
Abstract
Background
A schwannoma arising from the pleura is rare. The computer tomography (CT) features, however, have seldom been disclosed in the English literature.
Purpose
To retrospectively assess the role of CT in the diagnosis of pleural schwannomas.
Material and Methods
Eleven patients with pathologically confirmed pleural schwannomas were included in the study. CT images and clinical data were analyzed. The CT features emphasized included the location of the neoplasm, as well as its diameter, origin, margin, shape, attenuation, enhancement pattern, and extent and invasion into adjacent structures, all of which were observed and recorded.
Results
Seven patients were men, while four were women; patients were aged 21-60 years, with a mean age of 45 years. Most cases were incidentally detected. Seven cases involved neoplasms located in the right hemithorax whereas four cases involved neoplasms in the left hemithorax. The mean tumor diameter was 4.4 cm (range, 2.3-6.4 cm). All of the tumors were solitary and well-defined ovoid (n = 7) or round (n = 4) in shape. The schwannomas showed isoattenuation (four cases) or mild hypoattenuation (seven cases) to the chest wall muscle on unenhanced CT. All cases showed minimal enhancement on contrast-medium-enhanced CT. Two bony erosions of the rib were also observed.
Conclusion
CT findings may suggest the diagnosis of pleural schwannoma preoperatively. Pleural schwannoma should be included in the differential diagnosis of solid, solitary, and well-defined pleural tumors.
Schwannoma (or neurilemmoma) is usually a benign, slow-growing neoplasm that originates from any nerve that has a Schwann cell sheath. Schwannomas tend to develop in the head and neck. Schwannomas in the flexor surfaces of the extremities are usually small and solid, while schwannomas arising in the mediastinum and retroperitoneum are considerably larger and are more likely to undergo spontaneous degeneration and hemorrhage (1,2). Schwannoma is an exceptionally rare neoplasm in the pleura (3). Most of the published materials on schwannomas in the pleura are either case reports or relatively small series, recorded primarily in the surgical literature, with limited emphasis on imaging characteristics (3–7). Thus, the clinical and radiological features of pleural schwannoma have yet to be established, and its preoperative diagnosis is sometimes challenging.
The aim of the present paper was to present the imaging features and clinical characteristics of 11 cases with pleural schwannomas examined by multi-detector computed tomography (MDCT).
Material and Methods
Patient selection
The institution review board approved the present retrospective study, and the requirement for informed consent was waived. Between January 2003 to December 2011, 11 patients underwent surgery for pathologically confirmed pleural schwannoma. Seven patients were men and four were women. Available clinical data and CT manifestations, as well as the surgical and pathological reports, were reviewed for each patient.
After the operations, patients were assessed clinically and with MDCT on follow-up. The follow-up period ranged from 8 to 76 months (mean, 49 months).
CT techniques
All patients underwent chest MDCT. Seven patients underwent a 16-slice CT scan, whereas four underwent a 64-slice CT scan (LightSpeed; GE Healthcare, Milwaukee, WI, USA). All patients were given a non-ionic iodinated contrast material (Omnipaque 300 mg I/mL, GE Healthcare) administered using a power injector (Ulrich Medical, Germany) at a rate of 2.5–3.0 mL/s through an 18-gauge intravenous catheter placed in an antecubital vein. The dose of the contrast material delivered was 2 mL/kg of the patient's body weight. A 20 mL flush of normal saline solution was administered immediately after the contrast material was injected. All axial CT images were obtained during breath-holding before (unenhanced) and 50–60 s after the initial administration of contrast material.
The major scanning parameters were as follows: tube potential, 120 kV; tube current, 260 mA; beam pitch, 1.5; beam collimation, 4 to 2.5 mm; gantry rotation time, 0.8 s; section thickness, 4.0 mm; reconstruction interval, 4.0 mm; and table feed, 15.0 mm/rotation. Images were reconstructed in the lung windows and mediastinal windows on the workstation for review.
