
Abstract
Background
Primary surgical repair forms the definitive treatment of esophageal atresia. Long-term survival rates and patient morbidity after repair still remains a problem especially in developing countries. Postoperative morbidity depends on the incidence of anastomotic leak, gastroesophageal reflux, strictures, and recurrent fistula formation.
Purpose
To describe the frequency of different findings at fluoroscopic evaluation of postoperative esophagus in children following repair for esophageal atresia with or without tracheo-esophageal fistula.
Material and Methods
Hospital records and upper gastrointestinal contrast studies of 210 patients following repair for esophageal atresia with or without a tracheo-esophageal fistula were reviewed by two pediatric radiologists. All children underwent surgery in the first few days of life (days 1–6). Fluoroscopic contrast study was performed at various intervals after surgery in children with suspected complications or feeding difficulties.
Results
Images from upper gastrointestinal contrast studies of 210 patients (126 boys, 84 girls) were evaluated and recorded. Findings were recorded as normal postoperative appearances (37.1%) and complications/sequelae, which included strictures (33.8%), minor and major leaks (11.9%), reflux (13.8%), motility problems (7.1%), persistent fistula (3.8%), diverticulae formation (4.7%), and hiatus hernia (2.1%).
Conclusion
Strictures, leaks, and reflux are the most common complications of esophageal atresia repair. Knowledge of various postoperative appearances would be useful for planning an appropriate management strategy in these children.
Keywords
Esophageal atresia (EA), first described by Gibson in 1697 (1), is the most common congenital malformation of the gastrointestinal tract, second only to anorectal malformations (2). According to a population-based study, using data from a large European database for two decades, the reported overall prevalence is 2.4 cases per 10,000 births (3). EA comprises of a spectrum of anomalies, with EA and distal tracheo-esophageal fistula (TEF) being the most common defect, seen in nearly 85% of these children. A child with EA-TEF typically presents with feeding difficulties, choking, respiratory distress, and frothing in the first few hours of life. Associated anomalies are frequently seen in children with EA, occurring in more than 50% of patients, described as VACTERL (vertebral, anorectal, cardiac, trachea-esophageal, renal, and limb) defects (4).
Surgical treatment involves primary or delayed anastomotic repair which requires significant surgical skill. Although the mortality after primary repair is almost negligible, long-term survival rates still continue to be poor in patients with associated cardiac, central nervous system, or pulmonary anomalies (5). Moreover patient morbidity after repair still remains a problem especially in developing countries. Postoperative morbidity depends on the incidence of anastomotic leak, gastroesophageal reflux, strictures, and recurrent fistula formation. Knowledge of the imaging appearances of these conditions is essential especially on fluoroscopic contrast studies (contrast tube esophagograms) for prompt identification and management. The present study describes the postoperative appearances of esophageal atresia repair and evaluating the incidence of various appearances in the given surgical population.
Material and Methods
The present study is a retrospective study wherein contrast tube esophagograms of all patients admitted in the pediatric surgery unit who underwent repair of esophageal atresia/ tracheo-esophageal fistula over a 5-year period (April 2006 to March 2011) were reviewed after approval from the institute ethics committee. Two hundred and ten children who had undergone upper GI contrast studies after surgical repair as part of follow-up formed the study group.
Apart from the demographical data including age, gender, other relevant systemic examination, and radiological findings were also recorded.
The standard surgical approach was aimed at primary repair in all cases except in cases of long gaps, poor general condition, or major associated anomalies. Surgery was performed in all children through thoracotomy approach using extra pleural technique when possible. In all cases of distal tracheo-esophageal fistula, ligation and disconnection of fistula and end-to-end esophageal anastomosis was performed. In children with long gap esophageal atresia, however, lower pouch mobilization surgery was performed.
