
Abstract
Background
Preoperative embolization of tumors is a well-established procedure that has been successfully applied in various clinical situations. Preoperative embolization can reduce the vascularity of tumors resulting in a clearer operative field, less difficult dissection, decreased blood loss, and, in some cases, a decrease in tumor size. However, few studies have been conducted regarding the preoperative embolization of giant thoracic tumors.
Purpose
To examine the effectiveness and safety of interventional embolization of giant thoracic tumors before surgical resection.
Material and Methods
A total of 14 consecutive patients with giant thoracic tumors received angiography and the feeding arteries of the tumors were embolized using polyvinyl alcohol (PVA) particles and gelatin sponges 1 day before surgical resection. The patient records were retrospectively reviewed and data regarding diagnoses, embolization, and surgical resection were recorded.
Results
Angiography revealed the feeding arteries of the tumors to be characterized by multiple branches and thickened vessel trunks with abnormal distal branches superimposed of the tumor shadow. Embolization was successfully without complications in all patients, and all feeding vessels of each tumor were occluded. Embolization reduced the severity of bleeding during surgery and decreased the difficulty of resection of the tumor. No intraoperative or postoperative complications occurred.
Conclusion
Interventional embolization is a safe and efficient method to facilitate the surgical resection of giant thoracic tumors.
Huge thoracic tumors are rare in clinical practice, and surgical resection is difficult and associated with significant intraoperative and postoperative complications (1–3). The blood supply of thoracic tumors is abundant and typically provided by multiple arteries. The trunks of most feeding arteries are thickened, and the distal branches are numerous and tortuous, which can result in massive bleeding intraoperatively that is difficult to control. Significant bleeding can obscure the operative field, increasing the risk of iatrogenic injury and other complications. A second thoracotomy may be necessary for recurrent bleeding. Large intraoperative blood loss and blood transfusions can adversely affect the postoperative recovery (4).
Preoperative embolization of tumors is a well-established procedure that has been successfully applied in various clinical situations (1, 3, 5–8). Preoperative embolization can reduce the vascularity of tumors resulting in a clearer operative field, easier dissection, decreased blood loss, and, in some cases, a decrease in tumor size. However, few studies have been conducted regarding the pre-operative embolization of giant thoracic tumors, presumably because of limited case numbers, a perceived high risk associated with interventional embolization, and difficulties in localizing all of the involved feeding arteries. Embolization of arteries supplying a giant thoracic tumor, as with other tumors, can reduce bleeding during surgery and decrease the difficulty of the surgical resection. Herein we report the results of preoperative embolization of giant thoracic tumors in 14 consecutive patients.
Material and Methods
Patient data
In this retrospective study, the records of 14 patients, eight men and six women, with a diagnosis of giant thoracic tumors who underwent preoperative embolization of the tumors before surgical resection from March 2007 to May 2010, were reviewed. Giant thoracic tumors were defined as tumors with a diameter > 10 cm within the thoracic cavity. The mean patient age was 48.1 years (range, 17–78 years). Patient data are presented in Table 1. All patients had hypervascular tumors.
