
Abstract
Background
Magnetic resonance (MR) arthrography is the ideal imaging modality for the acetabular labrum. Three-dimensional (3D) fast spin-echo (FSE) sequences have similar diagnostic performance as two-dimensional (2D) conventional MR imaging for ligaments, menisci, or bone marrow edema in the knee.
Purpose
To compare the diagnostic accuracy and inter-observer reliability of 3D intermediate-weighted FSE sequence and 2D FSE sequences for the diagnosis of acetabular labral tears.
Material and Methods
Institutional review board approval was obtained and informed consent was waived for 45 patients (47 hips) who underwent 3D and 2D MR arthrography and subsequent arthroscopic surgery. The 3D sequences were performed using volumetric intermediate-weighted fast spin-echo imaging with fat suppression (voxel size, 0.6 × 0.6 × 1.2 mm; imaging time, 6 min 38 s). Labral tear was retrospectively and independently evaluated by two radiologists in four areas of the labrum (anterosuperior, posterosuperior, anteroinferior, and posteroinferior) on 3D and 2D FSE sequences. Statistical differences between the sensitivity and specificity of the methods were analyzed with the McNemar test, using arthroscopic findings as the reference standard. Inter-observer agreement was calculated using kappa statistics.
Results
Arthroscopic findings confirmed labral tears at 40 anterosuperior, 23 posterosuperior, 0 anteroinferior, and 2 posteroinferior quadrants. Sensitivity and specificity were 74% and 89% for 2D FSE sequences, and 78% and 92% for 3D FSE sequences, respectively. Sensitivities and specificities for the methods were not different statistically (P > 0.05). Inter-observer agreement for labral tear was substantial for 2D FSE sequences (k = 0.774) and almost perfect for 3D FSE sequences (k = 0.842).
Conclusion
3D intermediate-weighted FSE MR arthrography is excellent for diagnosing acetabular labral tears. Sensitivity, specificity, and inter-observer reliability were similar to conventional 2D MR arthrography. For evaluation of the labrum, 3D FSE MR arthrography is more time-efficient than 2D FSE MR arthrography.
Keywords
Acetabular labral tear is a significant cause of hip pain and clicking (1–4). Labral tears have been reported in patients without injuries or other abnormalities, as well as in patients with acetabular dysplasia, femoroacetabular impingement, congenital abnormalities, or previous trauma (2, 5, 6). Magnetic resonance (MR) arthrography is the generally preferred imaging modality for evaluation of the labrum, compared to MR imaging (MRI) or multidetector CT arthrography (3, 6–12).
Three-dimensional (3D) MRI can provide multiplanar reformatted images with a single acquisition as well as reduce partial volume averaging by acquiring thin continuous slices (11, 13). 3D gradient-recalled echo (GRE) sequences have been used usually for cartilage in joint imaging and have limited usefulness in the evaluation of other structures such as ligaments or menisci in the knee, and bone marrow edema (13–16). In recent years, studies about the usefulness of 3D fast spin-echo (FSE) sequences have been reported, mostly in the knee. 3D FSE sequences have similar diagnostic performance as 2D conventional MRI for ligaments, menisci, or bone marrow edema (13, 17–21). In the hip joint, evaluation of acetabular cartilage using 3D GRE sequences has been reported (22, 23). However, to our knowledge, no study has described the suitability of 3D FSE sequence at 3.0 T hip MR arthrography for acetabular labral tears. If diagnostic performance of 3D FSE sequences for detecting acetabular labral tear are similar to or better than that of 2D FSE sequences in the hip joint, we could use 3D FSE sequences instead of 2D FSE sequences for the evaluation of acetabular labral tear, and then expect time efficiency because of no need for multiple acquisitions in different planes. The purpose of this retrospective study was to compare the diagnostic accuracy and inter-observer reliability of 3D FSE MR arthrography with 2D FSE MR arthrography at 3.0 T for the diagnosis of acetabular labral tears.
Material and Methods
Patients
Our Institutional Review Board approved this retrospective study protocol, and the requirement for informed consent was waived. Between April 2009 and June 2010, 151 patients with hip pain underwent 155 hip MR arthrographic examinations. Among these patients, 45 underwent arthroscopic surgery in 48 hips, with persistent hip pain despite at least 12 weeks of conservative treatment. The patient group was 18 men (mean age, 42 years; range, 18–65 years) and 27 women (mean age, 47 years; range, 18–69 years). For three patients who underwent hip MR arthrography and arthroscopic surgery in both hips, one hip of one patient was excluded because no 3D oblique reformatted sequence was available. There was no patient with previous hip arthroscopy. Thus, 47 hips of 45 patients were included in this study. On hip plain radiographs, there were no abnormalities in 35 hips of 33 patients, cam type of femoroacetabular impingement with osseous bump formation at the femoral neck in five hips of five patients, mild osteoarthritis with definite osteophytes but unimpaired joint space in five hips of four patients, hip involvement of ankylosing spondylitis with osteophytes but unimpaired joint space in one hip of one patient, herniation pit of the femoral neck and intraosseous ganglion at the edge of the acetabular roof in one hip of one patient, and calcification around greater tro-chanter of femur in one hip of one patient. The interval between MR arthrography and arthroscopic surgery was 2–190 days (mean, 76 days). Arthroscopic surgery was performed by a single orthopedic surgeon with 11 years of experience in hip surgery who knew the MRI results at the time of the surgery.
