
Abstract
Background
Erythromycin is not only a potent antibiotic; it also has effects of reduction of inflammation and suppression of protein synthesis.
Purpose
To evaluate the impact of erythromycin on tissue hyperplasia after stent placement in a rat esophageal model.
Material and Methods
A total of 21 rats were included. After placement of self-expanding stents in the mid esophagus, the rats were divided into two experimental groups and one control group. The rats in the experimental groups received daily intraperitoneal injections of erythromycin for 5 weeks; 4 mg/kg (group A, n = 7) and 8 mg/kg (group B, n = 7). Those in the control group (n = 7) received 1 mL of saline intraperitoneally. After sacrifice, histologic analysis was done for thickness of the papillary projection, granulation tissue area, percentage of granulation tissue area, and degree of inflammatory cell infiltration. The statistical significance of differences between groups was assessed by Mann-Whitney U test.
Results
Tissue hyperplasia as reflected in thickness of papillary projection, granulation tissue area, and percentage of granulation tissue area, was higher in the control group than in the experimental groups, although there was no statistical significance (P = 1.00, 0.332, and 0.263, respectively). However, degree of inflammatory cell infiltration was significantly lower in the experimental groups than the control group (P = 0.025), and the higher dosage of erythromycin reduced inflammatory cell infiltration significantly (P = 0.037).
Conclusion
Intraperitoneal administration of erythromycin is very effective in reducing inflammation after stent placement in a rat esophageal model but has no significant effect on granulation tissue formation.
Stent-related tissue hyperplasia is a substantial obstacle to successful stent placement in non-vascular luminal organs such as the esophagus, trachea, and urethra (1–3). Tissue hyperplasia can foster restenosis and stent blockage and make it difficult to remove the stent, thus requiring stent replacement or even surgical removal (1, 4). The development of stent-related tissue hyperplasia consists of early inflammatory and late proliferative phases (5). The early inflammatory phase occurs shortly after injury or trauma during stent implantation. This damage triggers the production of inflammatory cytokines and growth factors, which in turn may be responsible for the recruitment and proliferation of inflammatory cells (macrophages and/or monocytes). The late proliferative phase is characterized by the proliferation of fibroblasts and myofibroblasts, and exuberant fibrosis. Thus many cytokines and growth factors, as well as granulation tissue, are involved in the tissue hyperplasia (5).
Macrolides, such as azithromycin, erythromycin, and roxithromycin, are potent antibiotics but also have other effects, namely reduction of inflammation, suppression of protein synthesis in fibroblasts, and inhibition of collagen proliferation (6, 7). It seemed possible therefore that erythromycin might inhibit or prevent tissue hyperplasia after stent placement and thereby improve the patency of stents.
Recently reduction of restenosis using stents coated with anti-proliferative medication has been reported (8–10). However, there has been no report of macrolide antibiotics decreasing stent-related tissue hyperplasia. Therefore, the purpose of this study was to evaluate the impact of erythromycin on tissue hyperplasia after bare metallic stent placement in a rat esophageal model.
Material and Methods
This study was approved by the animal research committee of our institution. All rats were maintained in conformity with the Guide for the Care and Use of Laboratory Animals (11).
Animals
A total of 21 male 9-week-old Sprague-Dawley rats weighing 300–350 g were included in this study. The animals were acclimatized for at least 7 days before the start of the experiments. All 21 rats were maintained on rodent feed and water ad libitum at 24 ± 1°C, 55 ± 10% humidity and a 12-h light/dark cycle under specific pathogen-free conditions. They were divided into two experimental groups of seven rats each and a control group of seven rats.
Esophageal stent placement
A self-expandable stent was placed in all rats, which was woven from a single thread of 0.127-mm-thick nitinol wire filament into a tubular configuration with six bent points on the upper and lower end portions. To encourage tissue hyperplasia through the stent wires, the stent was not covered. Gold markers were attached to either end of the stent to enhance radiopacity, and two barbs were located in the central area of the stent to prevent its migration. When fully expanded, the stent was 5 mm in diameter and 15 mm in length with a small mesh gap of 1.02×1.87 mm. It was made to our specifications by a local medical company (Taewoong, Gimpo, Gyunggi, Korea).