Patient data
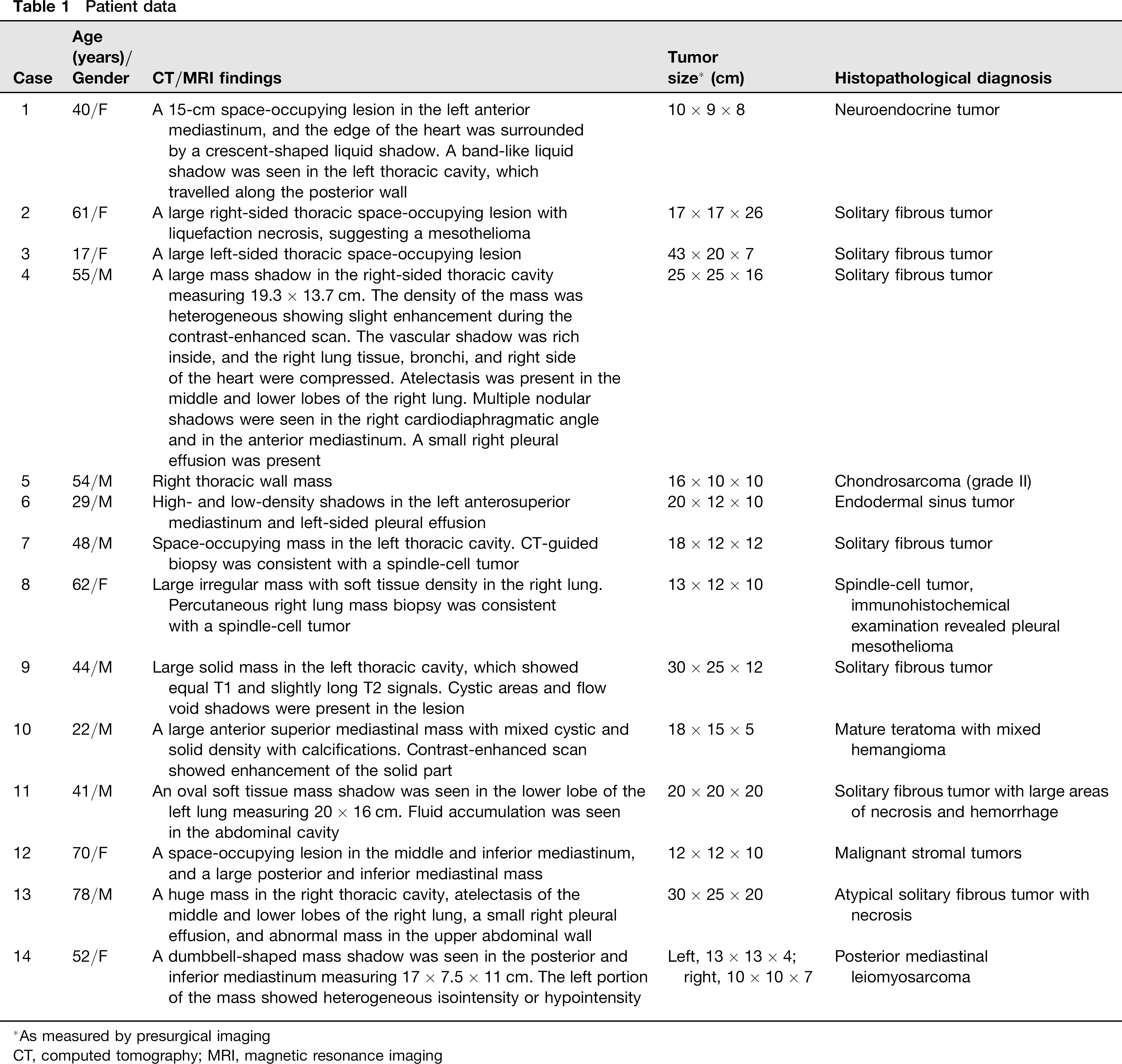
As measured by presurgical imaging
CT, computed tomography; MRI, magnetic resonance imaging
Diagnoses were made by computed tomography (CT) and/or magnetic resonance imaging (MRI). CT-guided biopsy was performed in all patients before surgery. Four patients had tumors in the left pleural cavity, five in the right pleural cavity, three in the anterior mediastinum, one in the middle mediastinum, and one in the posterior mediastinum.
Angiography, embolization, and surgical resection
Angiography using Seldinger's technique was performed in all patients (9). In brief, angiography of the thoracic aorta was performed with a 4F pigtail catheter. Then, Simmon and/or Cobra catheters were used to visualize the intercostal, pleural, inferior phrenic, and bronchial arteries. Angiography was also obtained to visualize the thyrocervical trunk, the thoracoacromial artery, branches of the sub-clavian artery, the lateral thoracic artery, branches of the left hepatic artery, and branches of the left gastric artery in some cases when necessary. Most tumor-feeding arteries were characterized by an increased number of branches and thickened vessel trunks, with blood supplying the area superimposed on the tumor shadow.