Imaging analysis
All CT images were evaluated retrospectively at the interactive picture archiving and communicating system workstations by two senior radiologists (SDH and QS) with 15 and 25 years of experience in radiological diagnosis, respectively, in a consensus manner. Cases of doubt in readings were resolved through consultation with an experienced radiologist (KMC). The items included in the imaging analysis were the following: (i) location (left or right hemithorax); (ii) lesion size; (iii) margin (well-defined or ill-defined); (iv) shape (round or oval); (v) comparison of attenuation characteristics of the tumors with those of surrounding chest wall muscles and described as follows: hypo-, iso-, or hyperattenuation on unenhanced and enhanced CT images; and (vi) enhancement pattern (homogeneous or heterogeneous). The presence of details of invasion into adjacent structures was recorded. If the radiological and pathological evaluations differed, the pathological evaluation was considered final.
Results
Clinical features
Clinical data and CT features are summarized in Table 1. The mean age of the patients was 45 years (range, 21–60 years). Most of the patients (8/11) were asymptomatic, and the lesions were detected incidentally during a routine physical examination; the three other patients complained of chest pain or discomfort. Physical and laboratory test results of the patients, including serum catecholamine's, were within the normal range. None of the patients had a history of neurofibromatosis.
Summary of clinical data and CT features of pleural schwannomas
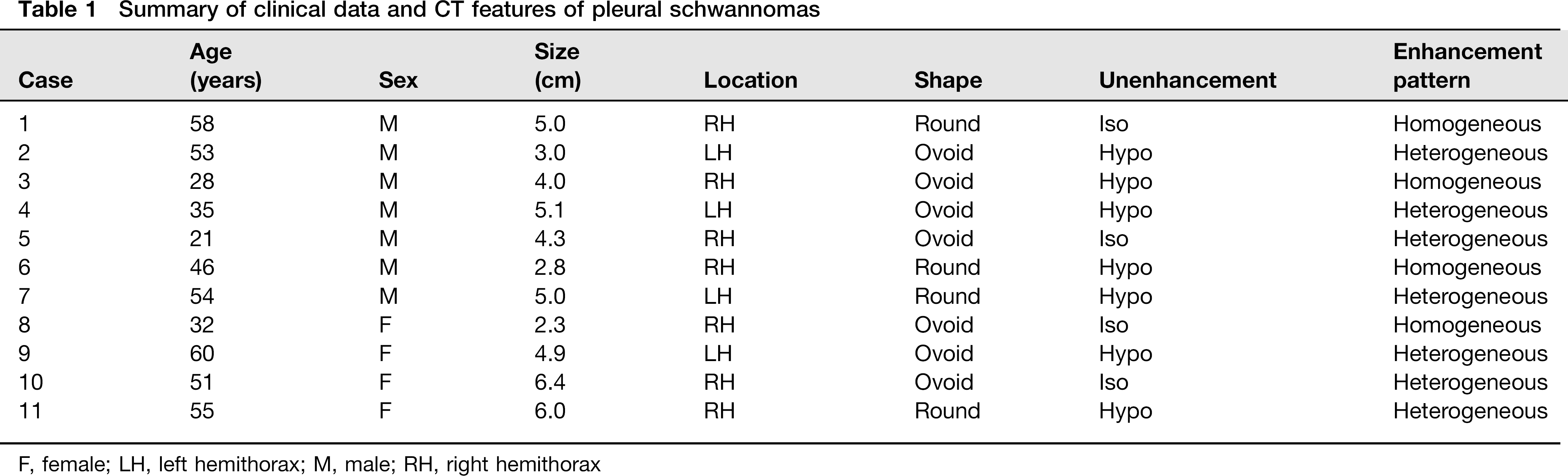
F, female; LH, left hemithorax; M, male; RH, right hemithorax
The operative procedure was tumor extirpation in all cases; five patients underwent wedge resection by video-assisted thoracoscopic surgery. In all cases, the tumor was completely excised, with clear resection margins. No complications arising from surgery and no evidence of recurrence at a mean follow-up of 49 months were observed.