Anesthesia was induced using intramuscularly administered ketamine hydrochloride (50 mg/kg; Yuhan Pharm. Co., Seoul, Korea) and 2% xylazine (0.1 mL/kg; Rompun, Bayer, Leverkusen, Germany) and was maintained throughout the procedure. Each esophageal stent introducer set consisted of a 6-F sheath with a dilator (Cook Medical Inc., Bloomington, IN, USA) was inserted through a custom-made mouthpiece (made of a 1-mL syringe with a hole in the middle), and a 4-F sheath was inserted under fluoroscopic guidance until its distal tip reached the lower esophagus. The sheath was then withdrawn until the distal tip was located at the level of clavicle, and the guide wire was removed. Esophagograms were obtained using an ionic contrast medium (Telebrix 30 Meglumine, Guerbet, Aulnay-sous-Bois, France) injected through the 4-F sheath, to determine the optimal location for stent placement. Normal esophageal diameter was about 3 mm on the esophagograms.
After an esophagogram was made, the 6-F sheath was advanced until its distal tip reached the lower esophagus. With the sheath in place, the guide wire was removed. The stent was then compressed until it fit into the distal end of the sheath. The stent was advanced through the sheath into the esophagus using a pusher catheter, and the sheath was withdrawn while the pusher catheter was held immobile. The stent was deployed at the level of the mid-thoracic esophagus with the upper stent margin positioned at the clavicle under fluoroscopic guidance. The sheath and the pusher catheter were withdrawn from the esophagus after stent placement. A postprocedural fluoroscopic check was performed immediately after stent placement to verify the stent position, and a follow-up esophagogram was made before each rat was killed, 5 weeks after the stent placement, to verify patency.
Administration of erythromycin and follow-up
The experimental groups received intraperitoneal erythromycin (Sigma-Aldrich, St Louis, MO, USA) once a day for 5 weeks after stent placement; 4 mg/kg in group A and 8 mg/kg in group B. The control rats were intraperitoneally injected with 1 mL of normal saline (0.9% w/v sodium chloride) once a day for 5 weeks.
During the follow-up, information on dietary consumption, weight change, and behavior was obtained.
Histological examination
The rats were killed with an overdose of xylazine hydrochloride 5 weeks after stent placement. Thereafter regions of the esophagus including untreated tissue 2 cm proximal and distal to the stent were removed surgically. Gross examination was performed to evaluate tissue hyperplasia and esophageal injury such as perforation or inflammation. The tissue samples were fixed in 10% neutral buffered formalin for 24 h, and the samples were sectioned transversely at three different levels, i.e. proximal, middle, and distal portions of the stented segment. The stents were then gently removed and the samples stained with hematoxylin and eosin.
By microscopic examination, the thickness of the papillary projection (the height of tissue protrusion into the lumen in millimeters), the granulation tissue area (in mm2), the percentage of the granulation tissue area (calculated as 100× (1-[stenotic lumen area/original lumen area]), and the degree of submucosal inflammatory cell infiltration (mild, 1; mild to moderate, 2; moderate, 3; moderate to severe, 4; and severe, 5) were evaluated. Original lumen area was calculated using holes which were made by initially deployed stent struts. For histological analysis, observer was blinded to group attribution. Triple measurements were made on each cross-section for each tissue sample and average values obtained.
Microscopic analysis of the esophagus was performed at ×12.5 and ×400 magnification. Measurements were carried out with TOMORO analySIS TS Lite (Step-By-Step, Techsan Digital Imaging, Seoul, Korea).
Statistical analysis
The Mann-Whitney U test was performed to evaluate the significance of differences between the groups using SPSS software (SPSS, version 15.0; Chicago, IL, USA). A P value <0.05 was considered statistically significant.
Results
Stent placement was technically successful in all the rats, and there were no procedure-related complications. None of the stents migrated, and the 5-week follow-up esophagograms showed good stent patency in all rats. Dietary consumption, weight change, and behavior during follow-up were normal in the control and experimental groups. All the rats were successfully followed up. No perforation occurred in any of the rats during stent placement or follow-up. The excised specimens showed tissue hyperplasia through the meshes, and all the stents were incorporated into the wall of the esophagus, as seen by gross examination.