Embolization was performed with polyvinyl alcohol (PVA) particles (Contour; Boston Scientific, Natick, MA, USA) 350-500 μm or 500-700 μm in size, and 1 × 1 × 1 mm gelatin sponge particles (Absorbable Gelation Sponge; JINLING Pharmaceutical Co. Ltd., Nanjing, China). Under local anesthesia, superselective catheterization of the tumor-feeding artery was performed using a 4F Simmons or Cobra catheter and the catheter was placed at the proximal opening of the tumor-feeding artery. Then a 3F microcatheter was inserted into the tumor feeding artery and placed at its distal end for embolization. PVA particles and gelatin sponge particles were dissolved in contrast agent and were aspirated in a 2.5 mL syringe and injected into the tumor-feeding artery for embolization via the microcatheter. First, distal branches of the feeding arteries were embolized with the PVA particles, and then the trunks were embolized with the gelatin sponge particles. Prior to injection of embolic material, the angiography images were carefully analyzed in order to observe whether spinal artery branches were present. Spinal artery branches may be derived from the bronchial, intercostal artery, thyrocervical trunk, and costocervical trunk. Differentiation between spinal arteries and the Adamkiewicz artery, which originates on the left side at the level of the eighth thoracic vertebra, is important. Attention should be paid to prevent embolizing spinal arteries mistakenly during the embolization. The embolic material should be injected slowly to avoid embolization of normal tissue caused by reflux. Gelatin sponge was used for embolization at the proximal end of the tumor-feeding artery as that may strengthen the PVA embolization and prevent the impact of proximal blood flow and subsequent PVA reflux. If abnormal blood vessel opening was present or the microcatheter was unable to be placed at the distal end of the tumor-feeding artery, the embolic material could be injected slowly through the 4F catheter. However, real-time fluoroscopy should be carried out and close attention should be paid to observe whether reflux of the embolic material is present. Prior to embolization, the injection pressure was tested using contrast agent in order to prevent ectopic embolization. Embolization was considered complete when no circulation of blood was seen by angiography after embolization. Thoracotomy and resection of the tumor was performed 1 day after embolization. Representative images of case number 14 are presented in Fig. 1.
Representative computed tomography (CT), magnetic resonance imaging (MR), and angiography images of case number 14, which was diagnosed as an posterior mediastinal leiomyosarcoma. (a, b) Axial T2-weighted MRI revealed a solid mass in the left thoracic cavity. A dumbbell-shaped mass shadow was seen in the posterior and inferior mediastinum measuring 17 × 7.5 × 11 cm. The left portion of the mass showed heterogeneous isointensity or hypointensity. (c) Angiographic embolization of feeding arteries. This image shows selective embolization using a catheter
Results
Embolization of 55 tumor-feeding intercostal, 13 internal thoracic, 11 inferior phrenic, five bronchial, and two lateral thoracic arteries was performed in 14 patients. Less common tumor-feeding arteries including two branches of the thyrocervical trunk, one thoracoacromial artery, one branch of the subclavian artery, one branch of the left hepatic artery, and one branch of the left gastric artery were also embolized in the 14 patients. In all cases, angiography showed that all embolized vessels were completely blocked, and no complications were observed during or after embolization in any patient. Sites of embolization are presented in Table 2.
