing equivocal findings on dynamic computed tomography (CT) or MRI could be verified by aid of hepatobiliary phase image (HBP), as the prevalence of HCCs that are hypointense on HBP is higher than washout of HCC on conventional dynamic CT or MRI (10-15). DWI is drawing attention due to its peculiar capability to differentiate tissue based on cellular density and architectural change, irrespective of vascularization (16-19). Given that one of the major histological differences between a dysplastic nodule (DN) and early HCC is the degree of cellular density (20), introducing DWI into the gadoxetic acid-enhanced MRI protocol could be beneficial in the diagnosis of early stage HCCs that do not fit the currently available HCC criteria.
To date, only one study has assessed the efficacy of combined reading of gadoxetic acid-enhanced MRI and DWI in the diagnosis of HCC (15). Therefore, we conducted this study to validate the usefulness of the imaging criteria established by the combined gadoxetic acid-enhanced MRI and DWI in the diagnosis of HCCs with ≤ 2 cm in size, detected during surveillance in patients with chronic liver disease. This study was conducted in a viral hepatitis endemic Asian population at high risk of developing HCC.
Material and Methods
Patient selection
The institutional review board approved this retrospective study and waived the requirement for informed patient consent. Our institutional database was reviewed retrospectively for liver MRIs conducted on patients suspected of having HCC based on multidetector-row computed tomography (MDCT) or sonography performed at our tertiary referral hospital between April 2010 and August 2011. During this period, 2760 consecutively registered patients with chronic hepatitis or cirrhosis underwent liver MRI. Of these patients, those who met the following criteria were included: (i) patients with HCC or benign hepatocellular nodule (i.e. DN) ≤ 2.0 cm in diameter that had been proven by either surgical resection or biopsy; (ii) patients who underwent both multiphasic MDCT and liver MRI, including gadoxetic acid-enhanced imaging and DWI; and (iii) patients had not undergone treatment for HCC prior to the MR examination. One hundred and eight patients (87 men, 21 women; age range, 30-73 years; mean age, 56 years) who had a total of 102 HCCs and 21 DN or two large regenerative nodules (RNs) ≤ 2 cm (size range, 0.6-2.0 cm; mean, 1.3 cm) formed our study population. We also selected 40 consecutive subjects who had undergone liver MRI for HCC surveillance but had no identifiable HCCs as a control group. Six hemangiomas and four nodular-shaped arterioportal shunts were identified in 10 of the 40 control group patients (Fig. 1). Thus, finally, 148 patients (103 men, 45 women; age range, 30-73 years; mean age, 55 years) formed our study population.

Flowchart of patient inclusion
The diameter of HCCs ranged from 0.6 to 2.0 cm (mean, 1.3 cm), and benign nodules ranged from 0.6 cm to 2.0 cm (mean, 1.2 cm). Of 90 patients who had only HCCs, 82 patients had one solitary HCC each, six patients had two HCCs each, and two patients had three HCCs each. Of the 18 patients with benign hepatocellular nodules, two patients had both single HCC (≤ 2.0 cm) and one DN or two large RNs, respectively. The 14 patients had one DN each and two patients had three DN each with one HCC each (3.0 cm and 4.5 cm, respectively). Of 102 HCCs, eight lesions were grade I and the remaining 94 lesions were grade II, according to Edmondson's classification of HCC (21). One hundred and thirty-six patients had liver cirrhosis associated with viral hepatitis B and 12 patients had viral hepatitis C-induced liver cirrhosis. Based on the Child-Pugh classification, 141 patients were classified as Child-Pugh class A, five were class B, and the remaining two were classified class C. All patients had undergone four-phase MDCT as surveillance for HCC before the MRI examination. Table 1 summarizes the demographic and clinical characteristics of the study patients.
Patient and tumor characteristics
APS, arterioportal shunt; DN, dysplastic nodule; RN, regenerative nodule
The diagnosis of all HCCs, eight DN (five low-grade and three high-grade), and two large RNs were based on a histopathological examination of the surgical specimens. Diagnosis of remaining 13 DN (10 low-grade and three high-grade) was based on the results of sonography-guided percutaneous biopsy. The average time interval between the MRI examination and surgery or biopsy was 9 days (range, 2-15 days). The operation included segmentectomy (n
Imaging techniques
Multiphasic (unenhanced, arterial, portal venous, and equilibrium phases) CT was conducted with either a 40-MDCT scanner (Brilliance 40; Philips Healthcare, Best, The Netherlands), a 64-MDCT scanner (Aquilion 64; Toshiba Medical System, Tokyo, Japan or a LightSpeed VCT 64, GE Healthcare, Waukesha, WI, USA). The scanning parameters were 120 kVp, 189-200 mAs, 5-mm slice thickness with an increment (overlap) of 2.5 mm, table speed of 26.5-39.37 mm/rotation (pitch, 0.828-1.07), and a single-breath-hold helical acquisition of 4-6 s, depending on liver size. Hepatic arterial phase scanning began 30-40 s after the injection of 110 or 120 mL of the non-ionic iodinated contrast agent, iopamidol (Iopamiro 300, Bracco, Milan, Italy) at a rate of 3-4 mL/s, by means of a bolus-triggered technique (120 kVp; 40-60 mA; monitoring frequency from 12 s after the contrast injection, 1 s; trigger threshold, 100 HU in the descending aorta; delay from trigger to initiation of scan, 18 s). The portal and equilibrium phases of scanning began 70 s and 180 s after the injection of the contrast agent, respectively.
