
Abstract
Background
The diagnosis of post-traumatic spinal cerebrospinal fluid (CSF) fistulae due to dural tears or lesions remains a challenge. Thus far, CT myelography is the standard test used to diagnose these complications.
Purpose
To evaluate the diagnostic ability of gadolinium-enhanced MR cisternography/myelography (intrathecal gadopentate dimeglumine or Gd-DTPA) in small animals that had experienced accidental spinal trauma.
Material and Methods
Four dogs and one cat suffered traumatic accidents resulting in neurological deficits underwent spinal MRI with intrathecal Gd-DTPA after routine plain films and MR images.
Results
T2-weighted SE images showed high water content in the epidural space or in the surroundings of the vertebrae in four animals. MR myelography revealed CSF leakage in all of them. In two animals CSF leaks were observed exuding from the spinal canal and tracking towards adjacent loose fat and interfascial planes. In two other animals Gd-DTPA extravasation was diffusely collected in paraspinal tissues around the vertebral arch. In the fifth animal a focal pseudomeningocele was observed adjacent to the traumatized region.
Conclusion
Intrathecal administration of Gd-DTPA is an effective method to reveal and confirm post-traumatic spinal CSF fistulae or other dural lesions in animals with potential application in humans.
The diagnosis of spinal cerebrospinal fluid (CSF) fistulae secondary to dural tears, rents, or lacerations, whether spontaneous or post-traumatic remains a diagnostic challenge in both humans and animals. In the spinal trauma setting, the detection of spinal dural tears is important because such defects can acutely entrap nerve roots. In addition, dural tears increase the risk of meningitis, which can cause a dural laceration and promote its remaining opening indefinitely, which may in turn lead to the development of post-traumatic meningocele. The meningocele itself then has the potential to act as a chronic focus for nerve root entrapment (1–3). However, dural tears and lacerations are clinically and radiologically very difficult to diagnose.
Intrathecal administration of paramagnetic compounds in magnetic resonance imaging (MRI) provides a potential opportunity to diagnose challenging CSF-related pathologies (4–6).
The purpose of this report is to review our experience with the use of intrathecally administered gadopentate dimeglumine (Gadolinium (III)-diethylene-triamine pentaacetic acid, or Gd-DTPA) in MRI in small animals that have experienced mild or severe spinal trauma, and to demonstrate its value in the diagnosis of traumatic dural tears. In light of our findings, we will discuss the pathophysiological mechanisms underlying CSF leaks, and display the information gathered from these series. Finally, we will attempt to predict potential applications for this examination in humans.
Material and Methods
Clinical and radiological findings
D-T2-HST, diffuse T2-hyperintensity on ventral paravertebral soft tissue; DSHC, domestic short-haired cat; F, female; L, left; LS, lumbosacral; N, no; M, male; R, right; R/O, ruled out; Y, yes
Animals' characteristics, clinical status, and radiological findings are presented in Table 1. The animals included in the study were four adult dogs and one adult cat. Traumatic spinal injury was caused by falls from heights (n = 2), by being run over by a car (n = 2), or by injury inflicted by another dog (n = 1). All fractures were categorized as closed fractures. The elapsed time between injury and radiological assessment ranged from 48 h to 2 weeks. Clinically, all animals presented with paraparesis or paraplegia; the remaining animal presented with cauda equina syndrome.
Plain films were obtained in all cases as the initial step of radiological studies. MRI of the animals was performed under general anesthesia which was induced with propofol (6 mg/kg body weight) and maintained with isofluorolane until the end of the procedure. The study was performed using a superconducting 0.5-T system (Gyroscan, Philips, Best, The Netherlands).
Our standard protocol included T2-weighted FSE (4000/110/16; TR/TE/echo train) images in the sagittal and transverse planes, as well as T1-weighted SE images (500/14; TR/TE). Intravenous (i.v.) Gd-DTPA was administered to two animals (cases 2 and 5) at a dose of 0.1 mmol/kg, and T1-weighted images were acquired in the transverse plane. Slice thickness/gap, field of view (FOV), and pixel resolution differed depending on animal size and the sequence performed. Standard sagittal FSE T2-weighted and SE T1-weighted sequences were usually performed with an FOV ranging from 320 to 300 and a slice thickness of 4–5 mm/0.4 (gap). Axial FSE T2-weighted and SE T1-weighted sequences were usually performed with an FOV ranging from 150 to 100 and a slice thickness of 4–5 mm/0.4 (gap). After the injection of intrathecal contrast material we always acquired transverse and sagittal T1-weighted sequences using the fat saturation technique. No fat-saturated T1-weighted sequences were previously acquired during the standard MRI procedure.