CT imaging characteristics
All tumors had a well-defined margin, were solitary, and were either round or oval in shape (Figs. 1–3). The imaging features are summarized in Table 1. Pleural tumors were ovoid (n = 7) or round (n = 4) in shape. Seven tumors were located in the right hemithorax and four were found in the left hemithorax. The average diameter of the tumors was 4.4 cm (range, 2.3–6.4 cm). Schwannomas on unenhanced CT showed either isoattenuation (four cases) or mild hypoattenuation (seven cases) to the chest wall muscles. The tumors appeared homogenous considering attenuation in four patients (Fig. 2) and heterogeneous in seven patients on contrast-enhanced CT. All tumors showed minimal enhancement on contrast-enhanced CT (Fig. 1). Two tumors showed erosion of the underlying rib (Fig. 1a). The lesion-lung interface was smooth (Fig. 3c).
A 21-year-old man with schwannoma who complained of chest pain shows a tumor located in the right posterior hemithorax. (a) Unenhanced chest CT shows a 2 cm × 3 cm ovoid tumor, with underlying rib erosions. (b) Contrast-enhanced axial CT image demonstrating heterogeneous enhancement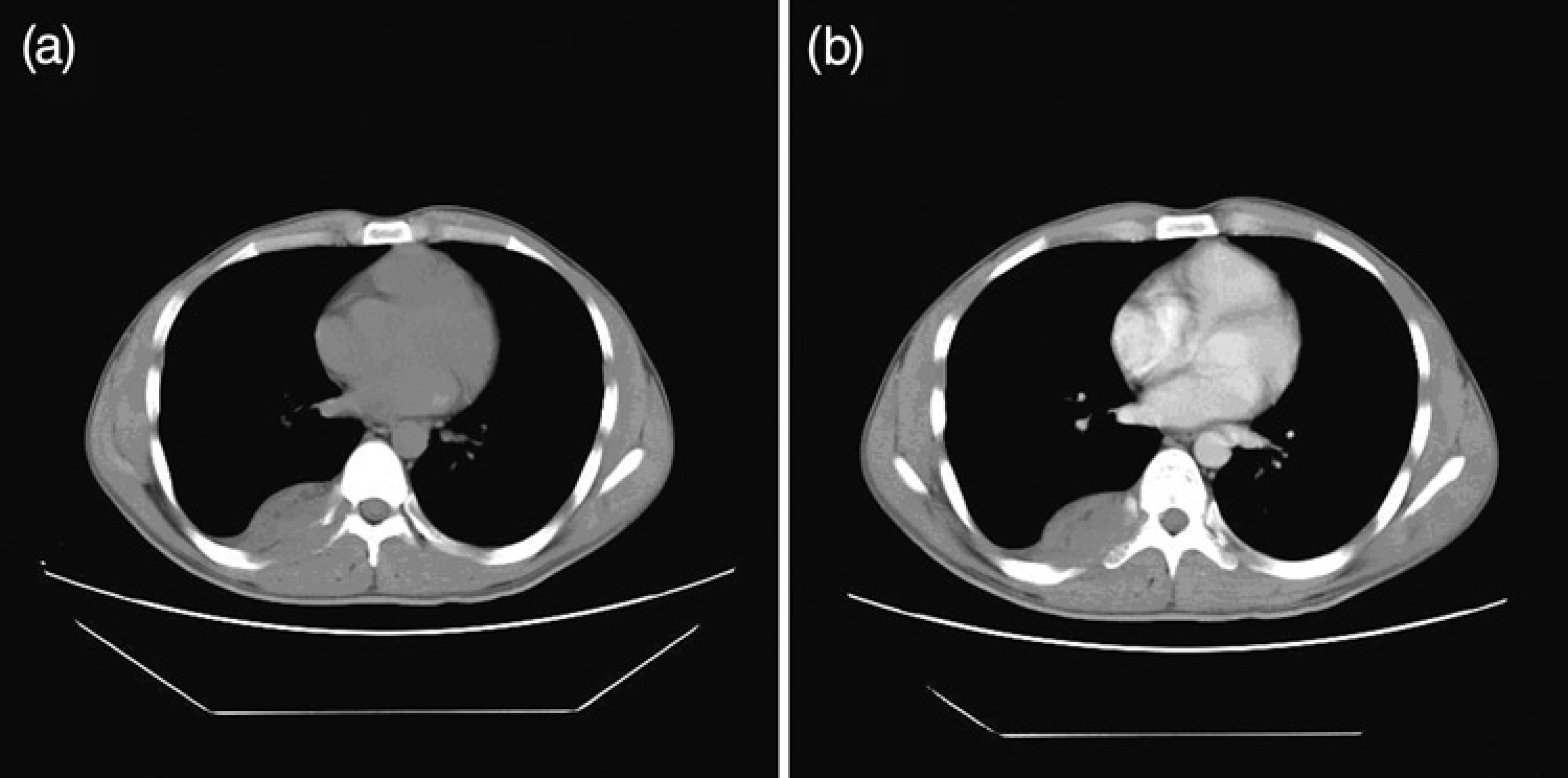