MRIs were acquired using a 3.0-T whole-body MR system (Intera Achieva 3.0-T; Philips Healthcare, Best, The Netherlands) with a 16-channel phased-array coil used as the receiver coil. MRI protocol included a respiratory triggered T1-weighted turbo field-echo in-phase and opposed sequence (TR/first echo TE, second echo TE, 10/ 2.3 [in-phase] and 3.45 [opposed-phase]; flip angle, 15°; matrix size, 256 × 194; bandwidth, 434.3 Hz/pixel); a breath-hold multishot T2-weighted sequence with an acceleration factor of 2 (1796/70; flip angle, 90°; matrix size, 324 × 235; bandwidth, 258.4 Hz/pixel), with a 5 mm section thickness and a field of view (FOV) of 32-38 cm. For gadoxetic acid-enhanced MRI, unenhanced, arterial-phase (20-35s), portal-phase (60s), late-phase (3 min) and 20-min delayed HBP images were obtained using a T1-weighted three-dimensional (3D) turbo-field-echo sequence (T1 high-resolution isotropic volume examination, THRIVE; Philips Healthcare) (3.1/1.5; flip angle, 10°; matrix size, 228 × 211; bandwidth, 724.1 Hz/ pixel), with a 2-mm section thickness and a FOV of 32-38 cm. The contrast agent was automatically administered intravenously at a rate of 1 mL/s for a dose of 0.025 mmol/kg body weight using a power injector, followed by a 20 mL saline flush. Diffusion-weighted single-shot echo planar imaging with the simultaneous use of respiratory triggering was performed using a TR/TE of 1600/70. The TR was matched in each patient to the length of the respiratory cycle prior to gadoxetic acid enhancement. The scanning parameters were b-value of 0, 100, and 800 s/mm; spectral presaturation with inversion recovery for fat suppression; matrix size, 100 × 100; acceleration factor of SENSE, 4.0; FOV, 35
Image analysis
To determine the imaging criteria for HCC with the combination of gadoxetic acid-enhanced MRI and DWI, the study coordinator and one radiologist reviewed all MRI scans for patients with HCCs or benign hepatocellular nodules to reach a consensus concerning the enhancement pattern on the gadoxetic acid-enhanced MRI and presence of hyper-intensity on DWI (at b-values of 100 and 800). In addition, to assess the impact of diagnostic criteria using combined MRIs, as compared to conventional HCC criteria using MDCT, two radiologists also determined the enhancement pattern of HCCs and benign nodules on MDCT. After reviewing MRI features for 102 HCCs and 23 benign nodule, six categories were determined: (i) nodule displaying enhancement foci on the arterial phase image and hypointensity on HBP (with/without washout on portal venous phase or 3 min late phase), plus hyperintensity on DWI; (ii) nodule displaying either iso- or hypointensity on the arterial phase image and hypointensity on HBP, plus hyperintensity on DWI; (iii) nodule displaying enhancement foci on the arterial phase image and hypointensity on HBP (with/without washout on portal venous phase or 3 min late phase), with no hyperintensity on DWI; (iv) nodule displaying hyperintensity on the arterial phase image and iso- or hyperintensity on HBP, plus hyperintensity on DWI; (v) nodule displaying hyperintensity on DWI, but not on gadoxetic acid-enhanced MRI; and (vi) nodule depicted as hypointense only on HBP. According to these categories, the MRI findings for both HCCs and benign hepatocellular nodules were stratified by two independent radiologists with 5 and 11 years of experience in the interpretation of liver MRI in their daily practices. All MRIs were reviewed independently and separately by the two radiologists, who were blinded to the patients’ history and the final diagnosis. We did not consider the ADC value as a diagnostic criterion because most of benign hepatocellular nodules were not depicted on DWI.