MRI protocol
Intra-articular injection of diluted contrast material was performed via the anterior approach under fluoroscopic guidance. First, to confirm intra-articular needle placement, a small amount of iodinated contrast agent is injected. For dilute gadolinium contrast agent (0.2 mmol/L), 0.1 mL of gadopentetate dimeglumine is diluted in 20 mL of normal saline solution. A total of 10–15 mL of dilute gadolinium contrast agent is injected in the hip joint. No anesthetic and/or epinephrine were included in the mixture. MR imaging examinations were performed with a 3.0-T system (Achieva; Philips Medical Systems, Best, The Netherlands) using a SENSE Torso coil or SENSE Cardiac coil. The routine protocol for hip MR arthrography at our institution is four 2D conventional sequences and one intermediate-weighted 3D FSE imaging with fat suppression. 2D MR arthrography included coronal T1-weighted FSE sequence, coronal T2-weighted fat-suppressed FSE sequence, sagittal T1-weighted FSE sequence, and axial T1-weighted fat-suppressed FSE sequence. No 2D oblique or radial FSE sequences were performed. The total imaging time for 2D MR arthrography was 11 min. Subsequently, an intermediate-weighted 3D FSE sequence with fat suppression was performed in the axial plane; the total imaging time was 6 min 38 s. Imaging parameters are in Table 1. Reformation of the 3D MR arthrographic images was performed at the imaging workstation by six MR radiographers in turns, immediately after image acquisition, in three parallel planes and one radial direction. Parallel reconstructions were generated in oblique planes with imaging parameters of 3-mm section thickness, 0.3-mm intersection gap, and 25 images (Fig. 1a–c). First, the oblique sagittal plane is oriented along the long axis of the femoral neck on a coronal image. Second, the oblique coronal plane is oriented along the long axis of the ilium with a true sagittal image (1). Third, the last oblique plane is oriented perpendicular to the long axis of the ilium in a true sagittal image. We decided that this last oblique plane was called as the oblique axial plane. Radial reformation (1-mm section thickness, 108 interval, and 36 images) was performed using the sagittal image as the reference image, rotating on the center of the femoral head (Fig. 1d). The time required for image reformation was approximately 1 min 10 s. Because directions of oblique or radial images, thickness, et cetera of 3D images are set in the imaging workstation and some adjusting of exact location or direction is needed, the reformation of 3D image with brief time was possible.
