
Abstract
Background
Technological advances introduced hand-carried ultrasound (HCU) imagers in daily clinical workflow providing several benefits such as fast bedside availability and prompt diagnosis.
Purpose
To evaluate the diagnostic yield of a latest generation HCU imager compared to contrast-enhanced multidetector computed tomography (MDCT) for the detection of pericardial effusion (PE) in cardiothoracic intensive care unit (ICU) patients.
Material and Methods
Thirty-six patients from a cardiothoracic ICU were enrolled to this study irrespective of their underlying disease. All patients were examined with a new generation HCU for the presence of PE. Definite diagnosis of PE was based on findings of MDCT as standard of reference. Statistical analysis was performed using PASW 18.
Results
PE was identified in 20 patients by MDCT (prevalence 56%). The HCU examination was carried out technically successfully in all patients. Sensitivity, specificity, positive and negative predictive value of HCU for the diagnosis of PE were 75%, 88%, 88%, and 74%, respectively.
Conclusion
HCU provides rapid, practical, reliable, and cost-effective diagnosis of PE in patients on cardiothoracic ICU.
Keywords
For patients in the intensive care unit (ICU) pericardial effusion (PE) is a common complication soon after cardiothoracic surgery and its incidence is dependent on the timing of the examination after surgery and is reported to be as high as 85% (1,2). As an even more severe complication for patients in the cardiothoracic ICU, an early cardiac tamponade is depicted in up to 6% of patients after cardiac surgery, in most cases owing to postoperative bleeding (3), whereas late cardiac tamponade is less frequent (4,5). Furthermore, PE occurs in up to 21% of patients suffering from cancer and these patients do also often present with cardiac tamponade (6).
Since 1954, when introduced by Edler and Hertz (7), the diagnosis and evaluation of PE has been based on echocardiography, which is the most effective non-invasive tool for the evaluation of pericardial fluid accumulation (8–10). However, the bulkiness and heaviness of ultrasound machines limited their bedside use for a long time (11,12) and the first portable ultrasound imagers had limitations in functionality and image quality and even missed important clinical findings (13).
Nowadays, further technological advances generated miniaturized ultrasound systems, leading to the introduction of hand-carried ultrasound (HCU) imagers in daily clinical workflow. Principal advantages of modern HCU devices are fast bedside availability and excellent transportability allowing prompt diagnosis and immediate therapeutic measures combined with low costs (14–17). The disposability of an HCU device and its easy transportability might fasten up the diagnosis of PE or cardiac tamponade at the bedside in the cardiothoracic ICU and help save precious time in coping with urgent situations.
Therefore the aim of the study was to evaluate the diagnostic yield of a latest generation HCU imager compared to contrast-enhanced multidetector computed tomography (MDCT) for the detection of pericardial effusion in cardiothoracic ICU patients.
Material and Methods
Patients
From February 2011 to April 2011 a total of 36 consecutive patients admitted to a cardiothoracic surgery ICU for whom a MDCT scan was ordered by their ward physician were examined additionally with HCU for the presence or absence of PE, irrespective of their underlying disease. There was no exclusion criterion. All patients enrolled to the study were examined at the core service hours of the Department of Radiology, i.e. 08:00 to 17:00 on working days and the ultrasound examination was performed by only one examiner (SS). Study participant operators (SS, FP) were neither aware of the indication for the contrast-enhanced MDCT nor of patients’ underlying disease. In Table 1 patients’ basic demographic data are reported. Informed consent was obtained for all patients. The study was approved by our institution's ethics committee (Ethics Committee of the Medical Faculty, University Medical Center Regensburg, Germany).