Statistical analysis
On the basis of the reviews submitted by the two observers, the sensitivity and specificity of MRI for diagnosing HCCs was calculated for each observer. The sensitivity for each image set was calculated according to the number of lesions assigned a category of 1–5 among the 102 HCCs. To provide a range of plausible sensitivity differences, the 95% confidence intervals (CIs) were also calculated (22). The kappa statistic for multiple observers was calculated to assess the inter-observer agreement for the stratification of lesions (23). Kappa values < 0.20 indicated positive but poor agreement, 0.21–0.40 indicated fair agreement, 0.41–0.60 indicated moderate agreement, 0.61–0.80 indicated good agreement, and > 0.81 indicated excellent agreement. All statistical analysis was conducted using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Signal intensities of HCCs and benign hepatocellular nodules
The distribution of HCCs and benign hepatocellular nodules according to the MRI features are summarized in Table 2. Of the 102 HCCs, 84 lesions (82.4%) showed hyper-enhancement on the arterial phase image, hypointensity on HBP and hyperintensity on DWI (Fig. 2) (category 1). Eight HCCs were considered as hypovascular HCC as they were seen as either iso- (i = 4) or hypointense (n = 4) on the arterial phase, hypointense on HBP, and hyperintense on DWI (Fig. 3) (category 2). Six HCCs were not evident on DWI, but were seen as arterially enhancing nodules with hypointensity on HBP (category 3). All six lesions were found in four patients who were classified as Child-Pugh class B (n = 2) or C (n = 2). Three HCCs were seen as arterially enhancing nodules with either isointensity (n = 2) or