Three parallel reformations and one radial reformation in three-dimensional MR arthrography of the right hip in a 48-year-old woman. (a) Oblique sagittal reformation was performed with orientation along the long axis of the femoral neck on a coronal image. (b) Oblique coronal reformation was performed in the plane parallel to the long axis of the ilium on a true sagittal image. (c) Oblique axial reformation was performed in the plane perpendicular to the long axis of the ilium on a true sagittal image. (d) Radial reformation in 10° increments was performed using the sagittal image as a scout locator, rotating on the center of the femoral head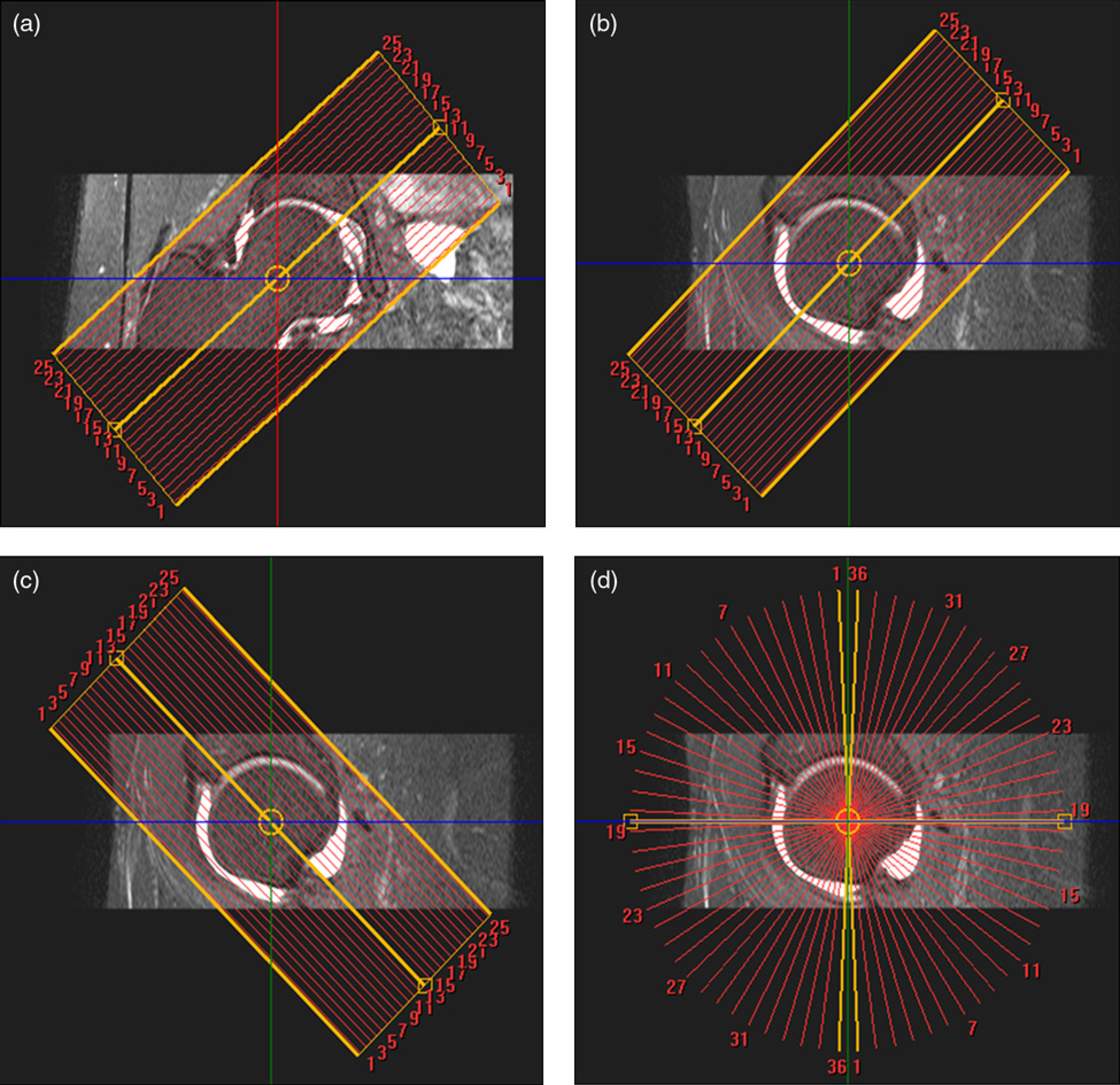
Imaging protocol of hip MR arthrography using a 3.0-T imager

FH, foot-head; RL, right-left
Image analysis
Two musculosketetal radiologists (SYP and JSP, with 4 and 10 years of experience, respectively) who were blinded to the arthroscopic results independently analyzed MR images. First, they reviewed 2D FSE sequences for labral tears, blinded to each other's findings. Two weeks later, they reviewed 3D FSE sequences for labral tears, like the preceding time. After independent reviews of both 2D and 3D FSE sequences, they met and together reviewed the cases with discrepancies in the diagnosis of labral tears, and reached a consensus without knowledge of the arthroscopic findings. The images were evaluated using a picture archiving and communication system (PACS) (PiViewSTAR, INFINITT, Seoul, Korea). Labral tears were diagnosed when there was interposition of contrast material between the labral base and the adjacent acetabular rim or extension of contrast material within the labrum, and the labrum was partially or completely absent (1, 6, 10). Labral tears were evaluated in four areas of the acetabular labrum: anterosuperior, posterosuperior, anteroinferior, and posteroinferior (Fig. 2). If a labral tear extended from one quadrant to another, it was noted in each quadrant. For example, if a labral tear extended from anterosuperior to posterosuperior, it was noted both in anterosuperior and posterosuperior quadrants.