In patients clinically suspected to have a leak in the immediate postoperative period, close monitoring of the retropleural drain was done along with a contrast study. Minor leaks were identified by appearance of frothy saliva in the retropleural drain with no accompanying deterioration in the general condition and a small radiological leak while major leaks were clinically suspected by the drain contents with the accompanying clinical deterioration of the patient either due to mediastinitis, pneumonitis, and septicemia and associated with a large defect in anastomosis on upper GI study. In patients who had no retropleural drain, leaks were clinically suspected by increased respiratory distress, fever, and sepsis, or the presence of pneumothorax/consolidation in the thorax. Apart from immediate postoperative UGI studies, follow-up contrast studies were also performed at various intervals after surgery on outpatient basis in children with feeding difficulties or other related complaints to look for stricture, gastroesophageal reflux, any motility disorder, or recurrent fistula.
A postoperative water-soluble contrast tube esophagogram with non-ionic contrast medium was performed at various intervals post surgery; in the immediate postoperative period for predominantly ruling out anastomotic leaks and in the latter periods for diagnostic purposes for identifying strictures, GE reflux, motility problems, and recurrence, depending on patient symptomatology. Adequate examination could be performed in all patients with the endpoint being complete visualization of the esophagus/ proximal stomach, anastomotic leak, aspiration into the tra-cheobronchial tree, and demonstration of a recurrent fistula if any. Contrast study involves injection of non-ionic contrast media through a small feeding tube placed through the nose and its tip placed initially in the distal esophagus or gastric fundus by an experienced radiologist under fluoroscopic control. Non-ionic contrast media is injected through the tube and the tube is slowly withdrawn till upper thoracic level (above level of tracheal bifurcation) while the contrast is being slowly injected in small amounts. Both lateral and supine views are necessary for an adequate study. Prone views at our institution are also performed as an add-on views in select problem cases (intu-bated children and in cases where it is not sure whether contrast in airways is due to aspiration or fistula).
Only stored fluoroscopic images (last image hold) were used, which is in line with our departmental protocol to reduce radiation dose in all the children. Although these stored fluoroscopic images are grainy, they are of diagnostic quality, as was demonstrated in this study.
All the contrast studies (contrast tube esophagogram) were interpreted and reported by two pediatric radiologists (KSS, AKS) both having 8–10 years of experience in pediatric radiology. One of the two pediatric radiologists performed the study and stored its images. Both pediatric radiologists, however, interpreted and reported the stored images. Anastomotic leaks were defined after Auldist et al. (6) as minor leakage (saliva in chest drain, but clinically well) and major leakage (mediastinitis or abscess, pneumothorax, empyema, radiologically confirmed major esophageal disruption). Esophageal stricture was suspected if the patients had symptoms of dysphagia, feeding difficulties, or other signs of obstruction. On contrast tube esophagograms, a stricture was defined as obstructive or non-obstructive (good distal flow). Gastresophageal reflux (GE reflux) was evaluated and categorized as minor (restricted till lower third/until carina) and major (reflux till the upper thoracic esophagus/beyond carina). Other conditions like recurrent fistula, esophageal motility problems, and diverticulae and esophageal hernias were also noted. Subsequent comparisons with other published studies were performed.
Results
Two hundred and ten patients of EA with/without (TEF) who underwent surgery and follow-up contrast tube esophagograms at various intervals postoperatively were included. The mean birth weight was 2.8 kg and the median age was 2.5 years (range, 6 days to 7 years) at the time of esophagography. All these children had undergone surgical repair of the OA/TEF at our institute within the first week of life and were on regular follow-up (average follow up period, 3 years; range, 3 months to 7 years) since then.