hyperintensity (n = 1) on HBP and hyperintensity on DWI (Fig. 4) (category 4). The remaining HCC (0.6 cm in diameter) was demonstrated only on DWI, but was not seen on any gadoxetic acid-enhanced MRI (category 5). On T2-weighted imaging, 93 HCCs were definitively hyper-intense (n = 82, 80.4%) or faint hyperintense (n = 11, 10.8%), and all were also demonstrated on DWI. We found no cases that were not seen on DWI but were demonstrated on T2-weighted imaging.
Categorization of hepatocellular carcinomas (HCCs) and benign hepatocellular nodules according to the findings on gadoxetic acid-enhanced MRI and DWI
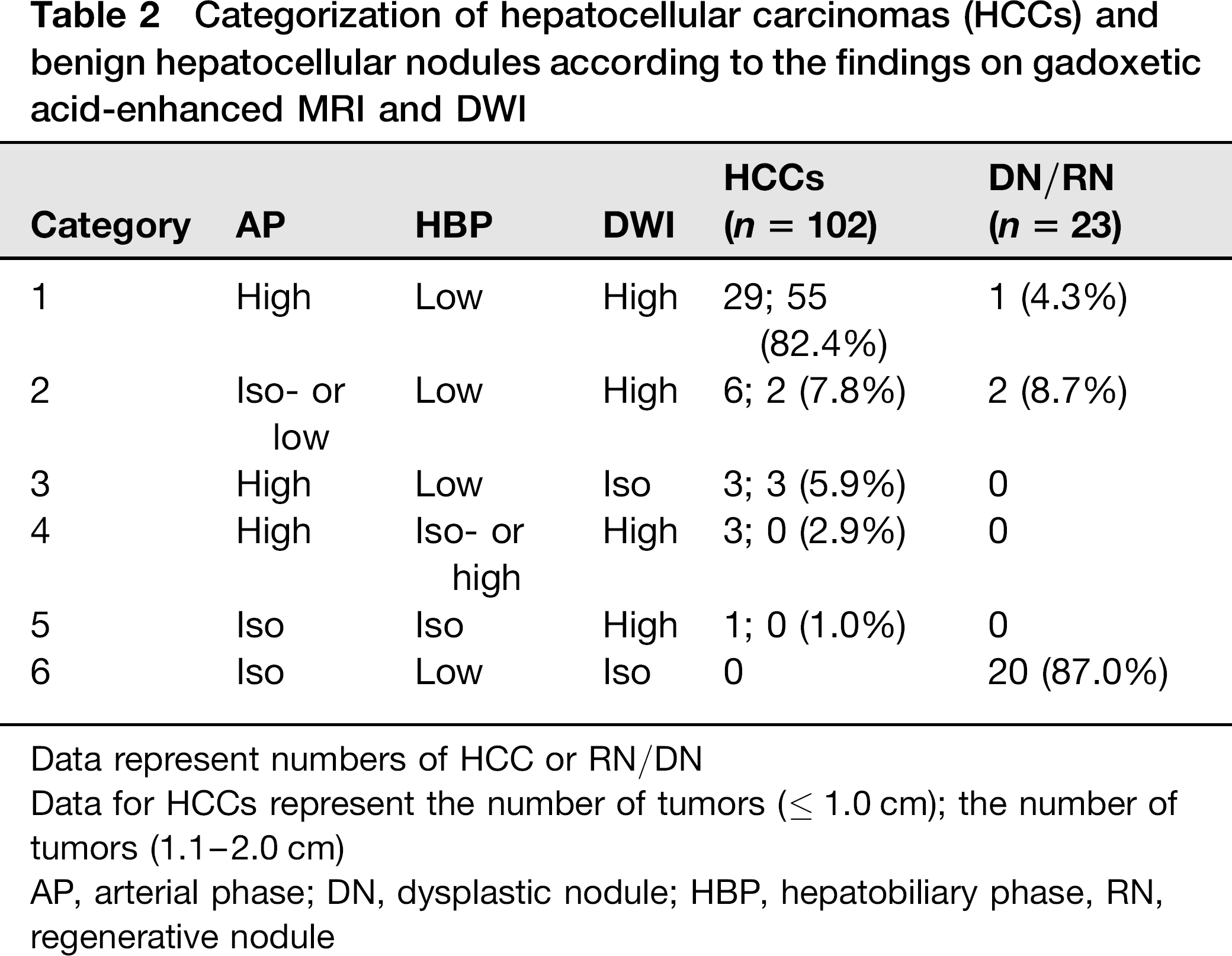
Data represent numbers of HCC or RN/DN
Data for HCCs represent the number of tumors (≤ 1.0 cm); the number of tumors (1.1-2.0 cm)
AP, arterial phase; DN, dysplastic nodule; HBP, hepatobiliary phase, RN, regenerative nodule

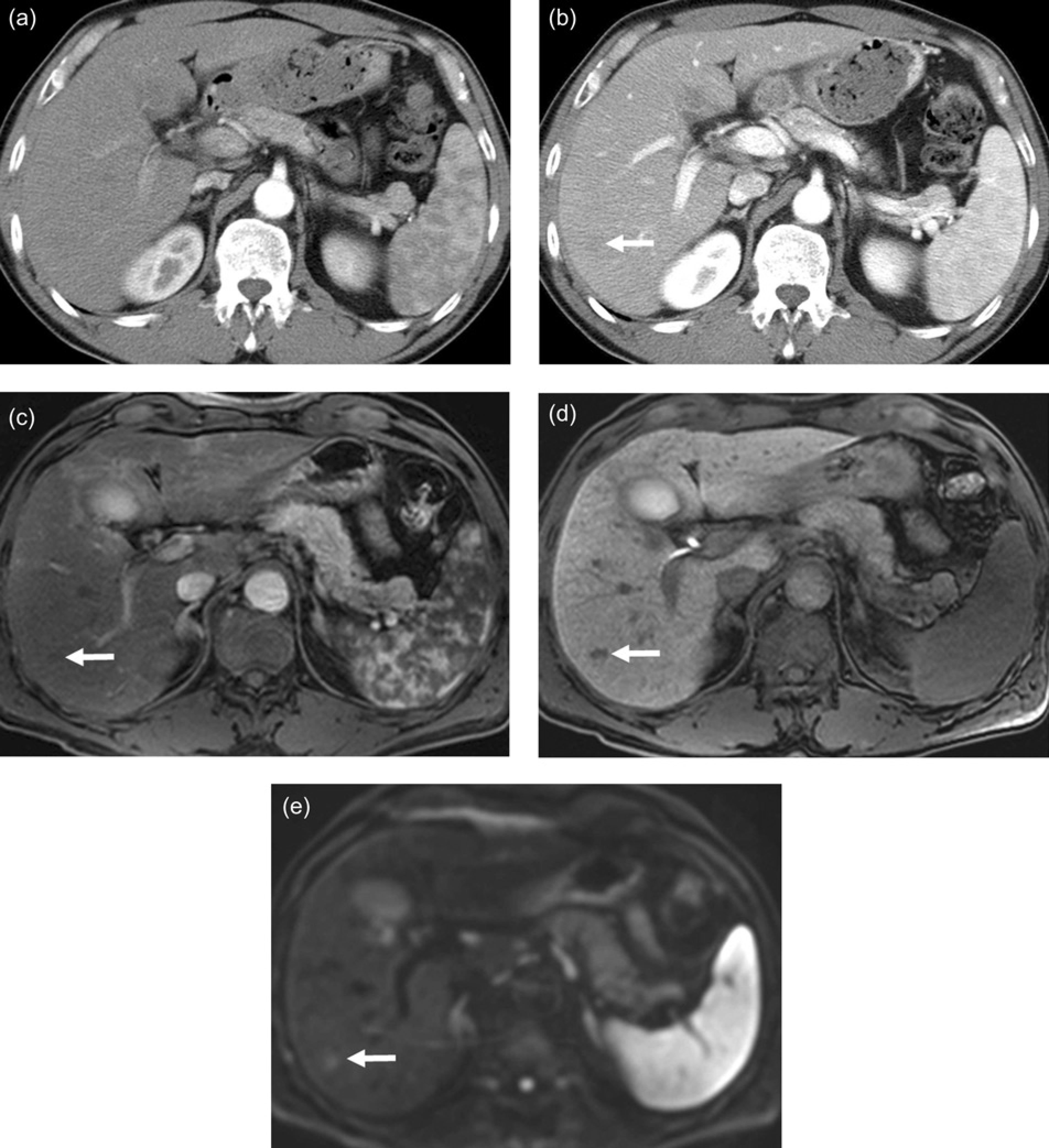
Surgically confirmed hepatocellular carcinoma in a 62-year-old woman. The arterial phase of multidetector row CT (a) shows nodular enhancement (arrow) in segment IV; however, equilibrium phase image (b) shows no washout. The axial arterial phase (c) and hepatobiliary phase image (d) 20 min after administration of gadoxetic acid shows definitive arterial hypervascularization of tumor (arrow) and hypointensity (arrow), respectively. (e) On axial single-shot echo-planar diffusion weighed imaging at b = 800 s/mm2, the tumor is clearly seen as hyperintense (arrow)
Surgically confirmed hepatocellular carcinoma in a 55-year-old man. The axial arterial phase (a) and portal phase image (b) of multidetector row CT shows subtle low attenuation (arrow) without arterial enhancement. The axial arterial phase (c) and hepatobiliary phase image (d) 20 min after administration of gadoxetic acid show small hypointense mass (arrows). (e) On axial single-shot echo-planar diffusion weighed imaging at b = 800 s/mm2, small nodule is seen as hyperintense (arrow)