The four quadrants of the acetabular labrum. Anterosuperior, poster-osuperior, anteroinferior, and posteroinferior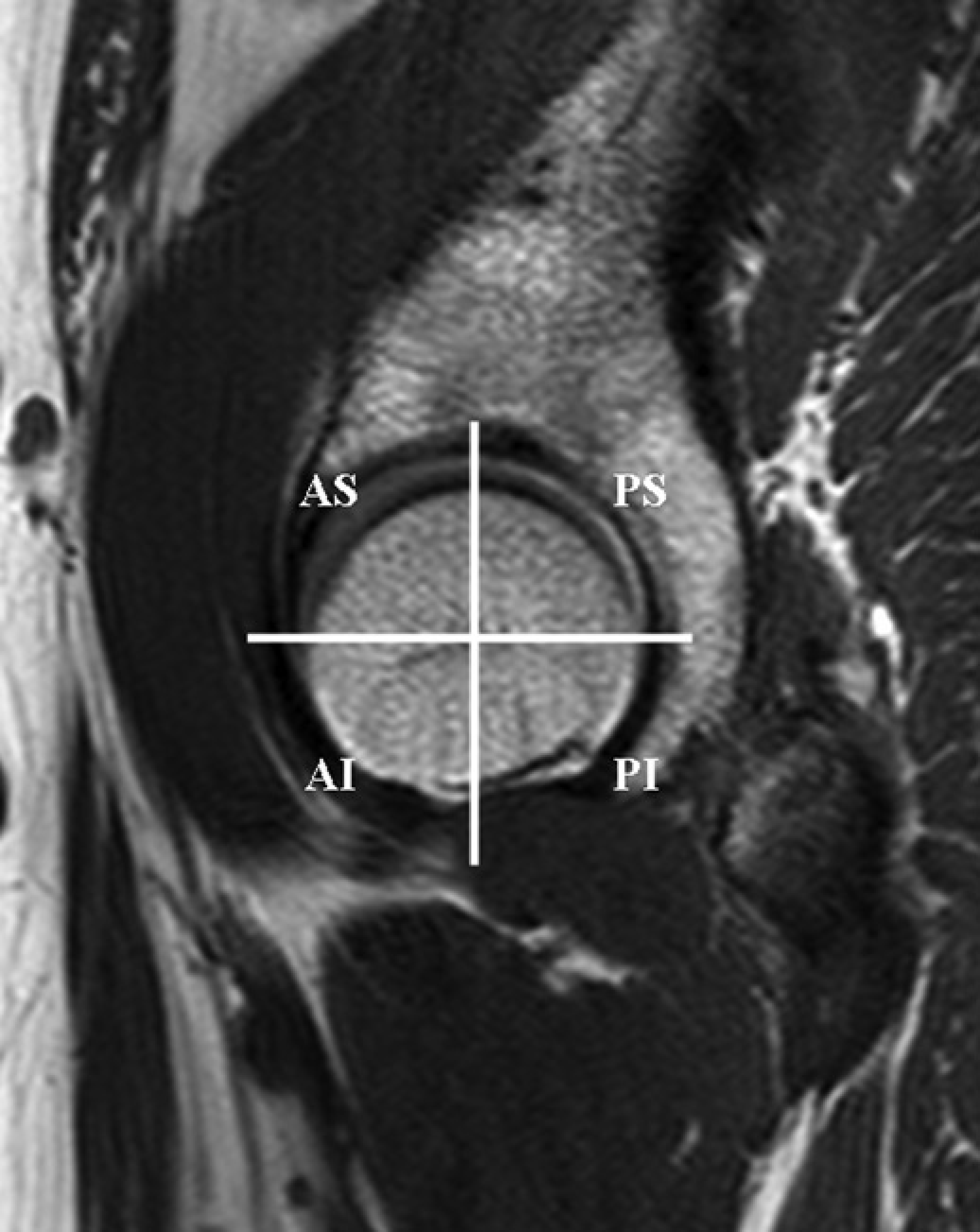
Statistical analysis
Agreement between the two radiologists for the presence or absence of labral tears was examined using κ statistics. A κ value of 0–0.20 indicated slight agreement; κ = 0.21– 0.40, fair agreement; κ = 0.41–0.60, moderate agreement; κ = 0.61–0.80, substantial agreement; and κ = 0.81–1.00, almost perfect agreement (24). K coefficients were calculated and compared using the statistical program MedCalc version 12.1.0 (MedCalc Software, Mariakierke, Belgium). Sensitivity and specificity were calculated and 95% confidence intervals were determined by comparisons to the arthroscopic findings. The McNemar test was applied to determine the statistical differences between the diagnostic performances of 2D and 3D FSE MR arthrographic examinations using the program SPSS version 18.0 (SPSS, Inc., Chicago, IL, USA).