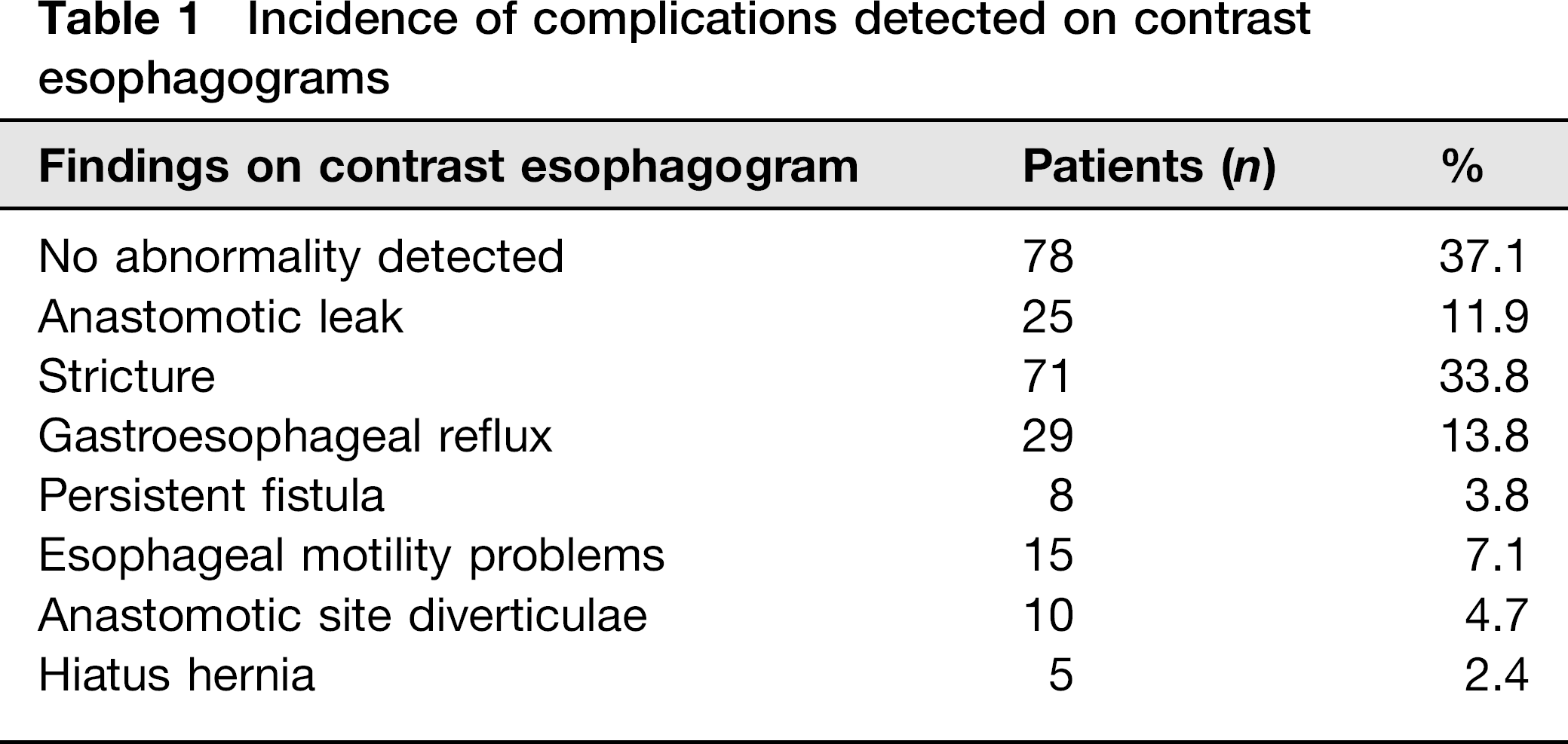
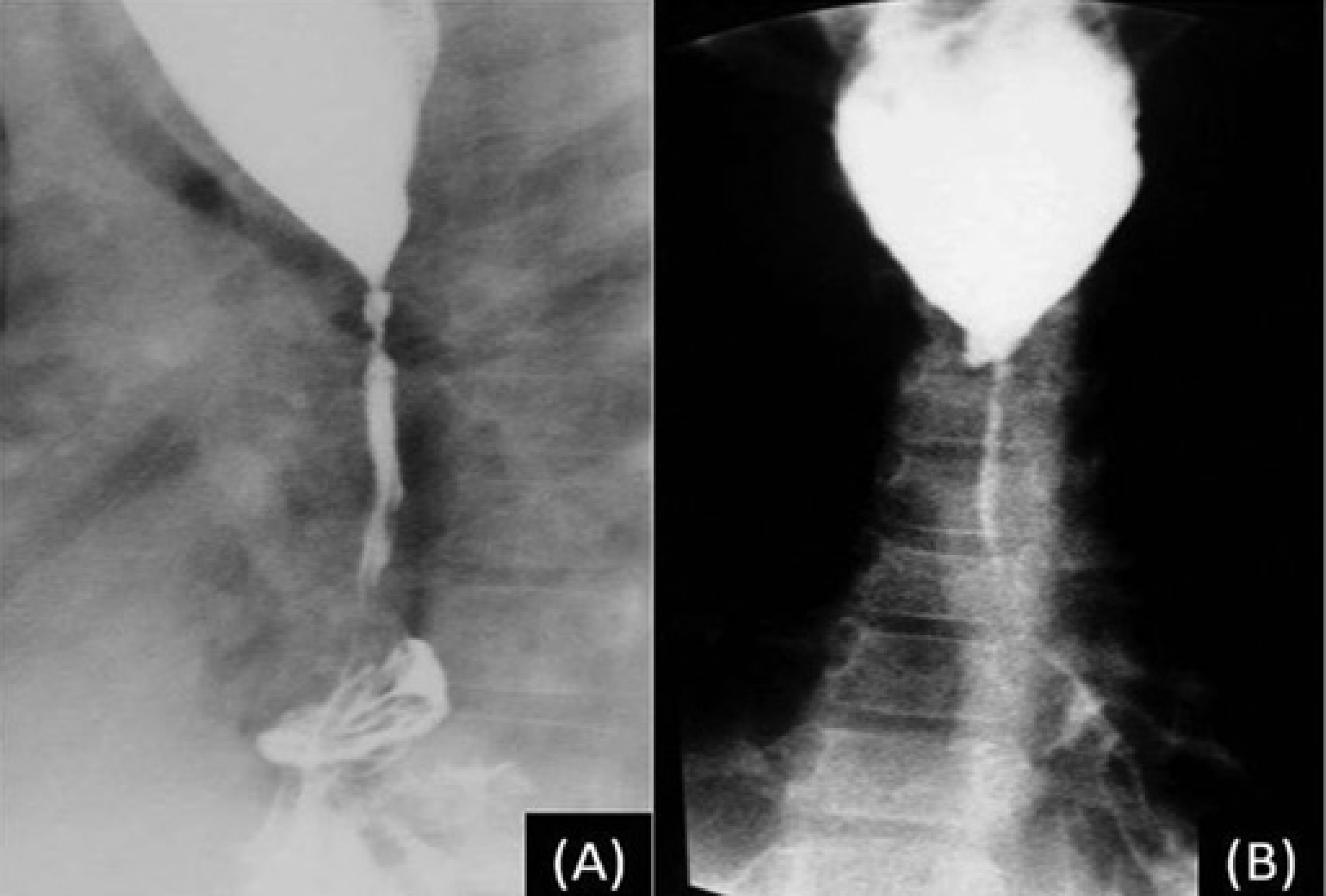
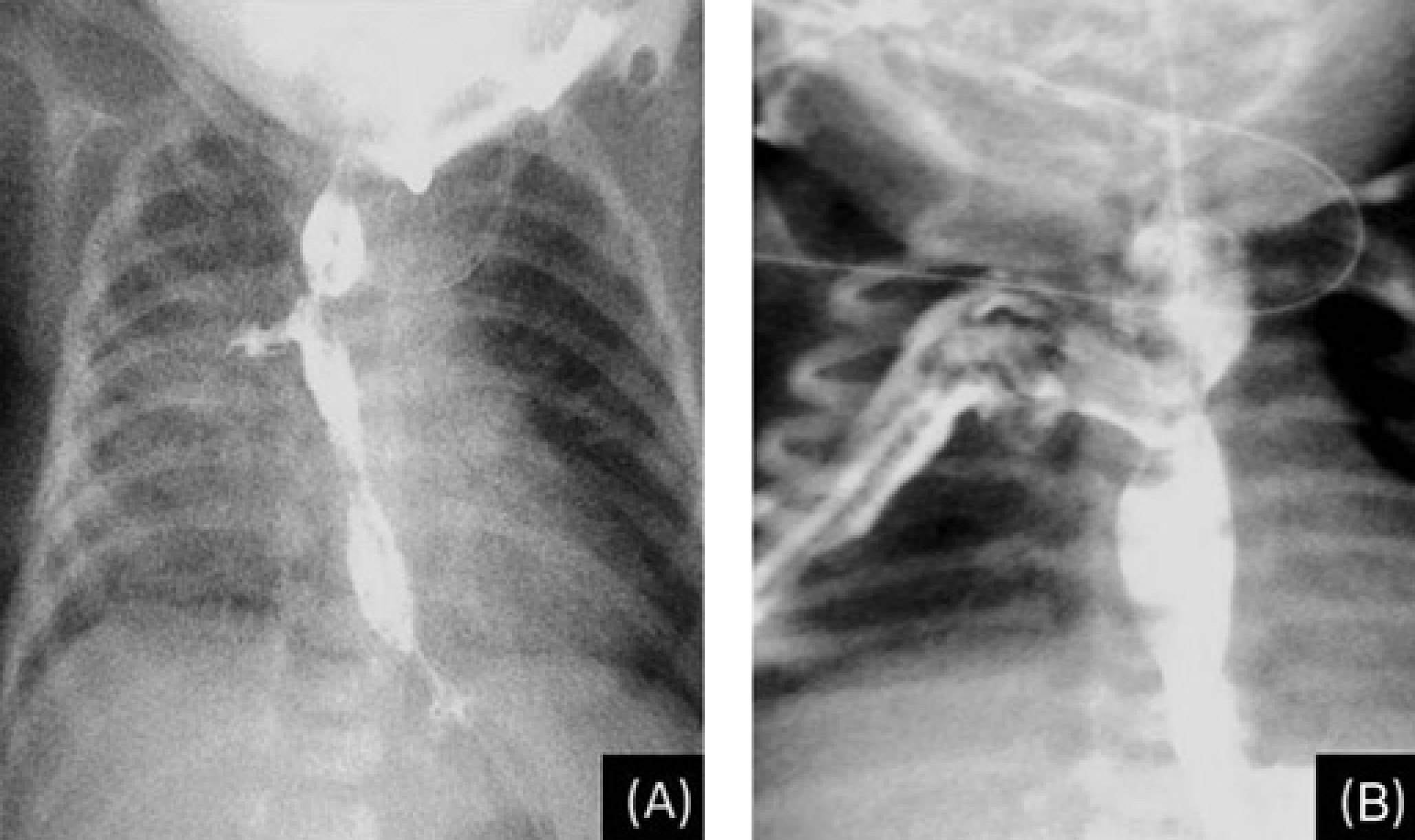