Surgically confirmed hepatocellular carcinoma in a 55-year-old man. On the axial arterial phase (a) and hepatobiliary phase image (b) 20 min after administration of gadoxetic acid, the tumor displays faint arterial hypervascularization and hyperintensity, respectively (arrows). (c) On the axial single-shot echo-planar diffusion-weighted imaging at b = 100 s/mm2, tumor is seen as hyperintense (arrow)
Out of 23 benign cirrhosis-associated hepatocellular nodules, 20 lesions were hypointense only on HBP, but were not depicted on other images, including arterial phase and DWI. However, two high-grade DN were rated as category 2, as they were seen as either iso- or hypointense on arterial phase and hypointense on HBP, with hyper-intensity on DWI. The remaining one high-grade DN (1.0 cm in diameter) was rated as category 1, as it showed arterial hyperenhancement and subtle hypointensity on HBP, as well as hyperintensity on DWI (Fig. 5). All hemangiomas and arterioportal shunts showed their typical imaging features as centripetal enhancement for hemangioma and arterially only enhancing nodules without signal intensity changes on other imaging for arterial portal shunts.

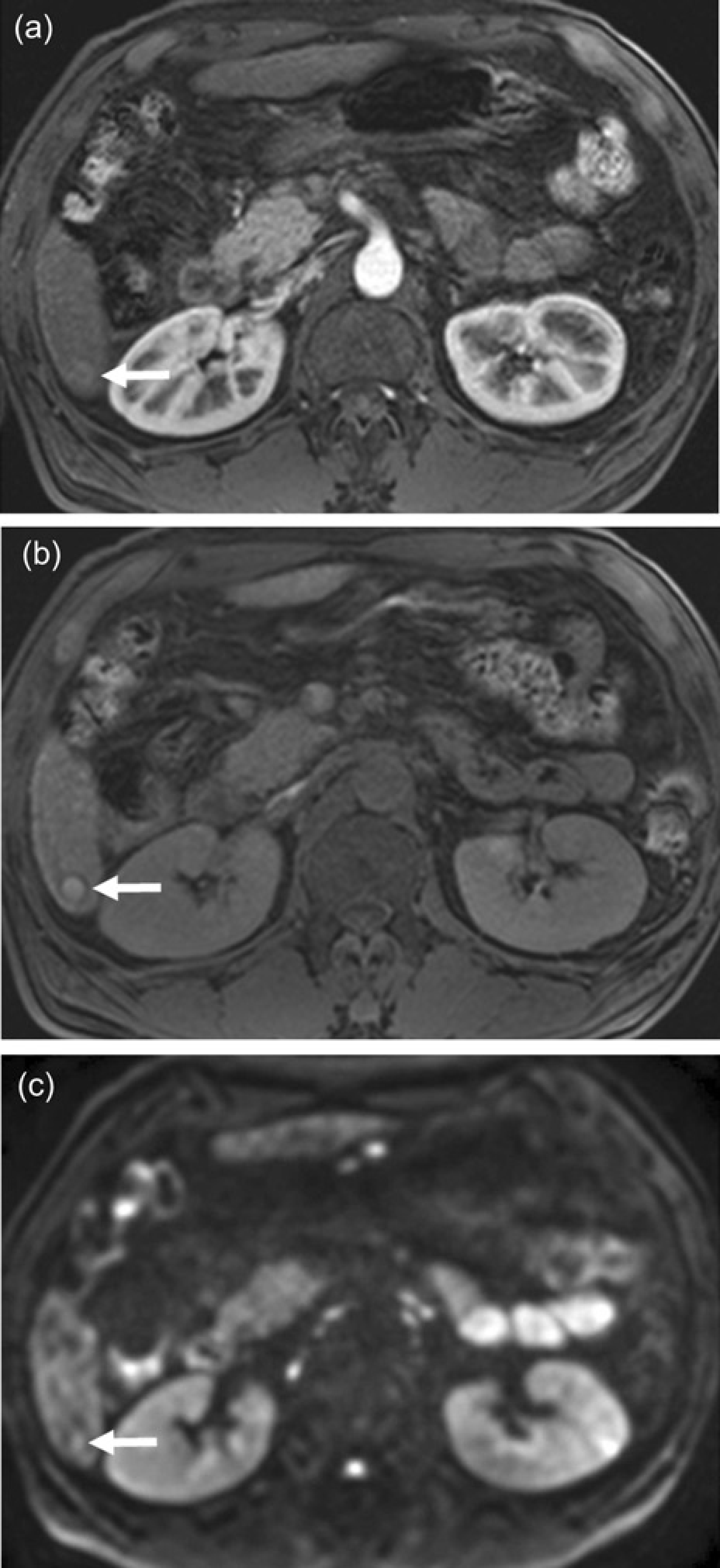
Surgically confirmed high-grade dysplastic nodule in a 56-year-old woman. The axial arterial phase (a) and hepatobiliary phase image (b) 20 min after administration of gadoxetic acid shows definitive arterial hypervascularization of tumor (arrow) and hypointensity (arrow), respectively. (c) On the axial single-shot echo-planar diffusion-weighted imaging at b = 800 s/mm2, nodule is seen as hyperintense (arrow)