Basic demographic characteristics of enrolled patients

Contrast-enhanced multidetector CT scan
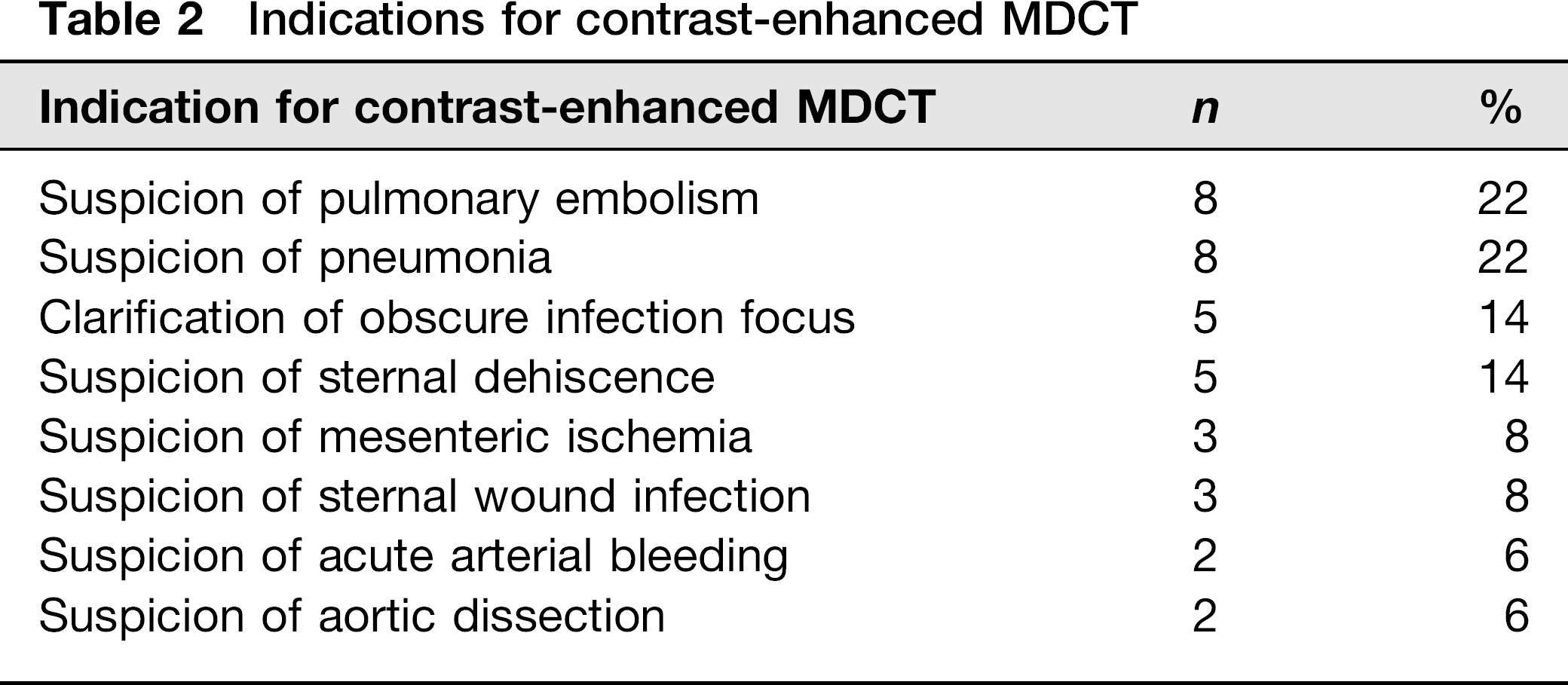
Indications for contrast-enhanced MDCT scan are reported in Table 2. According to standardized examination protocols, all scans were acquired either on a 16-slice CT (SOMATOM Sensation 16, Siemens Healthcare AG, Erlangen, Germany) or on a 128-slice CT (SOMATOM Definition Flash, Siemens Healthcare AG, Erlangen, Germany) after intravenous contrast medium injection of 70–120 mL Accupaque 300 (GE Healthcare, Waukesha, WI, USA) or 60–100 mL Ultravist 370 (Bayer Vital GmbH, Leverkusen, Germany), respectively. MDCT scans were evaluated for the presence or absence of PE, and the amount of PE was furthermore visually assessed, by the same radiologist (FP), specialized in cardiopulmonary imaging for 4 years who was unaware of the ultrasonographic or clinical findings.
Indications for contrast-enhanced MDCT
Chest ultrasound with hand-carried ultrasound
The ultrasound examination was carried out using a modern HCU device (VScan, GE Healthcare, Waukesha, WI, USA) providing a plane 1.7–3.8 MHz transducer for two-dimensional imaging and a 3.5-inch color LCD display. The weight of this imager is 390 g and the maximum scan time with fully charged batteries is approximately 1 h. A picture of the HCU device is shown in Fig. 1. The chest ultrasononographic studies with the HCU imager were performed just prior to the acquisition of the contrast-enhanced CT scan, when the patient was already lying on the CT table. To standardize and simplify the ultrasonographic examination each patient was examined in supine position when the patient was lying on the CT table. This course of examination was chosen in order to adapt the conditions of examination to the settings in patients on ICU. Assessment of pericardial effusion was made with B-Scan two-dimensional imaging in standard views parasternal long- and short-axis, apical four-chamber view, and subcostal views. PE appears as an anechoic stripe around the heart. Few amounts of PE appear as a thin stripe inside the pericardial space, not extending fully around the heart. Pitfalls in the assessment of PE are that few amounts of PE should not be confused with the pericardial fat pad, and that PE in general may not be mistaken for pleural effusion (18).