Angiographic data and surgical outcomes
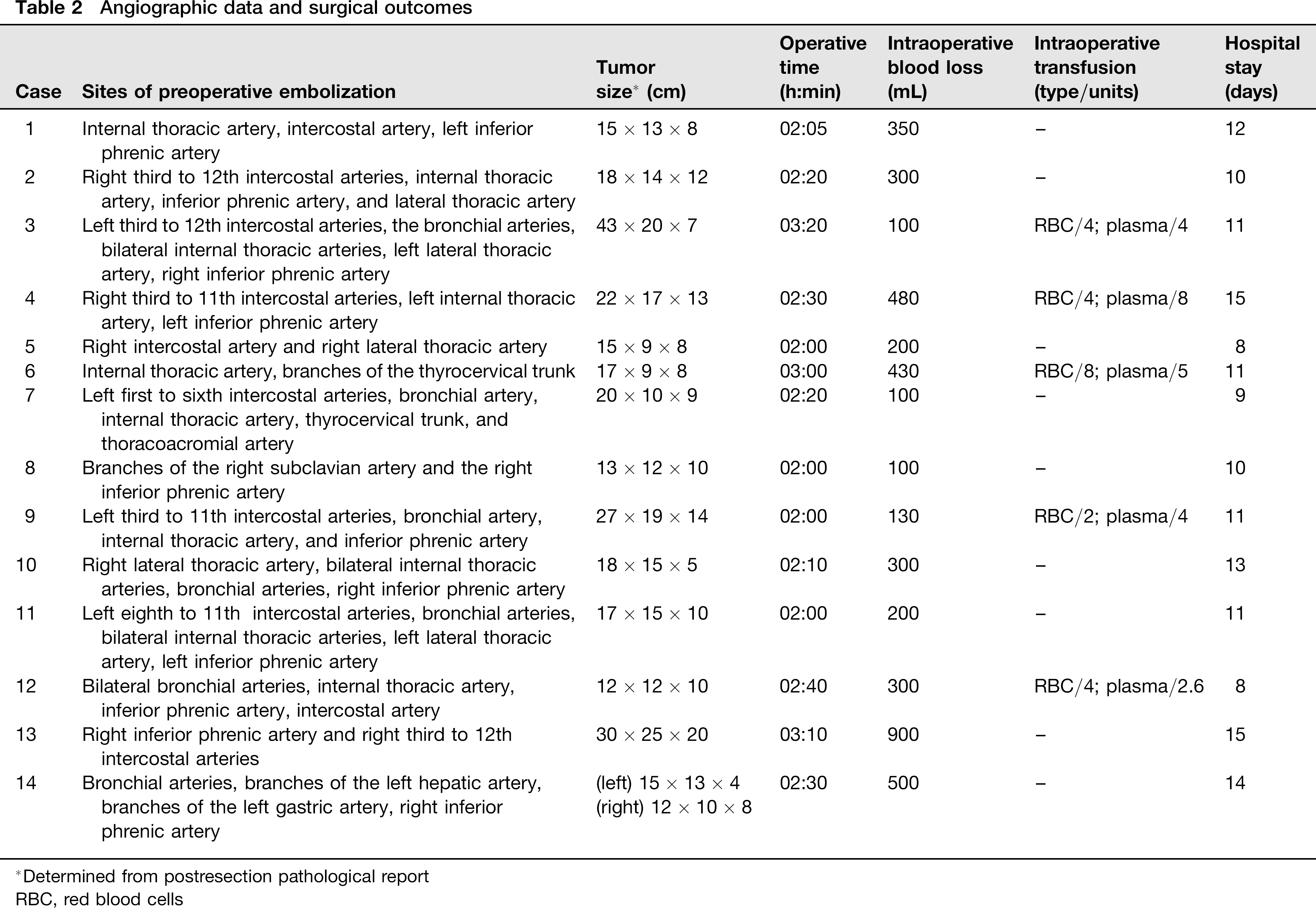
Determined from postresection pathological report
RBC, red blood cells
Operative and histopathological data are presented in Table 2. The average intraoperative blood loss was 314 mL (range, 100–900 mL), and the average operative time was 2.3 h. No intraoperative or postoperative complications occurred. The average hospital stay was 11.3 days. Histopathologically, the type of the tumor varied, with the major type being solitary fibrous tumors of the pleura (SFTP) (n = 6).
Discussion
In this report, we performed embolization of giant thoracic tumors of various etiologies. Embolization was completed without complications in all cases, and the patients tolerated the procedures well. In all cases embolization of the tumor was complete, and the difficulty of surgical resection was decreased because of decreased vascularity of the tumors and reduced bleeding during the surgical resection.