The procedure of intrathecal Gd-DTPA administration in veterinary medicine has been reported elsewhere (7). Briefly, after conventional MRI was conducted and under sterile conditions, an atlanto-occipital puncture was performed in the anesthetized animal and 1 mL of CSF was withdrawn. The CSF was then mixed with 0.2–0.5 mL of Gd-DTPA and re-injected via the same puncture.
Each animal was then positioned upright for 5–6 min so that diffusion of the contrast material throughout the entire subarachnoid space of the spine was maximized. Next, both sagittal and transverse T1-weighted and fat-saturated SE sequences were obtained, utilizing the same acquisition parameters as were previously used. No other sequences were acquired after the Gd injection.
Results
Plain films revealed either vertebral fractures and dislocations of varying severity, or no radiological abnormalities. Plain MR studies demonstrated intramedullary T2-hyperintense lesions related to the clinical findings in Cases 1, 2, 3, and 5 (Table 1). Medullary cord/nerve root compression promoted by acute disc/bony fragment compression were observed in two animals (Cases 1 and 4). In all but one case, additional diffuse T2-hyperintensities involving the paravertebral or interfacial soft tissue were identified adjacent to the bony lesions (Cases 2, 3, 4, and 5). In four animals, intrathecal administration of Gd-DTPA exhibited contrast agent extravasation from the spinal canal into the adjacent soft tissues. In two of these cases, the escape of contrast material was detected from a specific origin, because the contrast material followed a tracking course from the spinal canal towards the interfascial planes, soft tissues, and loose fat pads (Figs. 1 and 2). In animal 2, the final diagnosis consisted of a brachial plexus avulsion. Although no single leak was detected in the other two cases, we observed diffuse and extended contrast extravasation into soft tissues adjacent to injured vertebral arches (Figs. 3 and 4). In Case 2, the presence of prevertebral soft tissue thickening without an apparent connection to the spinal injury led us to suspect an inflammatory complication. Intravenous administration of Gd-DTPA revealed no soft tissue enhancement, thereby ruling out the presence of an abscess or phlegmon. The study accurately depicted the location and level of the CSF leak, and also precisely pinpointed the source of the outflow at the C7 and T1 right root sleeves, the course of the leak, and the region where the CSF accumulated. This information aided in the interpretation of the diffuse interfascial and intermuscular prevertebral hyperintensities identified on the T2-weighted images.
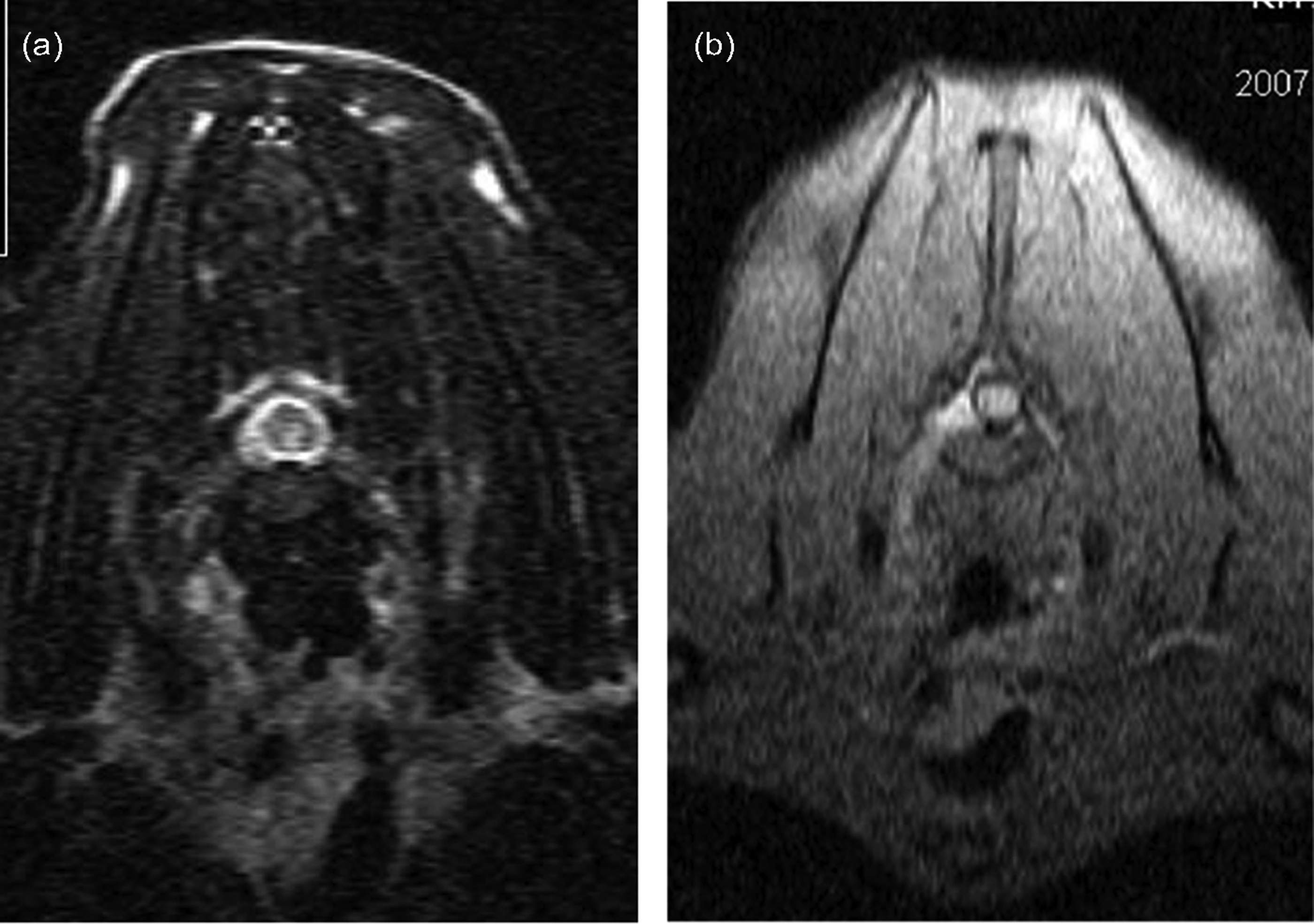