The histologic findings are summarized in Table 1. Granulation tissue formation was observed in the stent-implant sections in all rats, except for three of the rats in group B. Tissue hyperplasia as reflected in thickness of papillary projection, granulation tissue area, and percentage of granulation tissue area, there were no statistically significant differences between the control and experimental groups (P = 1.00, 0.332, and 0.263, respectively) and between the group B and group A (P = 0.655, 0.406, and 0.655, respectively). With regard to degree of inflammatory cell infiltration, however, there was a statistically significant difference between experimental and control groups; inflammatory cell infiltration in the control group was more extensive than in the experimental groups (4.04 ± 0.59 vs. 3.42 ± 0.60; P = 0.025), and the higher dosage of erythromycin reduced inflammatory cell infiltration more than the lower dosage (P = 0.037) (Figs. 1–3).
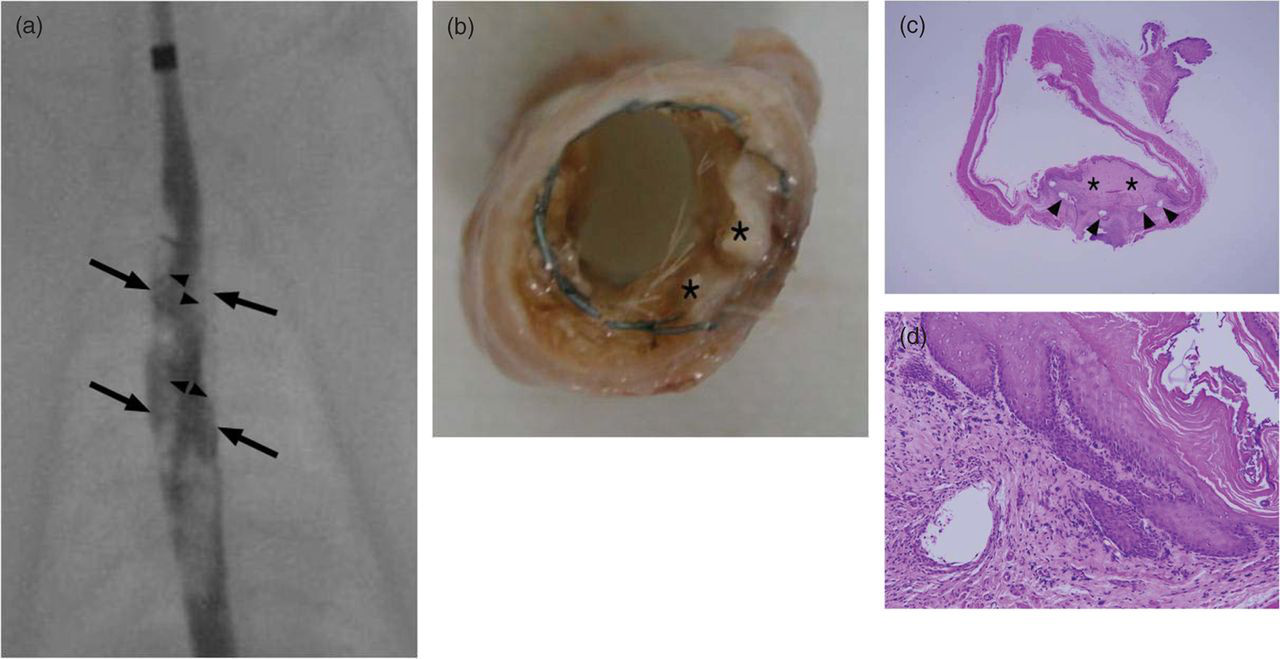
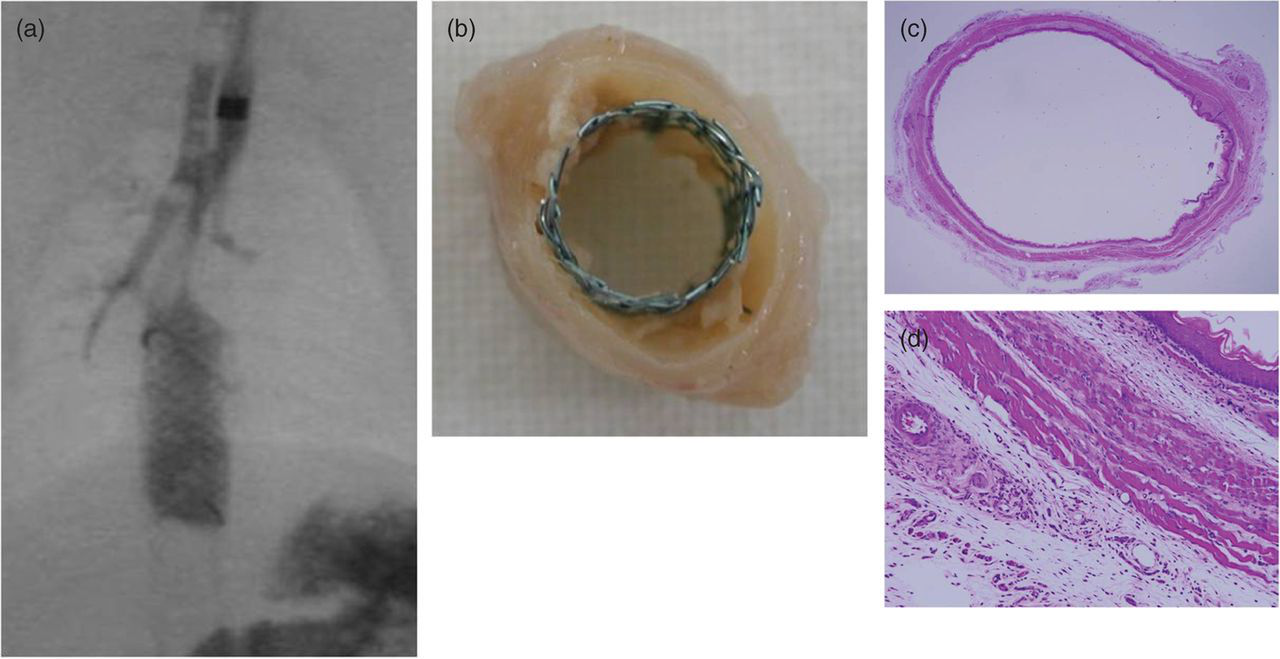
Representative esophagogram and histologic images of control rats. The stent was originally deployed at the slightly lower level of distal esophagus. The esophagogram (a) made immediately before sacrifice shows a gap between the contrast filling (arrow heads) and the stent wires (arrows) indicative of tissue hyperplasia. The histologic section (b) and corresponding microscopic image (c) show clear-cut tissue hyperplasia (asterisks) penetrating the meshwork of the stent. The area of the granulation tissue was 9.21 mm2. The stent struts are seen as holes (arrowheads). The high-power microscopic image (hematoxylin and eosin staining, x 200) (d) reveals inflammatory cell infiltration of grade 4 Representative