Although currently there is no diagnostic standard, in this study we defined tumors with a diameter > 10 cm as giant thoracic tumors (2, 10, 11). Thoracic tumors can originate from various tissues in the mediastinum, lung, and pleura (1, 3, 12). In this study, patients with giant thoracic tumors were generally young, and approximately one-third of the tumors resected in this study were SFTP. Other tumor types found in this study included neuroendocrine tumors, endodermal sinus tumors, Hodgkin's lymphoma nodular sclerosis type I, and thymoma.
Surgical resection of giant thoracic tumors is difficult, and may be accompanied by blood loss of up to 5000 mL (1, 2). Hemorrhage during surgery can obscure the operative field, extend the operation and recovery times, and result in the need for large transfusions, which also can result in complications and delayed recovery (4). Moreover, bleeding occurring near the intervertebral foramen can result in hematoma formation and subsequent compression of the spinal nerves (5). Postoperative bleeding is also not uncommon, requiring re-operation (2, 3).
Preoperative embolization of tumors is an established procedure and has been used successfully in a number of clinical situations (1, 3, 5–8). Shi et al. (5) reported a series of 18 patients with spinal tumors who underwent preoperative embolization and found that embolization reduced intraoperative bleeding and decreased the difficulty of resection. No complications of the embolization were noted in any patients, and the tumors were completely resected in 17 patients with an average intraoperative blood loss of 1100 mL. Other authors have reported minimization of intraoperative bleeding after preoperative embolization of tumors of the limbs, long bones, and meningiomas (6–8). Guo et al. (13) reported a series of five patients with SFTP where angiography and embolization of the tumor-supplying vessels were successfully performed 24 h within surgery.
Few studies, however, have been conducted regarding the preoperative embolization of giant thoracic tumors, presumably because of limited case numbers, a perceived high risk associated with interventional embolization, and difficulty identifying all of the arteries feeding the tumors. Puma et al. (3) reported three cases of highly vascularized giant thoracic sarcomas, which were embolized 48 h before surgical resection. Tumor size was reduced 20–32% by the embolization, and the authors stated that perilesional edema facilitated surgical dissection of the mass from adjacent tissue in all cases. Robert et al. (1) reported on preoperative embolization of Castleman's disease of the mediastinum and concluded that embolization minimized intraoperative bleeding.
Giant thoracic tumors usually have an abundant blood supply and multiple feeding arteries with numerous branches and thickened vessel trunks (1, 3). To facilitate surgical resection, precise embolization of all of the feeding arteries must be performed, and comprehensive angiography for all potential feeding arteries, including intercostal, internal thoracic, inferior phrenic, and bronchial arteries is required (14). Our results suggest that if all of the vessels supplying the tumor can be completely embolized, intra-operative bleeding, complications, and operation time can be reduced. Extra attention is necessary to determine if any of the feeding vessels are connected with the spinal and cervical vessels, and care must be taken to not embolize the anterior spinal artery, and to prevent embolization material from entering the cerebral and lower extremity arteries (8).
The risk of spinal artery embolization can be minimized in several ways. First, microembolization should be performed to help prevent misembolization. The embolization material should be solid with a diameter > 100 μm and should not overly concentrated (a mixed suspension of normal saline, iodine solution, and the embolic material can be used). Spinal arteries have many branches to the spinal cord, the average diameter of which are approximately 100 μm. The embolization material should therefore have a diameter greater than this to help reduce the risk of inadvertent embolization. Second, the speed of injection should be slow to prevent reflux. Third, during surgery, a contrast agent should be regularly injected to monitor embolization status. Once the feeding artery flow velocity slows, embolization should be stopped. Over-embolization should be avoided to prevent potential occlusion of the spinal cord trunk and consequent ischemia. Finally, a lidocaine spinal cord function induction test should be conducted before surgery. A positive test result, i.e. hypoesthesia and dynamical of the lower extremities, indicates that the bronchial intercostal and spinal root arteries share the same trunk. A coaxial microcatheter can then be used for superselective angiography to enter the bronchial artery and perform embolization.