Case 3. (a) Sagittal T2-weighted image of the lumbar spine shows a distraction fracture of L4-L5 (arrow) with increased signal and changes in the morphology of the dorsal spinal muscles (arrowhead). (b) Transverse T2-weighted image at L4-L5 demonstrates a hyperintense intramedullary lesion and a diffuse T2-hyperintensity involving right dorsal paravertebral soft tissue (arrows). (c) Sagittal fat-saturated T1-weighted images after the intrathecal administration of Gd-DTPA display two different CSF leaks, one ventral and the other dorsal (arrows). These leaks originate from the vertebral arch content, course through the intervertebral disk, and finally reach the prevertebral tissues and posterior paraspinal muscles Case 2. (a) Transverse T2-weighted image at the C7-T1 intervertebral disc space shows a hyperintense intramedullary lesion. (b) Transverse fat-saturated T1-weighted image at the level of C7-T1 after intrathecal injection of Gd-DTPA demonstrates a hyperintensity tract, consistent with a CSF leak, coursing from the intervertebral foramen towards the ventral intermuscular region (reprinted with permission from reference 7) Case 4. Sagittal (a) and transverse (b) FSE T2-weighted images at the lumbosacral region (L7-S1 level) exhibit a lumbosacral compression fracture (arrow in (a)). (c) Transverse fat-saturated T1-weighted image at the same level as (b), after intrathecal administration of Gd-DTPA, demonstrates a large numbers of hyperintense leaks emerging from both sides of the spine (arrows), consistent with CSF leaks secondary to a dural tear Case 5. Axial fat-saturated T1-weighted image, taken after the intrathecal administration of Gd-DTPA, depicts a diffuse centrifugal CSF leakage (arrows) all around the spine, emerging from the vertebral arch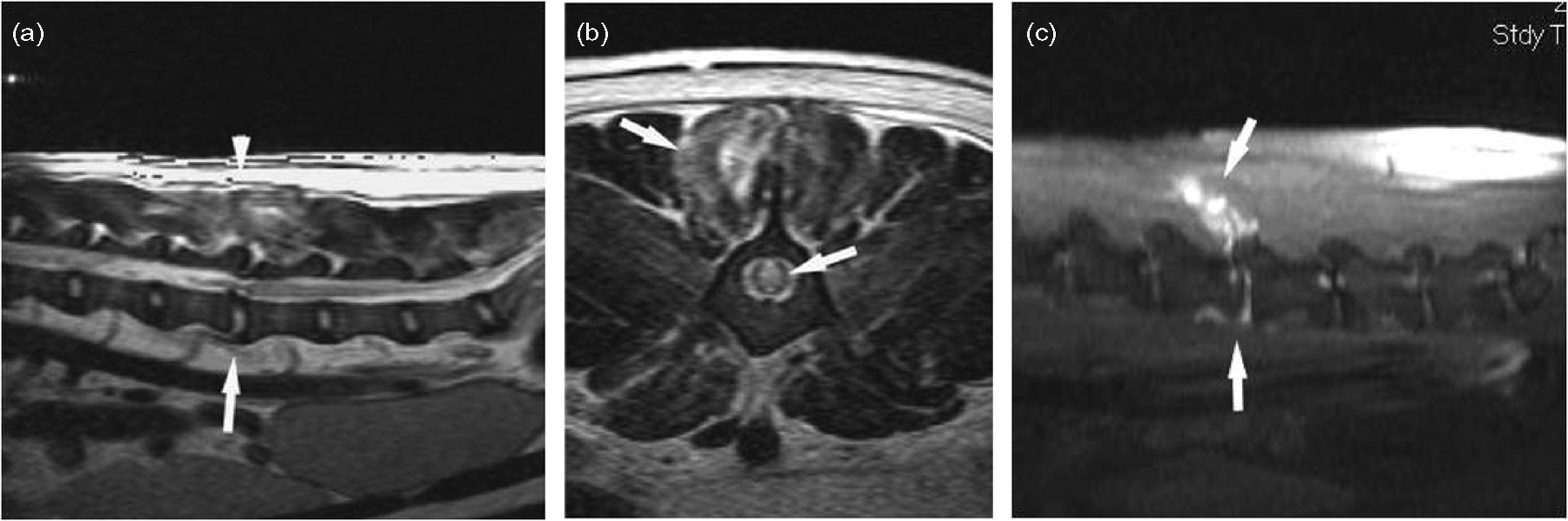


Finally, animal 1 had a small, well-defined, extramedullary pouching lesion that was dorsolateral to the spinal cord and hyperintense on T2-weighted sequences (Fig. 5). Intrathecal administration of Gd-DTPA enabled us to identify a contrast-filled meningeal pouch, consistent with a post-traumatic meningeal lesion or post-traumatic meningocele.
Case 1. Sagittal fat-saturated T1-weighted image after intrathecal administration of Gd-DTPA displays a contouring, cystic-like hyperintense lesion (arrow head) consistent with a small pseudomeningocele
Neither clinical nor biological side-effects nor toxicity, attributable to the administration of the intrathecal contrast agent, were exhibited by the study cohort.
Discussion