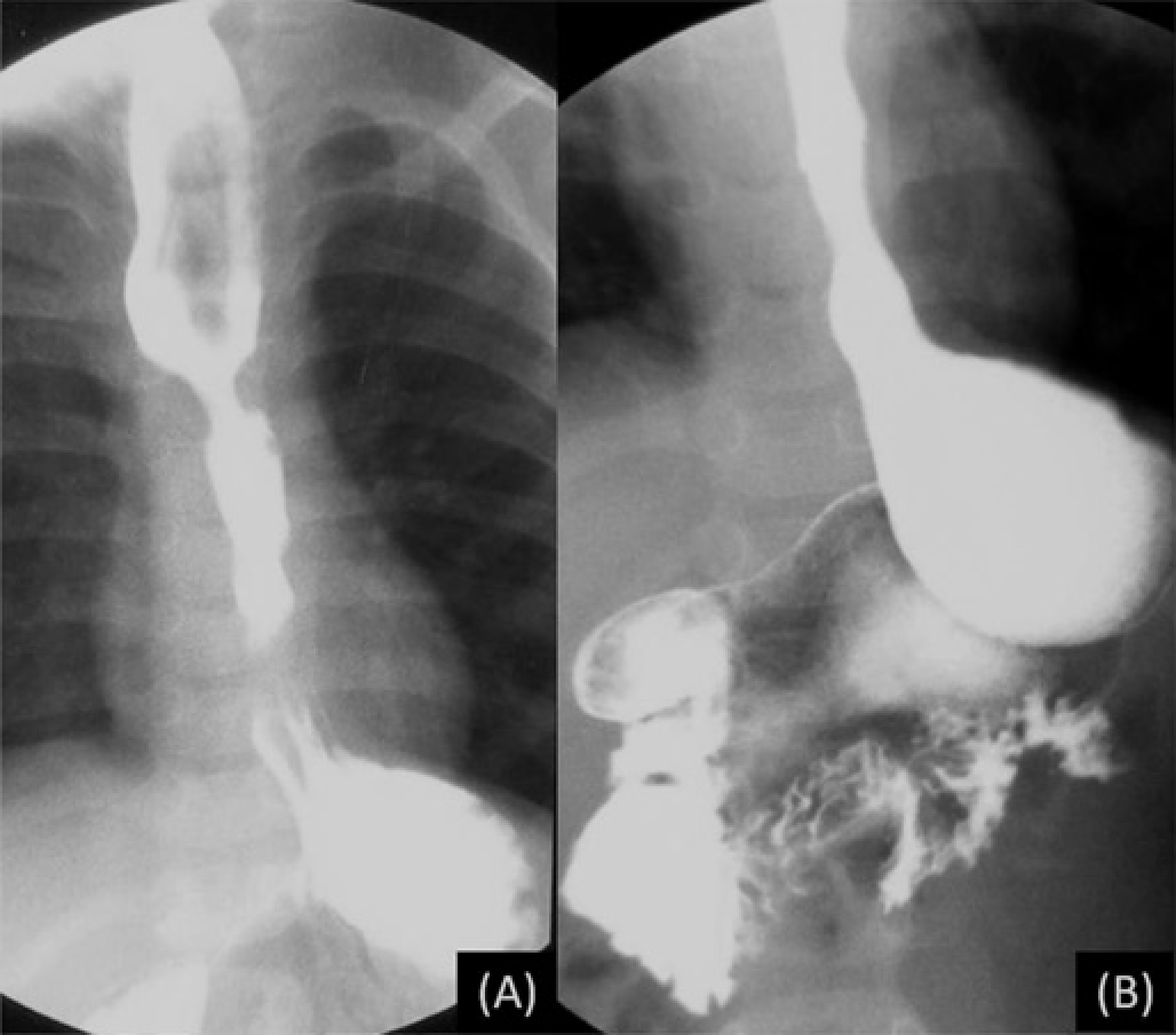
Tables 1 and 2 list the spectrum of findings seen on postoperative contrast tube esophagograms. Seventy-one out of the 132 patients (33.8%) had an esophageal stricture (Figs. 1 and 2), while anastomotic contrast leaks were seen in 25 children (11.9%) (Fig. 3), GE reflux in 29 (13.8%) (Fig. 4), and persistent/recurrent fistula in eight (3.8%) (Fig. 5).