Inter-observer agreement
The kappa values for the two observers were 0.904 for categorizing HCC and benign nodules, indicating excellent inter-observer agreement with MRI findings. Six HCCs were found to be mismatched between two observers in the lesion stratification according to the six categories proposed. Three lesions were assigned as category 1 by one reviewer and as category 3 by the other. Three more lesions were assigned as category 1 by one reviewer and as category 2 by the other reviewer.
Sensitivity and specificity for diagnosing HCC
When categories 1 to 5 were used as the criteria for diagnosing HCCs, among the 102 HCCs, 101 (sensitivity, 99.0%; 95% CI, 93.8–99.9%) were clearly discerned by observer 1 and 100 (sensitivity, 98.0%; 95% CI, 92.4–99.7%) were discernible by observer 2 (Table 3). For both observers, tiny HCCs (0.6 cm in diameter) assigned as category 5 was overlooked, as they showed subtle hyperintensity only on DWI, but were not evident in the other images. Three DNs were also classified as category 2 or 1, representing a specificity of 90.9% (95% CI, 74.5–97.6%) for both observers when categories 1 to 5 were used for the criteria for diagnosing HCC. In 40 control patients with no HCC, there were no false-positives by either observer.
Sensitivities and specificity for diagnosing 102 hepatocellular carcinoma with the combination of gadoxetic acid-enhanced MRI and DWI

Numbers in parentheses and brackets represent the number of true-positive lesions and false-positive lesions, respectively
Correlation between MRI categorization and the enhancement pattern on MDCT