Dural tears secondary to spinal trauma are potentially serious injuries that, if left unrepaired, may cause the herniation of neural elements through the meningeal defect. These structures may become entrapped in scar tissue, which in turn may lead to chronic pain, neural dysfunction, or intracranial hypotension syndrome. In addition, dural tears increase the risk of meningitis and focal infections. These infections may, in turn, cause dural lacerations that remain open indefinitely, which may lead to the development of post-traumatic meningocele. If left untreated, nerve root entrapment may delay, or entirely preclude, neurological recovery (2, 3, 8, 9).
Dural tears, rents, and lacerations are very difficult to diagnose clinically or radiologically before surgical exploration. Before the advent of CT dural tears were diagnosed radiologically through myelography (which is no longer used). Plain CT has low sensitivity and low specificity for the detection of spinal meningeal injury (10). Although CT myelography using water-soluble iodinated contrast medium overcomes some of these limitations, Gd-enhanced MR cisternography/myelography appears to be superior in the evaluation of dural leaks (4–6), including spinal leaks. MR cisternography/myelography is usually conducted following a standard MR spine imaging protocol, which provides an adequate general assessment of spinal cord injuries, including meningeal tears. This modality can also aid in the detection of spinal fractures, as well as paraspinal and vertebral soft-tissue edema and injuries (11, 12). In addition, plain CT images are useful in the overall evaluation of spinal fractures because of their ability to display complex bone lesions, including facet joint injuries (13, 14). Nevertheless, despite the anatomical detail of the brain, spinal tissues, and CSF that the conventional MRI technique provides, there are still a number of conditions for which CSF contrast enhancement is beneficial, including the detailed assessment of the subarachnoid spaces, abnormal CSF collections and leakages, and the study of CSF dynamics. To determine the potential feasibility and accuracy of intrathecal Gd-DTPA administration in the diagnosis of dural tears and the detection of CSF leaks, we have designed this prospective study in small animals that had experienced accidental spinal trauma with neurological deficit. We believe that this situation provides a comparable scenario to what may occur in humans seeking medical assistance for similar injuries. Previous studies in animal models have reported the benefits of Gd-DTPA-enhanced MRI to study CSF pathway disorders, and have outlined its tolerance and dose limits (15, 16). One such study has been performed in the field of clinical veterinary practice (7). This examination provides new information regarding the potential sources of fistulae or meningeal disorders that can otherwise be difficult to diagnose.