A 58-year-old man incidentally discovered with a tumor through a routine chest radiographic examination. (a) Unenhanced CT shows a 5 × 3 cm, round, well-defined margin tumor (b) Axial contrast-enhanced CT shows a well-defined homogeneous pleura-based mass, demonstrating a slightly homogeneous enhancement pattern with 17 HU of net enhancement
A 32-year-old woman with schwannoma in the right lower hemithorax. (a) Unenhanced CT shows a round hypoattenuation to the pleura muscle (b) Axial contrast-enhanced CT shows a pleura-based mass with obtuse tumor-pleura angles and minimal homogeneous enhancement. (c) An axial CT image displayed in the lung window setting shows that the lesion-lung interface is smooth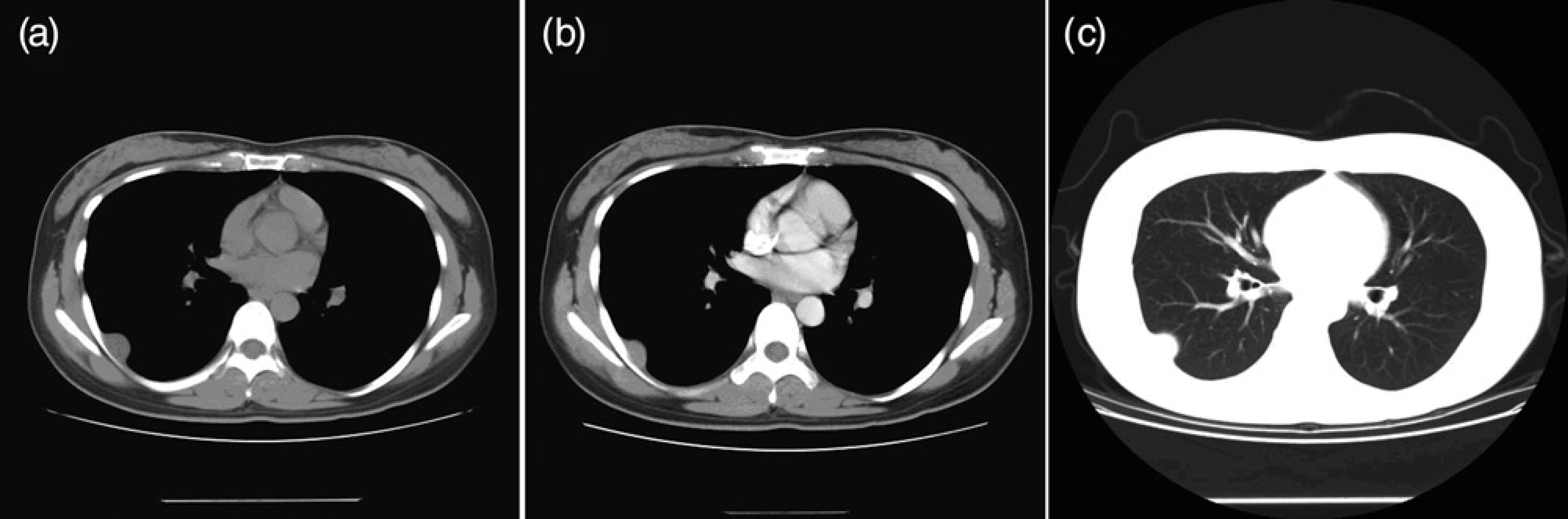
Associated features, including calcification, ipsilateral pleural effusion, vessel invasion, and encasement, were absent in all cases. No lymph nodes and distant lesions were detected on MDCT images.