esophagogram and histologic images of group A rats administered 4 mg/kg doses of erythromycin. The esophagogram (a) immediately before sacrifice shows the gap between contrast filling (arrow heads) and the stent wires (arrows), thus indicating tissue hyperplasia. A histologic section (b) and corresponding microscopic image (c) show definite tissue hyperplasia (asterisks) penetrating the meshwork of the stent. The area of the granulation tissue was 5.1 mm2. Stent struts are seen as holes (arrowheads), and the high-power microscopic image (hematoxylin and eosin staining, ×200) (d) shows inflammatory cell infiltration of grade 3 Representative esophagogram and histologic images of group B rats administered doses of 8 mg/kg erythromycin. The esophagogram (a) made immediately before sacrifice shows complete contrast filling within the stent, indicating absence of tissue hyperplasia. During the contrast injection, small amount of contrast material was aspirated inadvertently into trachea and bronchi. The absence of tissue hyperplasia is confirmed by the histologic section (b) and corresponding microscopic image (c). The high-power microscopic image (hematoxylin and eosin staining, ×200) (d) shows inflammatory cell infiltration of grade 2 Comparison of histologic findings in control and experimental groups *Mann-Whitney U test
†Inflammatory cell infiltration in the submucosa: 1, mild; 2, mild to moderate; 3, moderate; 4, moderate to severe; 5, severe Values are means ± SD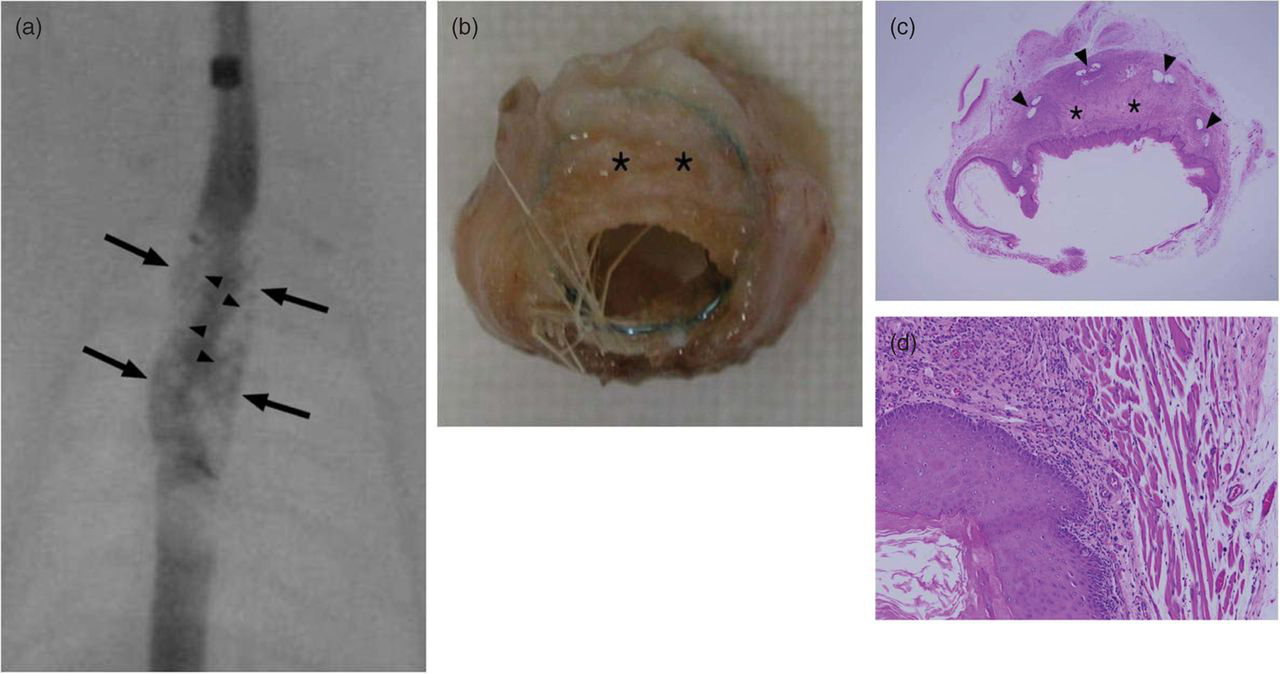
Discussion
In our study, 5 weeks of treatment with intraperitoneal erythromycin had a significant impact on submucosal inflammation.