Our series of animal subjects underwent medical care comparable to which might be offered to humans under similar circumstances. They were evaluated by a team of veterinary neurologists or neurosurgeons for specific diagnoses and treatment. The range of neurological manifestations elicited included involved sensory loss, paralysis, and paresis. Although the mechanisms of spinal injury and the corresponding clinical consequences differ between small animals and human beings, we believe that the diagnostic performance of intrathecal Gd-DTPA can be extrapolated from other mammals to humans.
Our results show that, at least in cases of moderate or severe spinal injuries, dural tears with CSF leaks are common (four out of five cases) and likely multiple. Dural tears may be located adjacent to or far from the vertebral or spinal cord lesion and their location is easily evaluated with Gd-enhanced MR cisternography/myelography. The frequency of dural tears secondary to spinal injuries in our study is similar to the values obtained in an investigation conducted by Morris et al., which was performed in humans with the use of CT metrizamide (17).
Although plain MRI can accurately display spinal cord injuries, many bony lesions, disk and ligament disruptions, potential epidural compressions, and adjacent soft tissue injuries, it can only suggest the presence of meningeal tears or lesions. Prompt surgical correction of entrapped nerve roots may markedly improve neurological deficit in these cases (18). Furthermore, the results of our study indicate that the detection of dural tears and the consequences of CSF leaks may aid in explaining the clinical presentation and associated neurological deficit observed in these animals.
With regard to the source of CSF leaks, we can identify two specific radiological patterns. First, there is a pattern in which the source of the Gd-DTPA leakage can be precisely defined. In this pattern, there are usually one or two sources, and the course of the contrast material tracks follows the trajectory of the meningeal fistulae and eventually pinpoints the meningeal tear (Cases 1 and 2). There is a second pattern in which the contrast leakage is diffuse and disseminates into areas adjacent to the location of the spinal injury, although no single source of Gd-DTPA emergence can be identified (Cases 3 and 4). It appears that the first pattern tends to occur in instances of less severe spinal trauma, and nerve root or sleeve avulsion mechanism should be suspected. This was the pattern in animal 2, in which a brachial plexus injury was finally diagnosed. By contrast, the second pattern might be more frequently associated with severe injuries, which are more prone to develop meningeal lacerations (2), as observed in Cases 3, 4, and 5.
The differences between these two patterns might be important when considering surgical treatment in humans (2, 3). Even in the single case whose CSF leak was not observed, a post-traumatic dural lesion was demonstrated. Although the consequences of the post-traumatic spinal meningocele in this particular animal are difficult to predict, we know that in humans it has the potential to promote nerve root entrapment (2, 3). Dural tears are found in 7–28% of patients operated upon for spinal injuries. We also know that dural tears in humans may be missed if the fracture is treated non-operatively or by an anterior approach alone (2, 3). Furthermore, the absence of neurological deficit in patients with spinal trauma does not exclude the presence of dural tears or nerve root entrapment, and in spinal trauma the absence of neurological deficit does not exclude either dural tearing or nerve root entrapment (18).
Technically, acquisition sequences should always include T1-weighted fat-saturated images. These sequences are highly suitable for the evaluation of CSF leaks because they suppress the high signal intensity produced by the fat-containing medullary bone, thereby avoiding the possible misinterpretation and pitfalls of distinguishing the high-signal-intensity CSF (which contains gadolinium) from bone (which contains fat), which might conceivably be confused with leaks. We believe that fat-saturation techniques facilitate the recognition of fistulae and tracks not only because they suppress the signal from the medullary bone, but also because they suppress fat signal from epidural, paraspinal, and subcutaneous fat-containing tissues, as shown in Figures 1C, 2B-C, 3C, and 4. These findings are particularly useful when CSF leaks are suspected in patients during the post-traumatic period, yet they are also of use in the evaluation of any type of leak and any study of the spine (4, 5).