Results
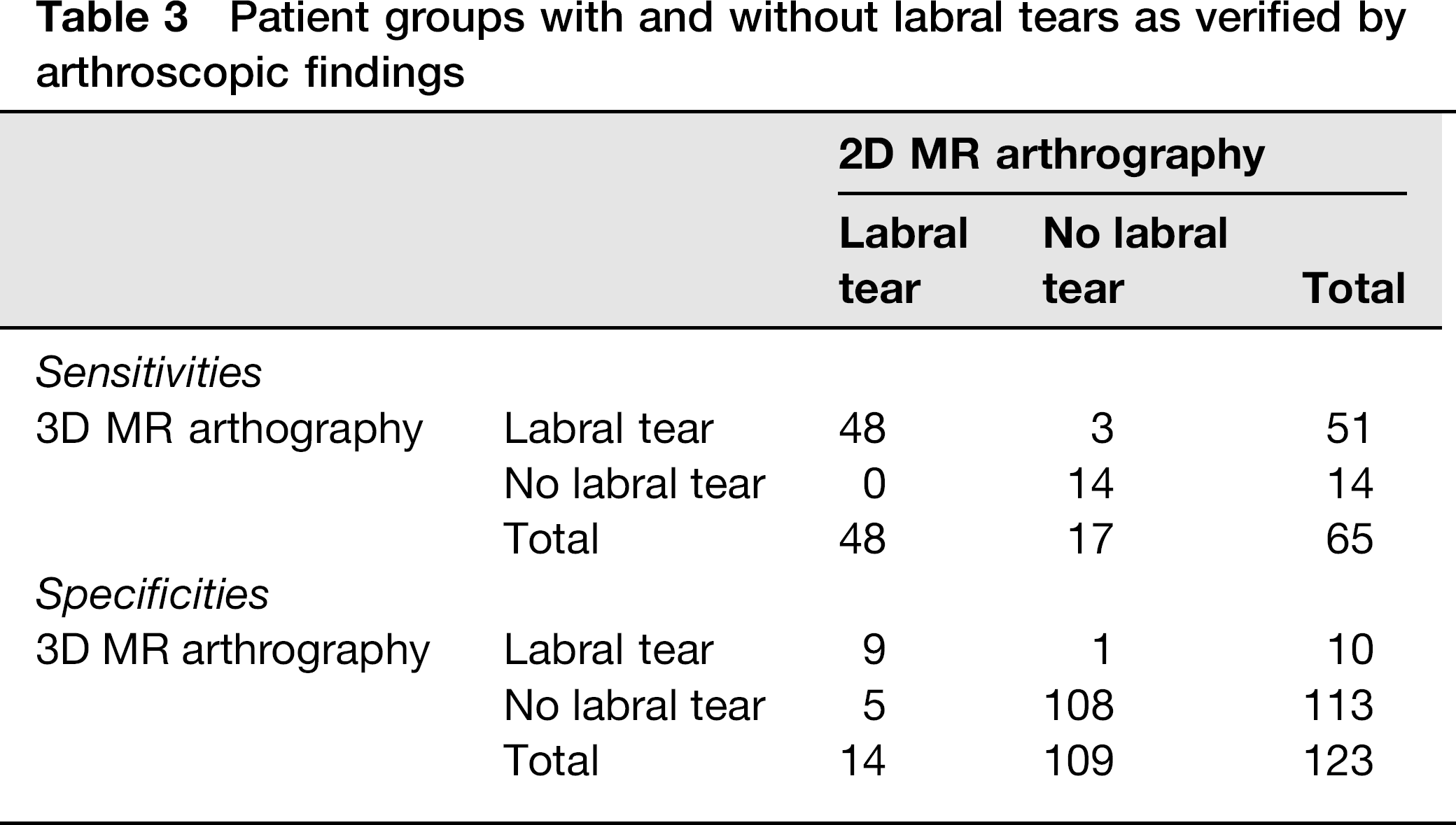
Forty-four of 45 patients had arthroscopically proven labral tears in 46 hips and underwent labrectomy or debridement, with or without shrinkage. One patient did not have a labral tear. In 188 quadrants of 47 hips of 45 patients, arthroscopy revealed labral tears at 65 quadrants, distributed as 40 anterosuperior, 23 posterosuperior, 0 anteroinferior, and 2 posteroinferior. The sensitivity and specificity of 2D and 3D FSE hip MR arthrography are presented in Table 2. By 2D FSE MR arthrography, 48 quadrant labral tears (74%) were correctly diagnosed, and by 3D FSE MR arthrography, 51 (78%) were correctly diagnosed. Of 65 quadrant labral tears, 48 were correctly diagnosed with both 2D and 3D FSE MR arthrography (Fig. 3). Three labral tears were diagnosed with 3D FSE MR arthrography but missed with 2D FSE MR arthrography. These were all posterosuperior labral tears (Fig. 4). No tear was diagnosed with 2D FSE MR arthrography but missed with 3D FSE MR arthrography. Of 123 quadrants without labral tears, five were false-positives by 2D FSE MR arthrography and true-negatives by 3D FSE MR arthrography; these were four posterosuperior and one anteroinferior quadrant. One posterosuperior quadrant was a true-negative by 2D FSE MR arthrography and a false-positive by 3D FSE MR arthrography (Table 3). No significant difference was seen between the diagnostic performances of 2D and 3D MR FSE arthrographic examinations (P > 0.05).