Formation of stent-related tissue hyperplasia involves early inflammatory and late proliferative phases (5). The early inflammatory phase occurs shortly after injury or trauma during stent implantation, which triggers the production of inflammatory cytokines and growth factors and in turn may be responsible for the recruitment and proliferation of inflammatory cells (macrophages and/or monocytes). The late proliferative phase is characterized by proliferation of fibroblasts and myofibroblasts and exuberant fibrosis (5).
Macrolide antibiotics such as azithromycin, erythromycin, and roxithromycin, have multiple biologic effects on monocytes and macrophages, and inhibit the production of inflammatory cytokines such as interleukins and tumor necrosis factors (2, 6). Recently, it has been reported that erythromycin reduces transforming growth factor-beta (TGF-ß) gene expression and type IV collagen production (12). TGF-ß is a multifunctional inflammatory mediator that regulates chemotaxis (for monocytes, lymphocytes, neutrophils, and fibroblasts), angiogenesis, production and remodeling of extracellular matrix, and proliferation of epithelial cells and fibroblasts (6, 13). TGF-ß play a role in the transition from the inflammatory phase to the proliferative phase in the wound healing process (13). It is also responsible for aspects of wound scarring, fibroblast proliferation, and collagen production. Numerous studies have supported a role of TGF-ß as a fibrogenic cytokine that evokes pathologic fibrosis in various organs (14–17). High-level expression of TGF-ß and deposition of extracellular matrix have been reported to be dominant factors in stent-related stenosis of the airways (18). Therefore, it seemed possible to hypothesize that erythromycin might inhibit or prevent tissue hyperplasia after stent placement.