From a pathophysiological and clinical perspective, it is of interest to note that some collection, apparently unrelated to the injury itself and not explained by the standard MRI examination, which included the intravenous administration of Gd, was ultimately explained by the demonstration of a CSF leak once the intrathecal administration of Gd-DTPA was performed (Case 2). Additional T1-weighted sequences with i.v. administration of Gd are advisable to perform in cases that feature fluid collections around the traumatized areas in order to distinguish edematous post-traumatic tissues or inflammatory collections.
With respect to the safety and tolerability of gadolinium-enhanced MR cisternography, many clinical trials and clinical series have established its tolerability and low incidence of minor side-effects in both animals and humans (4, 5, 15–21). An additional benefit of MRI is the absence of radiation exposure. Also, in our study, no clinical or biological adverse effects were recorded that were attributable to the intrathecal administration of the contrast agent.
We believe that these results are important for various reasons. First, Gd-enhanced MR cisternography/myelography is a minimally invasive but a very sensitive and effective examination for imaging CSF leaks in the setting of spinal trauma, which is a particularly challenge for any diagnostic test. Second, regarding our own experience and extrapolating from the human experience, this complication is likely more frequent than previously thought, given that its reported prevalence has ranged from 7.7% to 25% in previously published neurosurgical series, (2, 3, 10). This complication is particularly common among patients who have sustained high-energy trauma, especially patients with laminar fractures, lumbar burst fractures or patients with neurological deficit. This information is critical in determining the best surgical treatment for these patients, because the management of dural tears requires an initial posterior approach, dislodgement of entrapped nerve roots and the repair of dural tears (3). Third, CSF fistulae were visualized as enhancing material originating from or adjacent to the spinal canal. These leaks presented varying routes along the paravertebral and surrounding tissues, ranging from a single source to countless sources, which likely represent a large dural laceration. Next, all of the animals in this study that presented with moderate or severe spinal injuries with neurological deficit were eventually diagnosed with major meningeal tears or rents only after gadolinium-enhanced MR cisternography/myelography was performed. Finally, intrathecal Gd-DTPA has the potential to determine an independent prognostic factor in moderate to severe spinal trauma. In summary, Gd-enhanced MR cisternography has proven to be an effective and minimally invasive method for evaluating suspected CSF fistulae in patients suffering from spinal injuries.
However, our report presents some shortcomings. First, this study was performed in small animals, and although many clinical and pathophysiological features in the field of spinal injury can be extrapolated to human beings, a number of unrecognized differences could have been overlooked. Nevertheless, the purpose of the research was to create a reproducible model that demonstrated the feasibility and effectiveness of gadolinium-enhanced MR cisternography to detect CSF fistulae in cases of spinal injury before its application in clinical practice. The study's second shortcoming is the lack of surgical confirmation of dural lesions. However, evidence collected from previous studies regarding the demonstration of CSF leaks using intrathecal Gd-DTPA injection renders these observations reliable (4, 5). Furthermore, the study presents a very limited number of cases. However, the tested subjects were non-selected and provided an adequate cross-sectional survey of typical spinal injuries in small animals whose owners seek veterinary care. Additionally, gadolinium-enhanced MR cisternography shares the contraindications and risks of any CNS puncture, as well as those associated with MRI technology, such as foreign bodies and pacemakers. Finally, the intrathecal administration of gadolinium-containing compounds is not currently approved worldwide, and is off-label in the United States and in many European countries, although it appears to be clinically more useful and less risky than CT cisternography/myelography (4–6).
In conclusion, we have described the use of intrathecal Gd-DTPA in the diagnosis of meningeal lesions, in particularly dural tears, in small animals that have experienced spinal trauma. It superbly depicts the leaks and tracks of the CSF escaping from the spinal canal into other compartments, as well as meningeal tears and lesions. The effectiveness of this examination appears to be very high, and the results can be reliably extrapolated to human medicine, although the intrathecal Gd-DTPA administration in humans is not currently approved worldwide. The diagnosis of such complications is important because of the prognostic and therapeutic implications they entail for animals and humans alike. This study should encourage the use of this diagnostic modality in humans in the setting of moderate to severe spinal trauma.
Footnotes
ACKNOWLEDGEMENTS
This work was supported in part by the Ministry of Science and Innovation (Ministerio de Ciencia e Innovación) of Spain (Ref.: TIN2007–61768).