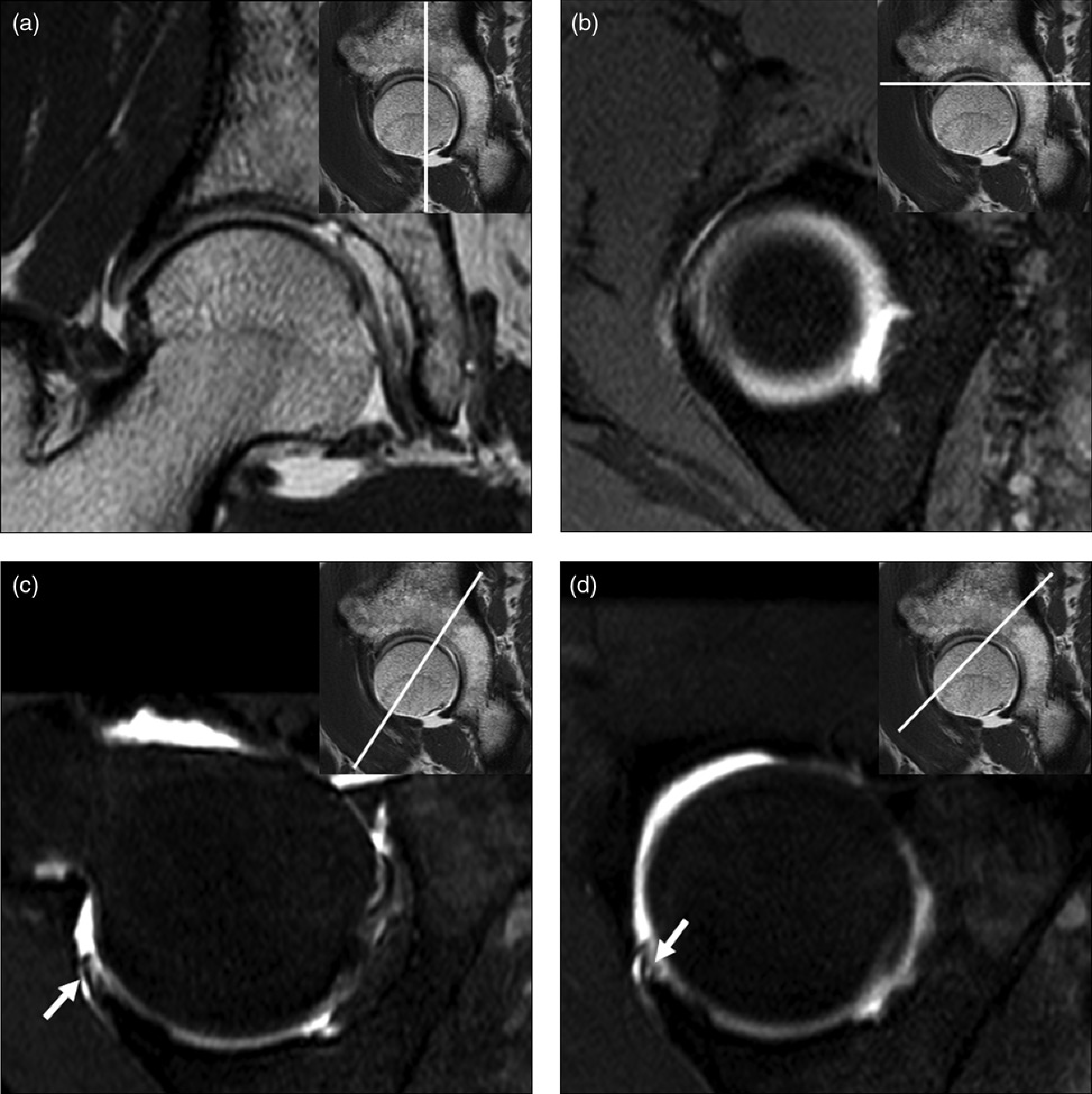
A 44-year-old woman with arthroscopically proven anterosuperior labral tear. T1-weighted fast spin echo sagittal image (a) and fat-suppressed T1-weighted fast spin-echo transverse image (b) show a labral tear with extension of contrast material. 3D MR arthrography with radial reformatted image (c) and with oblique axial reformatted image (perpendicular to the long axis of the ilium on sagittal image) (d) also show labral tears with extension of contrast material A 54-year-old man with arthroscopically proven posterosuperior labral tear. T1-weighted fast spin-echo coronal image (a) and fat-suppressed T1-weighted fast spin-echo transverse image (b) show posterosuperior labrum. No tear at the posterosuperior labrum was diagnosed by both radiologists using 2D conventional sequences. 3D MR arthrography with radial reformatted image (c) and with oblique coronal reformatted image (d) show tear at postero-superior labrum with extension of contrast material
Sensitivity and specificity of acetabular labral tear using 2D and 3D hip MR arthrography
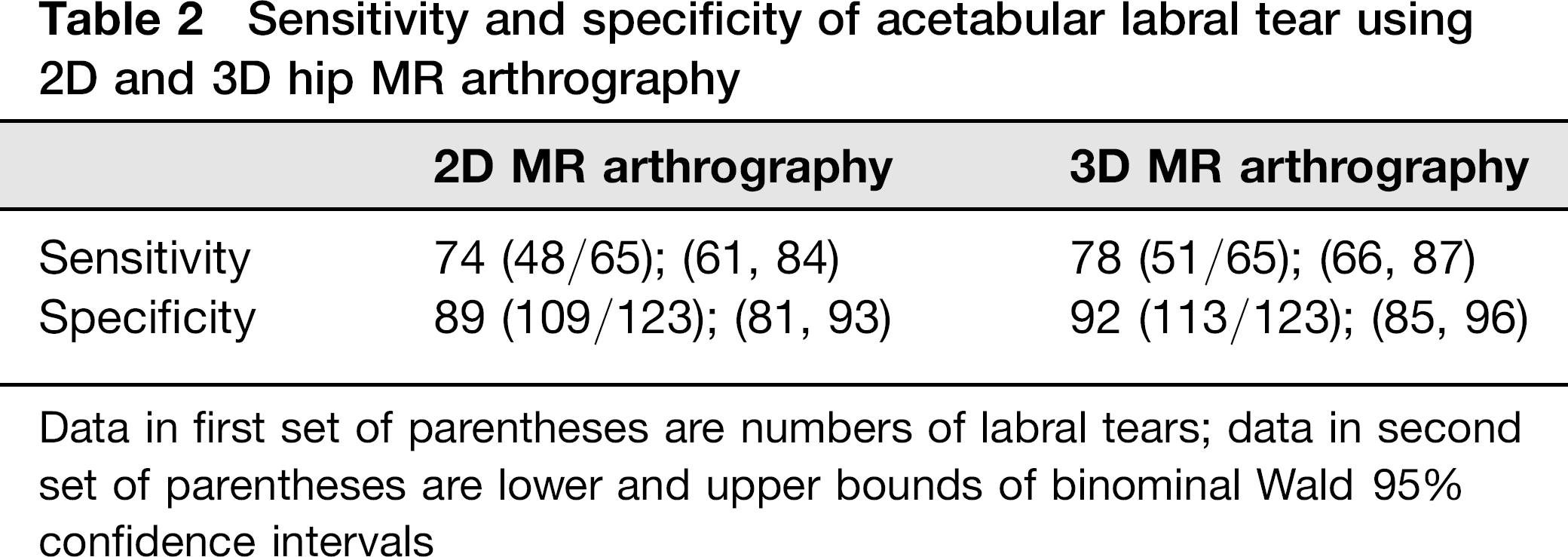
Data in first set of parentheses are numbers of labral tears; data in second set of parentheses are lower and upper bounds of binominal Wald 95% confidence intervals
Patient groups with and without labral tears as verified by arthroscopic findings
The inter-observer agreement for labral tear was substantial for 2D FSE MR arthrography (κ = 0.774; 95% confidence interval: 0.678, 0.870) and almost perfect for 3D FSE MR arthrography (κ = 0.842; 95% confidence interval: 0.759, 0.925). No significant difference was observed between the κ coefficients for 2D and 3D FSE MR arthrography (P = 0.057).
Discussion
The joint MR imaging protocols used at most institutions consist mainly of 2D FSE sequences repeated in multiple planes. With recent improvements in MR technology, 3D sequences with isotropic resolution have become available for joint MRI. This 3D MRI acquires continuous thin-section data through joints with high spatial resolution, minimizing the effects of partial volume averaging. After a single acquisition, multiplanar reformat images in any orientation are available, eliminating the need to repeat sequences with identical tissue contrast in different planes. In the joint imaging, GRE sequence has been usually used for 3D MR arthrography because of imaging time and is useful for cartilage imaging (11, 13). Vastly undersampled isotropic projection (VIPR) steady-state free