Incidence of complications detected on contrast esophagograms
Subclassification of the anastomotic leaks, strictures, and gastroesophageal reflux into major/minor and obstructive/non-obstructive patterns


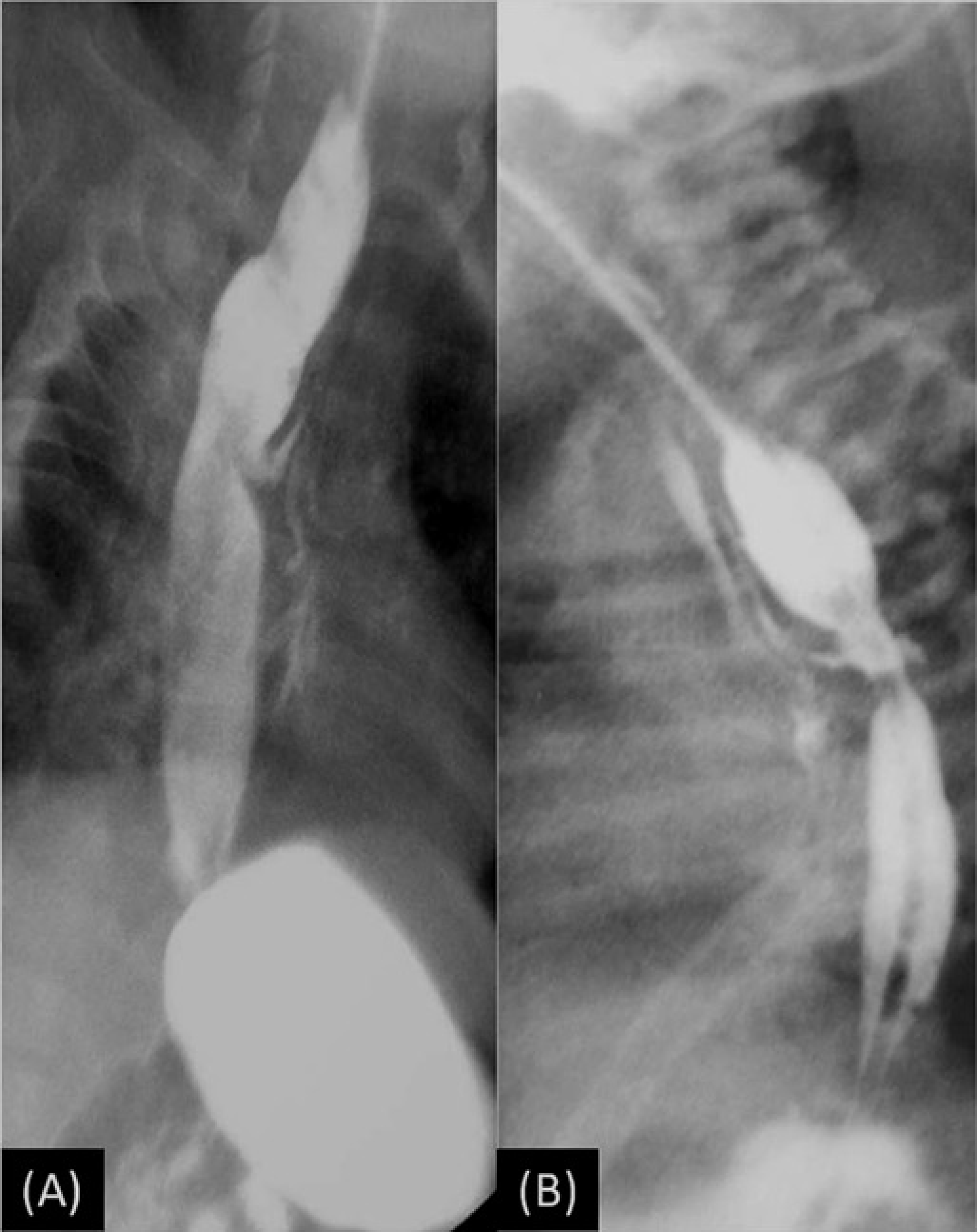
Postoperative contrast tube esophagograms depicting a partially obstructive (a) and a completely obstructive (b) stricture
Contrast tube esophagogram demonstrating long segment esopha-geal stricture with hiatus hernia
Postoperative contrast tube esophagograms showing minor (a) and major (b) anastomotic leaks
Contrast tube esophagogram showing a major gastroesophageal reflux
Postoperative contrast esophagogram revealing remnant/ recurrent upper pouch tracheo esophageal fistula
Discussion
Strictures, leaks, and reflux are the most common complications of esophageal atresia repair in children who undergo surgery for esophageal atresia with or without trachea-esophageal fistula. A recent population-based study using data from 23 well-defined European regions has reported overall prevalence of 2.4 cases per 10,000 births (3).