We found that erythromycin significantly decreased the degree of inflammation of the stented esophagus (P = 0.025), and higher dosage of erythromycin significantly decreased the degree of inflammation than lower dosage of erythromycin (P = 0.037). There were also a tendency for less tissue hyperplasia in the experimental groups than in the control group and a tendency for less tissue hyperplasia in the higher dosage of erythromycin than in lower dosage of erythromycin. These effects of erythromycin on stent-related tissue hyperplasia might be an antibiotic effect, or they might not. However, considering previous study results (2, 5, 6, 13, 18), we could guess that this is accounted for if erythromycin influences the early inflammatory phase but has minor effect on TGF-ß and the later proliferative phase. However, we did not evaluate concretely the action and effectiveness of each step of formation of stent-related tissue hyperplasia and perform quantitative assays using the methods of molecular biology. Therefore, further study will be needed for the confirmation.
With regard to a possible explanation for its failure to reduce granulation tissue formation, it is possible that insufficient dosage of erythromycin was responsible, and the optimum doses for the anti-fibrogenic and anti-inflammatory effects of erythromycin are not known. However, since the dosage of intravenous erythromycin is generally 5–8 mg/kg/day (19, 20), we used 4 mg/kg and 8 mg/kg for the intraperitoneal injections. With administration of usual dose of erythromycin, erythromycin is generally known to have an anti-inflammatory action independent of its antibacterial effect in the fields of respiratory medicine and otolaryngology (21–25). Therefore it is possible that the levels of erythromycin used in our study may have been sufficient for its anti-inflammatory effect, but not for its anti-fibrogenic effect. Since we introduced erythromycin intraperitoneally, we could not estimate its local concentration in the stented esophagus. Also we could not evaluate its effect on TGF-ß, a factor needed for the production of granulation tissue and fibrosis. Thus, further studies with various doses of erythromycin and various administration routes, as well as quantitative assays using the methods of molecular biology, should be undertaken.
In our study, the total period of erythromycin treatment and observation was 5 weeks. It is possible that the short period of treatment was responsible for our failure to observe suppression of the tissue hyperplasia secondary to stent placement by erythromycin. In previous experimental studies of therapeutic effectiveness using nonvascular stent models, the length of the studies varied between 4 and 8 weeks (8, 9), while in clinical studies treatment lasted from 5 weeks to 3 months and follow-up was extended to a maximum of 6 months in order to observe delayed effects (26, 27). The length of treatment in our study was consistent with the 4 to 8 weeks of the previous studies (8, 9, 26, 27), and should have been adequate to test the effectiveness of the drug so that if we were to extend the observation period beyond 5 weeks, we would be able to observe any delayed effects or delayed responses.
In the current state of knowledge it is not possible to be confident that erythromycin plays a role in inhibiting stent-related tissue hyperplasia. Nevertheless, the anti-inflammatory effect of erythromycin observed here should not be neglected. Understanding the influence of erythromycin on the inflammatory processes that take place in the stented esophageal wall should be valuable for understanding the phenomenon of tissue hyperplasia. Although further studies are necessary, erythromycin could be used in clinical practice as a complement to other drugs with definite anti-proliferative effects rather than as a substitute for them in the treatment of tissue hyperplasia secondary to stent placement.
We used a previously developed rat esophageal model (28). This has several advantages over other animal models, including: (i) cost-effectiveness; (ii) less extensive migration; and (iii) more granulation tissue formation. Granulation tissue secondary to stent placement in the rat esophagus has been reported to be approximately 30% (28), which seems to be adequate for experimental purposes such as evaluation of therapeutic interventions. Moreover, the rat esophageal model has advantages over larger animals. The rat model is a high through-put model because of its easy manipulation and relatively low cost. Also appropriate antibodies and transgenic and knockout strains are available in rats.
This study has several limitations. First, the number of rats used was rather small. Second, because it was difficult to count all inflammatory cells, the degree of submucosal inflammatory cell infiltration was determined subjectively from the distribution and density of inflammatory cells. Third, esophagograms were obtained in all rats before sacrifice 5 weeks after stent placement to verify patency. However, when gross specimens were obtained immediately after the esophagograms, food material was frequently observed within the stented esophagus, and this food material could be interpreted as filling defects on esophagograms thus mimicking stenosis. Therefore we could not evaluate the esophagographic results and the correlation between the degree of stenosis on esophagograms and specimen pathology.
In summary, we have shown that erythromycin was very effective in reducing inflammation after bare metallic stent placement in a rat esophageal model but had limited efficacy in preventing granulation tissue formation.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A091263).