Image of the study hand-carried ultrasound device (VScan, GE Healthcare, Waukesha, WI, USA) with kind permission of Mr Bastian Werminghoff (GE Healthcare Germany, Munich, Germany)
The operator (SS) was a radiologist with the knowledge of more than 1000 documented ultrasound examinations within the last year under the supervision of an experienced ultrasound examiner who has conducted > 5000 ultrasound examinations every year for > 10 years. Moreover, the operator was unaware of the MDCT scan results or the clinical findings.
Statistical analysis
Data were acquired using Excel tables (Excel 2007, Microsoft, Redmond, WA, USA). Statistical analysis was performed using PASW 18 (PASW V.18, IBM SPSS Inc., Armonk, NY, USA). Agreement between the findings of HCU an MDCT as standard of reference was assessed from 2 × 2 tables.
Results
HCU was carried out technically successful in all 36 patients. Mean scanning time with HCU was 1.5 min with a range of 1 -3 min.
Contrast-enhanced MDCT scan depicted PE in 20 of 36 patients, hence, prevalence of PE was calculated to be 56%.
Examination with HCU (Fig. 2) revealed PE correctly in 15 of 20 patients (75%). In the remaining five cases in whom HCU was false-negative, the amount of PE visually assessed on the MDCT scans revealed < 20 mL of PE in all five cases. These small amounts of PE were considered to be either physiologically or at least hemodynamically irrelevant.
Congruent finding of a large PE by HCU and contrast-enchanced MDCT scan in a 74-year-old male patient 4 days after cardiac valve prosthesis for whom a contrast-enhanced chest MDCT scan was ordered for the clinical suspicion of sternal wound infection. (a) Contrast-enhanced MDCT scan: PE is marked between arrows; (b) B-Scan HCU image (subcostal view): PE is marked between arrows
The absence of PE was correctly verified by HCU in 14 of 16 (88%) patients. HCU was false-positive in two cases in whom the amount of PE was estimated to be < 20 mL, respectively. These small amounts of PE were considered to be physiologically or at least hemodynamically irrelevant as well.
Overall, sensitivity, specificity, positive and negative predictive value of HCU for the diagnosis of PE were 75%, 88%, 88%, and 74%, respectively.
The results of diagnosis of PE by means of HCU are summarized in Table 3.
Sensitivity, specificity, positive (PPV) and negative (NPV) predictive value for the diagnosis of pericardial effusion (PE) using hand-carried ultrasound with MDCT as standard of reference

Discussion
The introduction of HCU imagers has been discussed controversially for image quality and decisionmaking in daily clinical practice, as earlier studies reported drawbacks of older portable ultrasound systems (19).
Recent studies (15,19) have been using other HCU imagers, such as the Acuson P10 (Siemens Healthcare, Erlangen, Germany) or the OptiGo (Philips Medical Systems, Andover, CA, USA) as well as the Sono-Heart (SonoSite Inc., Bothell, WA, USA) and disclosed promising findings, but HCU imagers have not made their way into daily clinical workflow yet.
The present study was performed with a latest generation HCU device (VScan, GE Healthcare, Waukesha, WI, USA) with a plane 1.7–3.8 MHz transducer for two-dimensional imaging and a 3.5-inch display. The tested device proved good handling and image quality as well as quickness of use. It was evaluated before for its image quality in echocardiography by Prinz and Voigt (19) with satisfying results. But, to the best of our knowledge, it has not been investigated in the assessment of PE yet.
Therefore, in the present study the yield of this new generation HCU imager for the diagnosis of PE was evaluated with contrast-enhanced MDCT as standard of reference.
Prevalence of PE was 56% in our study population, which is comparable to the corresponding literature (1,2). Sensitivity and specificity for the diagnosis of PE by means of HCU were 75% and 88%, respectively, which is promising, in particular in consideration of the fact, that in all false-negative cases, the amount of PE was estimated to be 20 mL or less. As the pericardial cavity normally contains approximately 15–35 mL of pericardial fluid, these few amounts of PE of <20 mL have to be considered to be either physiologically or at least hemodynamically irrelevant (20).
There are limitations of the present study. Only 36 patients were enrolled, and the examination with the HCU as well as the reading of the MDCT was carried out by only one operator, respectively. Naturally ultrasound is an operator-dependent modality and different operators might gain different results. Furthermore all patients were admitted to a cardiothoracic ICU with a self-evident high prevalence of PE.
In conclusion, the findings of this study indicate that modern HCU imagers provide a helpful approach for easy, reliable, and cost-effective detection of PE. Systematic use of HCU might improve surveillance of patients who are at risk of suffering from PE and it might help to diagnose PE before it becomes clinically relevant. Abandonment of radiation and quick bedside availability without the need of transportation are further advantages of patient surveillance by HCU systems.