Table 4 summarizes the enhancement patterns of HCCs on MDCT, with relation to the MRI category. Of 102 HCCs, 64 HCCs (62.7%) showed arterial hyperenhancement and washout on MDCT. Among them, 55 HCCs (53.9%) were >1.0 cm in diameter. Seventeen and eight HCCs were seen as arterially only enhancing nodules (16.7%) and hypovascular nodules (7.8%), respectively. Thirteen HCCs (12.8%) were not identified on MDCT. Of 23 benign hepatocellular nodules, one high-grade DN showed arterial enhancement and suspicious low attenuation on equilibrium phase of MDCT, whereas the others were apparent as low attenuated nodules on portal venous and/or equilibrium phase (n = 13) and were not depicted on MDCT (n
Enhancement patterns of hepatocellular carcinomas on MDCT with relation to MR categories
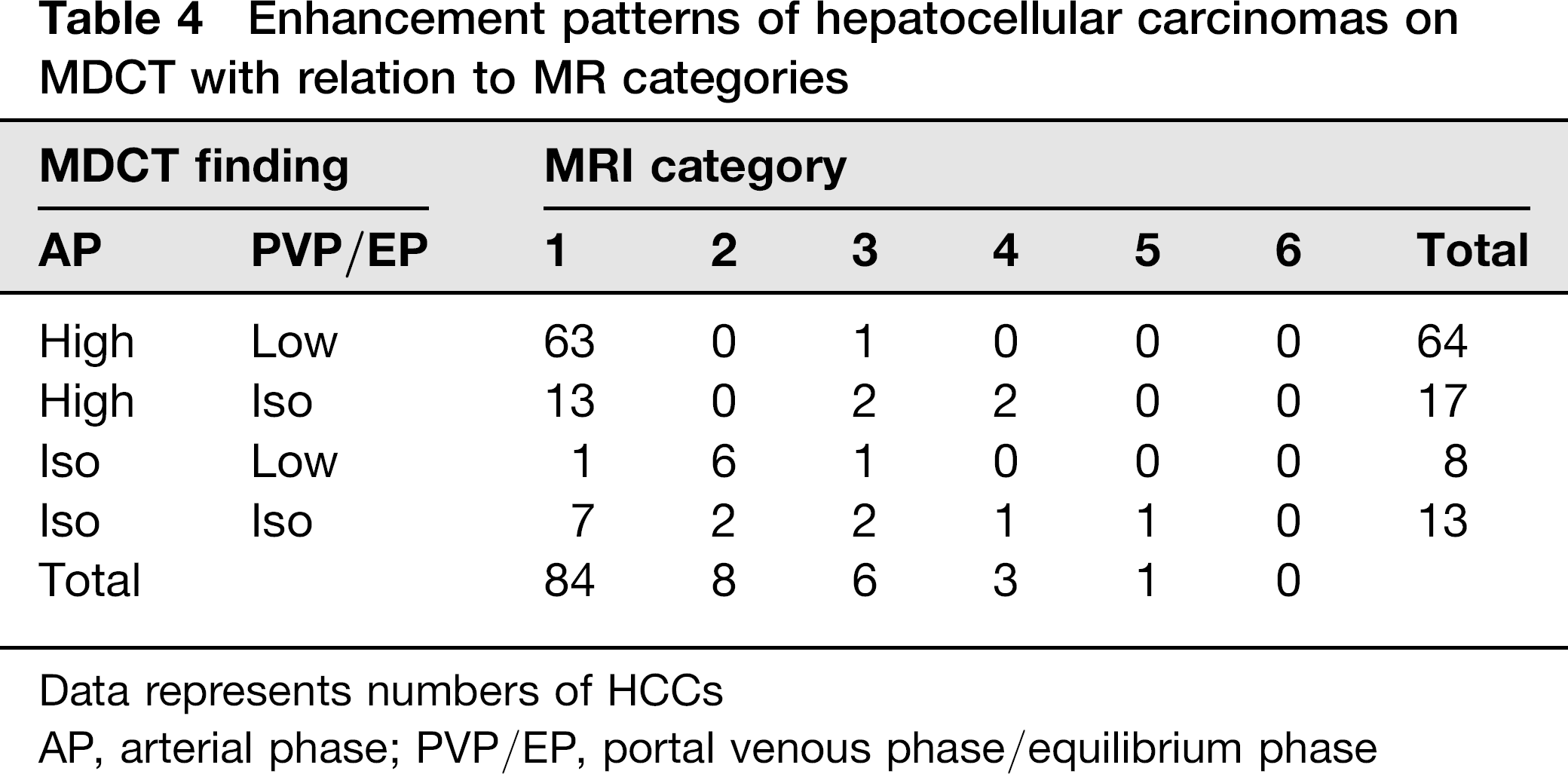
Data represents numbers of HCCs
AP, arterial phase; PVP/EP, portal venous phase/equilibrium phase
Discussion
In the current study, we recruited a cohort of patients with chronic viral hepatitis or cirrhosis who were suspected of having hepatic nodules ≤ 2 cm on MDCT or sonography performed as surveillance, and who underwent liver MRI. The study samples included HCCs and cirrhosis-associated benign hepatocellular nodules confirmed histologically, hemangiomas, and nodular arterioportal shunts. Nodules arising in patients who had a history of HCC were not included. With regard to the stratification of lesions, excellent inter-observer agreement was demonstrated, with 101 of 102 HCCs discernible by observer 1 and 100 of 102 HCCs discernible by observer 2, when using MRI category 1-5 as the criteria for HCC. This implies the reproducibility of the approach.