A number of different materials have been used for embolization of tumors. Gelfoam has been used commonly in the past; however, because of the relatively large particle size, proximal occlusion of large vessels can lead to ineffective embolization. Sundaresan et al. (15) used absolute ethanol for the preoperative embolization of spinal metastases from renal cancer with good results. N-butyl cyanoacrylate and polymethlymethacrylate are commonly used embolic agents (16), and one author has described the use of a detachable balloon to occlude a vertebral artery before surgery for a cervical vertebral tumor Breslau et al. (17). Non-absorbable PVA particles, used in our series, are one of the most frequently used embolic agents reported in the literature. PVA particles 150–250-mm in diameter result in distal embolization with occlusion at the capillary level. Larger particles, 250–500-mm in diameter, can then be used to embolize larger vessels or anastomoses. The use of non-absorbable PVA microspheres might prevent the recurrence of tumor hypervascularity due to recanalization of an embolized artery, which is commonly seen with absorbable gelatin sponges. Complications related to embolization are primarily due to devascularization of areas adjacent to the tumors being embolized, and in regions such as the spine, damage to adjacent areas can lead to permanent loss of functionality (18).
In this study, SFTP were the most common tumor encountered (6/14). SFTP are a firm, encapsulated lobular mass with a characteristic whorled appearance in the benign variety, and a more homogeneous appearance in malignant neoplasms (19, 20). On cut section, there may be areas of hemorrhage and necrosis in both, although calcifications are usually confined to benign tumors. The size may vary from 1 to 36 cm in diameter, with a mean of 6–8 cm, and can weigh as much as 5.2 kg (19, 20). Microscopically, the smaller benign tumors (< 8 cm in diameter) tend to be poorly vascularized with few visible mitoses and uniform elongated spindle cells with variable amounts of collagen and reticular fibers. Larger benign tumors often have greater pleomorphism, but usually < 4 mitoses/10 high-power fields. Malignant SFTPs show increased cellularity with crowding and overlapping nuclei, cellular pleomorphism, and a high mitotic count (> 4 mitoses/10 high-power fields). Malignant tumors commonly have areas of hemorrhage, necrosis, myxo-matous changes, and vascular or stromal invasion. Immunohistochemistry may be useful in differentiating SFTPs from mesotheliomas and sarcomas (19). SFTPs are generally vimentin-positive and cytokeratin-negative, as opposed to mesotheliomas, which are cytokeratin-positive and often vimentin-negative. In addition, both the benign and malignant varieties of SFTPs are CD34-, CD99-, and bcl-2-positive. SFTPs are also generally S-100-, carcino-embryonic antigen-, and smooth muscle actin-negative (19).
SFTP are rare neoplasms that fortunately are benign in 80% of the cases, and are curable with careful, complete resection. Although the less common malignant variety of SFTPs have a higher recurrence rate and higher tumor-related mortality, aggressive surgery and careful postoperative surveillance may still permit long-term survival in as many as 70% of patients (19, 20). After complete resection, chest CT scans should be used to monitor for recurrence every 6 months for the first 2 years, and then yearly. Most recurrences, particularly of the sessile malignant tumors, occur within 24 months of the initial resection. Nevertheless, all SFTP patients need long-term follow-up of 15–20 years due to the possibility of late recurrences. If a local recurrence is detected in any patient, strong consideration should be given for re-resection, which may be curative (20).
In conclusion, the results of this study indicate that pre-operative interventional embolization of giant thoracic tumors is feasible and effective in reducing intraoperative blood loss and decreasing the difficulty of surgical resection, provided that all of the arteries supplying the tumor can be precisely localized. We suggest that this approach may be particularly applicable for the management of hypervas-cular tumors as determined by presurgical contrast enhanced CT or MRI.