Discussion
This article presents the largest radiological series of benign pleural schwannomas to date. Primary pleura tumors are rare and constitute 1–2% of all thoracic tumors (8). Although rare, it is important for a radiologist to recognize the appearance of schwannomas because they can be mistaken for malignant tumors.
Primary pleural tumors have an almost equal chance of being benign or malignant (8–10). However, the risk of malignancy in a nerve sheath tumor is minimal (2–5%) unless a history of Von Recklinghausen's disease or radiation exposure, which increases the risk (3,11). As primary pleural tumors, the mean size of malignant tumor is larger than that of benign tumors (10). The majority of pleural schwannomas are asymptomatic. An incidental mass seen on a chest radiograph is a common presentation of pleural tumors. The lack of symptoms has been attributed to a very slow tumor growth. Pain and neurological symptoms are uncommon unless the tumor becomes large. One patient in our study reported anterior left rib discomfort lasting for 10 years, which was believed to be musculoskeletal in nature. Schwannomas occur at all ages but most typically in persons between the ages of 20 and 50 years and more frequently in men than in women (12).
Histologically, a typical schwannoma is S-100 protein positive (neurogenic) and has two components: Antoni type A (cellular component) and Antoni type B (myxoid component). The heterogeneous characteristics of a schwannoma are caused by confluent areas of hypocellularity adjacent to densely cellular or collagenous regions, xanthomatous changes, and/or regions of cystic degeneration (13).
CT findings may suggest the diagnosis of a pleural schwannoma preoperatively. In our study, the CT appearance of all pleural schwannomas featured well-defined margins, ovoid or round shapes, with attenuations between water and soft tissue on unenhanced imaging and heterogeneous on contrast-enhanced imaging because of cellularity differences, collagenous regions, xanthomatous changes, and cystic degeneration. Heterogeneous contrast enhancement is due to variations in the degree of cellularity and loose cellularity with prominent diffuse edematous change, which may result in minimal contrast enhancement. Thus, in our study, no CT evidence of degenerative changes necrosis and calcification was observed. However, tumors in the retroperitoneum and mediastinum may be considerably larger. As a result, these tumors are more likely to manifest with secondary degenerative changes, such as cystic formation and calcification (14,15), and can occasionally cause changes in the rib, but otherwise do not invade or obstruct adjacent structures.
The preoperative diagnosis of pleural schwannomas is sometimes challenging. Pleural schwannomas are not usually considered in the differential diagnosis of pleura masses, and this result in inaccurate preoperative diagnoses. In our series, none of the patients had a definitive preoperative diagnosis. The differential diagnoses of solid tumors include pleural schwannomas, pleura lipomas, solitary fibrous tumor, pleural metastasis, and mesothelioma. The final and exact diagnosis depends on histopathologic testing.
Chest CT is the mainstay imaging technique for the primary assessment of a pleural disease and affords improved sensitivity for the identification process of a malignant pleural process. With the development of advanced cross-sectional imaging techniques in recent years, a CT scan is now capable of showing the size and location of a tumor and aids in surgical planning. Surgical resection is considered the primary treatment for these tumors. Local resection is considered as sufficient treatment for smaller tumors, although thoracoscopy is usually the preferred surgical approach. Larger or more aggressive tumors require resectioning of the pleura (3).
In conclusion, pleural schwannomas are an extremely rare entity. Pleural schwannomas are often found incidentally or are present with vague, non-specific symptoms; the radiologist should remember the possibility of incidental detection during CT scanning of the pleura. Analysis of CT findings from our 11 cases of pleural schwannomas did not provide any specific diagnostic features, although certain findings can be suggestive of this lesion. Schwannomas on CT appear with a well-defined margin, being ovoid or round, and either isoattenuated or hypoattenuated to muscles of the chest walls. Pleural schwannomas should be included in the differential diagnosis of solid, solitary, and well-defined pleural tumors.