precession (SSFP) (VIPR-SSFP), one of GRE sequences, is less sensitive than conventional MRI for detecting lateral meniscal tears and bone marrow edema lesions (14). It may be more difficult to detect increased water content within edematous bone marrow when compared with the highly fluid-sensitive fat-suppressed T2-weighted FSE sequences because of potential weakness of the T2/T1-weighted tissue contrast. Lower sensitivity, specificity, and accuracy for meniscal tears, and lower sensitivity for anterior cruciate ligament lesions of 3D GRE sequences than those of 2D SE sequences were reported (15). Higher signal intensity in normal meniscal tissue on 3D GRE images than on the SE sequences might degrade imaging contrast. Recently, several studies have compared 2D and 3D FSE sequences, mainly in the knee joint (11, 13, 17–21, 25–28). Jung et al. (28) reported on the diagnosis of supraspinatus tendon tears with 3D isotropic turbo spin-echo SPACE sequence at 3.0 T shoulder MR arthrography. Although there were reports on 3D GRE MR arthrography for the evaluation of acetabular cartilage, no previous study has compared 2D and 3D FSE MR arthrography to evaluate the acetabular labrum. Our study could be the first to compare 2D and 3D FSE MR arthrographies at 3.0 T to diagnose labral tears.
In our study, the sensitivity and specificity of 3D FSE MR arthrography were slightly higher than those of 2D FSE MR arthrography, although diagnostic performances of the methods were not significantly different. Considering the imaging time, 3D FSE MR arthrography was more efficient than 2D FSE MR arthrography for detecting labral tears. The total imaging time of 2D FSE MR arthrography was 11 min in our study. For 3D FSE MR arthrography, the total imaging time was 6 min 38 s and the time required for image reformation was < 1 min. At our institution, 2D FSE MR arthrography consisted of the minimum sequences with no oblique or radial reformatted images assisting in the diagnosis of labral tears. Thus, more imaging time may be needed for 2D FSE MR arthrography at most institutions. We propose that 3D FSE MR arthrography might replace 2D MR arthrography for assessing the acetabular labrum, thereby reducing 2D FSE sequences by eliminating the need for 2D FSE sequences in multiple planes for labrum evaluation. Therefore, we expect shortening of the imaging time when 3D FSE MR arthrography is used for labrum evaluation, with only two or three 2D FSE sequences for evaluation of periarticular soft tissue or bone.