More than 50% of infants with esophageal atresia have an associated anomaly (7) related to cardiovascular (29%), genitourinary (14%), gastrointestinal (13%), anorectal (14%), skeletal (10%), and respiratory (6%) systems. Genetic abnormalities are seen in 4% while in another 11% other abnormalities not related to any specific system are present. This condition was associated with a high rate of mortality until lately. Recent developments in anesthesia, surgical techniques, cardiology and cardiac surgery, nutrition, and antibiotic therapy, however, have contributed to improvements in survival and function of affected infants.
Primary surgical repair with or without gastrostomy forms the definitive treatment of esophageal atresia. Complications related to the surgical procedure include anastomotic leak, stricture, GE reflux, fistula recurrence, and motility abnormalities which require scrupulous diagnostic evaluation. Of these, leaks present in the immediate/ short-term postoperative period while the others including stricture, fistula recurrence, GE reflux, and feeding/respiratory difficulties complications are medium- to long-term complications. Anastomotic leaks occur in up to 15–20% of patients with a major leak occurring in only one-third or less of these (8). The major leaks are seen in the early postoperative period (< 48 h) and present with life-threatening pleural collection/tension pneumothorax. Minor leaks are usually detected later on “routine” contrast studies performed on days 5–7 postoperatively. Anastomotic strictures develop in 30–40% of cases most of which respond to fluoroscopic dilatations (9). High anastomotic tension, anastomotic leakage, and gastroesophageal reflux lead to increased risk of stricture formation. GE reflux is common in postoperative patients with significant reflux occurring in up to 40% of cases (10, 11). Recurrent trachea-esophageal fistula is seen in 5–14% of patients (12). A suspicion of recurrent fistula should arise if the infant manifests respiratory symptoms (coughing during feeds, apnesophageal atresic, or cyanotic episodes) or has recurrent respiratory infections after “successful” repair of the esophageal atresia. Dysmotility affects the distal esophagus which can be seen on contrast studies in the form of in discoordinate peristalsis (13).
The reason for variable incidence of these complications in different studies can be attributed to different surgical methods; temporal advancements in operative techniques and largely due to slightly different way of defining these conditions, e.g. reported incidence of anastomotic leaks is between 8–21% (14–20). This is because some authors have referred only to symptomatic major leaks (18) while others have referred to radiologically apparent but clinically inapparent leaks (14). Anastomotic leaks in the present series amounted to 12% of the patients. Similarly, strictures were defined variably into combined obstructive and non-obstructive types by some authors while others have considered and reported only obstructive symptomatic strictures. The incidence of other complications like gastro-esophageal reflux, recurrent fistula, and motility abnormalities have been listed in Table 3. Comparison of the present data with other similar studies reveals near similar pattern of various abnormalities in the postoperative period. Although CT is useful in suspected esophageal perforation or leaks (21, 22) (findings include extraluminal air, periesophageal fluid, esophageal thickening, a tract at the site of the tear, and extra luminal contrast), however, it involves much higher radiation doses and is not routinely indicated especially in children.
Comparative evaluation of complications in various studies following surgical repair

Our study does have its inherent limitations. It is a retrospective study. We have only depicted the various radiological appearances as seen on a fluoroscopic contrast tube esophagograms in children who underwent surgery for eso-phageal atresia with or without tracheo-esophageal fistula. We have not dwelt in detail regarding the type of surgery performed or various surgical options available in this group of children. We have also not looked into associated anomalies. Our endeavor has been primarily to study the radiological data and to be able to identify the various complications.
In conclusion, leaks, reflux, and strictures are the most common complications seen in children following surgical repair for OA. Knowledge of the fluoroscopic contrast tube esophagograms is useful for planning an appropriate management strategy to help reduce significant morbidity in these individuals. Further, contrast tube esophagograms should preferably be performed by using non-ionic contrast medium so that leakage into the mediastinum, pleural cavity as well as aspiration into the trachea-bronchial tree do not carry increased risk of fluid retention, adhesions, et cetera, as can be seen with ionic contrast and barium suspension.