In our series, the prevalence of HCCs fitting the AASLD diagnostic criteria based on MDCT was 53.9%, which is similar to previous reports showing that 33-61% of HCCs
It is noteworthy that lesions showing equivocal findings on gadoxetic acid-enhanced MRI as being hypovascular hypointense nodule or arterially only enhancing nodules could be diagnosed as HCC when they showed hyperintensity on DWI (categories 2 and 4). This finding agrees closely with a prior report (27), in which arterial hypervascularization on conventional gadolinium-enhanced image and hyperintensity on DWI was proposed as a HCC criterion. However, unlike the equilibrium phase using an extracellular agent, the enhancement of tumors on HBP was not related with the hemodynamic characteristics. In our series, three HCCs showed both arterial hypervascularization and iso- (n = 2) or hyperintensity (n = 1) on HBP, probably owing to remnant hepatocyte activity in the tumors, while showing hyperintensity on DWI. However, in theory, DN might show arterial hypervascularization and enhancement on HBP, owing to their unpaired artery and their hepatocyte function, respectively (28, 29). Therefore, we expected that the addition of hyperintensity on DWI to the gadoxetic acid-enhanced MRI could be a guideline in differentiating between HCCs and DNs. Presently, 86 HCCs (84.3%) showed hyperintensity on DWI, whereas only three DNs (13.0%) showed this feature. Thus, it is reasonable to assume that hyperintensity on DWI is highly indicative of HCC in patients with chronic hepatitis or cirrhosis (27). One HCC was depicted only on DWI, but not on other sequences. Thus, given that DWI provides the high lesion-liver contrast, adding DWI to routine protocol of gadoxetic acid-enhanced MRI could be beneficial in characterizing equivocal hepatocellular lesions as well as HCC detection.
Although gadoxetic acid readily enables the delineation of hypovascular HCC as hypointense on HBP, it is challenging to differentiate HCC from benign hepatocellular nodules (i.e. DN) (10, 12, 14). Presently, eight HCCs were regarded as hypovascular HCCs and all showed hyperintensity on DWI (category 2). However, of 23 benign hepato-cellular nodules seen as hypointense on gadoxetic acid-enhanced MRI, two high-grade DNs fitted into category 2, as they also showed hyperintensity on DWI. Furthermore, one high-grade DN showed arterial hypervascularization and subtle hypointensity on HBP, as well as hyperintensity on DWI (category 1). Thus, when categories 1–5 were used as HCC criteria, the specificity were 90.9% for both observers. In consideration of diagnostic criteria that ensure improvement in sensitivity while maintaining high specificity, particularity in the setting of liver transplantation, our proposed criteria might not be satisfactory. However, high-grade DNs are considered as pre-malignant lesion and in some institutions they are subject to treatment (6). In view of this, current criteria might lead to the diagnosis of both HCC and high-risk nodules, as well. Precise histopathologic differentiation between DN and early HCC is still difficult as high-grade DN might have unpaired arteries, as does HCC, and their cellular density is nearly identical to that of early HCC (20). Thus, it is difficult to distinguish between high-grade DN and HCCs, even using MRI with multiparametric data.
Our study had several limitations. First, the retrospective study design might have caused a selection bias with regard to the initial imaging referrals because most liver MRIs were acquired in patients suspected of having liver nodules on MDCT performed as surveillance. Therefore, lesions not apparent on MDCT might have been under-represented in our study. As such, the reviewers might be sensitized to considering diagnosis of HCC. These might have resulted in an overestimation of the actual sensitivity of MRI. However, the objective of our study was not to determine the absolute sensitivity of liver MRI for diagnosing HCC. Second, in consideration of radiation hazard and contrast-induced nephropathy (30), we used relatively thick image slices and smaller volume of contrast medium for MDCT. This might have led to lower detection of HCC. However, the present detection rate for small HCC with MDCT was similar to those of previous reports (6, 24, 25). Third, we included only HCC, DN, large RN, and hemangioma ≤ 2.0 cm in size. Thus, the data could not distinguish HCC from other hypervascular hepatic lesions. Fourth, most patients were classified as Child-Pugh class A. It is uncertain whether our criteria could be available in patients with Child-Pugh class B or C. In our series, six HCCs were not depicted on DWI and all were found in four patients, classified as Child-Pugh class B or C. The background cirrhotic liver could show restricted diffusion, which makes it difficult to identify the HCC in the severe cirrhotic liver, compared to non-cirrhotic or mild cirrhotic liver (31). Fifth, we did not perform another separate reviewing session to determine the detect-ability of gadoxetic acid-enhanced early dynamic imaging including arterial, portal venous, and 3-min late phase. However, as was mentioned, our study could not determine the efficacy of gadolinium-enhanced early dynamic images relative to new MRI criteria for diagnosis of HCC because gadoxetic acid uptake in hepatocytes occurs about 1 min after the administration of the contrast medium (26). Finally, large numbers of the included HCCs were ≤1 cm in size. To date, it has not yet been determined whether a much earlier diagnosis of HCC could lead to a better outcome.
In conclusion, with the diagnostic parameters for HCC based on combined gadoxetic acid-enhanced MRI and DWI, it is possible to reliably diagnose small HCCs ≤ 2.0 cm in size including hypovascular HCC in patients strongly suspected of small HCC based on MDCT. However, the results of our study provide no data about the absolute sensitivity of liver MRI for detecting HCC or its relative efficacy to MDCT due to selection bias.