In previous reports, MR arthrography showed a sensitivity of 63–100% and specificity of 71–100% for detecting acetabular labral tears (9, 29–31). In our study, the 2D MR arthrography sensitivity was 74% and specificity was 89%; the 3D MR arthrography sensitivity was 78% and specificity was 92%. Sensitivity and specificity of both 2D and 3D MR arthrography for labral tears were comparable with those of previous investigations.
Our study has several limitations. First, intermediate-weighted sequences with fat suppression were performed for 3D MR arthrography instead of T1-weighted fat-suppressed sequence. With an intermediate-weighted sequence with fat suppression, differentiating labral tears from degeneration with increased signal intensity in the labrum may be difficult. We experienced this problem in a few cases; however, in most cases, differentiating the two conditions was not difficult because the signal intensity of the contrast material extended into labrum in the labral tears was more intense than that of labral degeneration. In fact, unlike T1-weighted fat-suppressed sequence, an intermediate-weighted sequence with fat suppression may have advantages for visualizing abnormalities in cartilage, bone, and periarticular structures. Second, we did not use isotropic voxel dimensions in 3D MR arthrography for shorter imaging times. However, we believe that the non-isotropic 3D MR arthrography in our study had an image quality sufficient for evaluation of labral tears. Third, we did not use a double oblique orientation technique for the radial reformatted sequence (32–34). The true sagittal image of the hip joint was adopted as scout locator to map the radial reformatted images, rotating on the center of the femoral head. We hypothesized that this might be an easy and relatively accurate method for obtaining perpendicular images of the labrum because the acetabular rim is concave and nearly parallel with the femoral head. With this method, a radial reformatted sequence can be obtained easily in a shorter time than for the double oblique orientation technique. Fourth, 2D oblique or radial FSE sequences were not performed. Three labral tears diagnosed with 3D FSE MR arthrography but missed with 2D FSE MR arthrography, were all posterosuperior labral tears (Fig. 4). These results may be especially affected by no oblique 2D FSE image. Also, field of view was smaller and resolution was lower in 2D FSE sequences than in 3D FSE sequence. Sensitivity, specificity, and accuracy may be affected by no oblique 2D FSE sequence as well as smaller field of view and lower resolution of 2D FSE sequences. So, diagnostic performance of the 3D FSE hip MR arthrography may be overestimated. These drawbacks occurred because this was retrospective study. We actually performed 3D MR arthrography for practical use, to obtain oblique or radial sequences at our institution with shorter imaging time. To shorten imaging time of hip MR arthrography, we performed the minimum sequences of axial, coronal, and sagittal 2D FSE sequences with smaller matrix size that may have the impact on diagnostic image quality. 3D FSE MR arthrography was only for the evaluation of intra-articular pathology such as labrum or cartilage. So, field of view of 3D FSE MR arthrography was smaller. However, 2D FSE MR arthrography was for the evaluation of other structures such as bone, joint, and soft tissue as well as labrum, and field of view was larger. Fifth, we did not evaluate the type or pattern of labral tears. Sixth, the imaging parameters of MR arthrography were not constant for shorter imaging times, variability in patient size, or when using different coils (SENSE Torso coil or SENSE Cardiac coil). Seventh, a single orthopedic surgeon performed the arthroscopy, and arthroscopic findings were used as the reference standard. Misinterpretation or overlooking at arthroscopy can be a source of error because it is operator-dependent. Finally, the study has a selection bias. Only one patient had no labral tear. It is obvious for the study to have a highly selected study population, because only patients who underwent arthroscopic surgery were included. However, labral tears were evaluated in four quadrants of the acet-abulum: anterosuperior, posterosuperior, anteroinferior, and posteroinferior. In the study, there were labral tears in 65 quadrants and no labral tear in 123 quadrants. Specificity was 89% for 2D MR arthrography, and 92% for 3D MR arthrography. As for this result, there may be no problem in diagnosing ‘no labral tear’ as well as ‘labral tear’.
In conclusion, intermediate-weighted 3D FSE MR arthrography is accurate for the diagnosis of labral tears and is comparable to 2D FSE MR arthrography. For evaluation of the labrum, 3D FSE MR arthrography is more time-efficient than 2D FSE MR arthrography. Therefore, 3D FSE MR arthrography could be an alternative to 2D FSE MR arthrography for detecting labral tears.
Footnotes
Acknowledgements
This research was supported by the Program of Kyung Hee University for the Young Researcher of Medical Science in 2010 (KHU-20100758).