
Abstract
Background
Nutcracker syndrome, also called left renal vein entrapment syndrome, is a cause of non-glomerular hematuria with difficulties in diagnosis. Multidetector computed tomography (MDCT) is a powerful tool to prevent unnecessary diagnostic procedures.
Purpose
To retrospectively determine the prevalence of nutcracker phenomenon and nutcracker syndrome seen in MDCT in consecutive patients.
Material and Methods
The institutional review board approved the study and waived the requirement for informed consent. Abdominal contrast-enhanced MDCT scans were reviewed from 1000 consecutive patients. MDCT scan assessment included renal vein diameter measurements and evaluation for the presence of anterior or posterior left renal vein entrapment. Electronic medical records and urine analysis reports of patients with left renal vein entrapment were reviewed. Student's t test was used to assess differences in renal vein diameter in patients with left renal vein entrapment.
Results
Left renal vein entrapment was observed in 10.9% (109), retro-aortic left renal vein in 6.5% (65), entrapment of left renal vein between superior mesenteric artery and aorta in 4.1% (41), and circumaortic left renal vein in 0.3% (3) of patients. Mean diameters of right (8.8±1.9 mm) and unentrapped left (8.9±1.8 mm) renal veins were not significantly different (P = 0.1). The mean diameter of anterior entrapped left renal veins (10.3±2 mm) was significantly greater (P = 0.04) than contralateral renal veins (8.6±2.1 mm) in their widest portion. In 8.8% of patients with the left renal vein entrapment, urine analysis showed isomorphic hematuria or proteinuria with no other known cause. Varicocele and pelvic congestion were seen in 5.5% of patients with the left renal vein entrapment.
Conclusion
Left renal vein entrapment is not a rare entity and renal nutcracker phenomenon might be underdiagnosed.
Left renal vein entrapment, also known as the nutcracker phenomenon (NCP), is defined by compression of the left renal vein between the aorta and the superior mesenteric artery (1) (anterior nutcracker phenomenon) or between the aorta and the lumbar spine (posterior nutcracker phenomenon). In anterior NCP, the superior mesenteric artery originates at an acute angle from the abdominal aorta and compresses the left renal vein. In posterior NCP, the left renal vein passes posterior to the abdominal aorta and is compressed between the aorta and the lumbar vertebrae. Resultant compression of the left renal vein leads to increased venous pressure.
A radiologic finding of left renal vein compression alone may not be significant unless it is correlated with clinical symptoms (2). The nutcracker syndrome (NCS) occurs in patients with NCP who have clinical symptoms such as isomorphic hematuria, postural proteinuria, left flank pain, left varicocele, pelvic congestion, or hypertension (3, 4). Previous studies have shown that postural proteinuria and intermittent hematuria is associated with left renal vein entrapment (5–7). Postural or orthostatic proteinuria is a condition in which protein appears in the urine in otherwise healthy people who have been in an upright position for a long time. Spontaneous remission of left renal vein entrapment has been reported (8).
The nutcracker syndrome can be diagnosed with a combination of imaging and clinical findings (3, 9). CT and MRI are the most accurate methods in the diagnosis of left renal vein entrapment. Other tests include sonography, color Doppler sonography, intravenous urography, uretero-renoscopy, urine analysis, and left renal vein phlebography and manometry. The exact prevalence of NCP is unknown, and no large series has examined the frequency of NCP. The aim of this study was to investigate the prevalence of NCP detected by abdominal multidetector computed tomography (MDCT) and to determine the prevalence of NCS.
Material and Methods
Patient population
Our institutional review board approved the study and waived the requirement for informed patient consent. We retrospectively identified all patients who underwent abdominal MDCT over a 7-month period at our institution. Our study included 1151 consecutive patients who were referred for abdominal MDCT imaging and who were suspected of having an extrarenal disease, from February 1, 2011 to August 30, 2011.
We excluded patients with malformations or renal vasculature and diseases affecting renal vein diameter. Patients with a single kidney (n = 29), inferior vena cava duplication (n = 7), left-sided inferior vena cava (n = 5), doubled renal vein (n = 41), ectopic kidney (n = 1), horseshoe kidney (n = 3), conglomerate retroperitoneal para-aortic lymph node masses (n = 12), retroperitoneal fibrosis (n = 3), mass lesion (n = 4) or ileus (n = 1) compressing renal vein, renal cell carcinoma invading renal vein (n = 7), renal vein thrombosis (n = 3), severe polycystic kidney disease (n = 3), atrophic kidney (n = 28), and artifacts due to motion or metallic materials (n = 4) were excluded. After these exclusions, abdominal MDCT examinations were reviewed for 1000 patients (mean age, 52.3 years; range, 2–98 years): 537 male patients (mean age, 51.7 years; range, 2–93 years) and 463 female patients (mean age, 53 years; range, 3–98 years) who fulfilled the inclusion criteria. Routine abdominal MDCT images were retrospectively evaluated for the presence of left renal vein entrapment using a picture archiving and communication system in our institution. Electronic medical records of patients with left renal vein entrapment were reviewed.
CT imaging
All 1000 MDCT examinations were performed using a 64-detector row scanner (Aquilion; Toshiba, Tokyo, Japan) with the following parameters: 120 kV, 130 mAs, 0.4 s per rotation, 0.5-mm section thickness, and 0.828 beam pitch. All patients underwent craniocaudal scanning in the supine position during a single held breath. A 1 mL/kg dose of non-ionic contrast medium with an iodine concentration of 300 mg I/mL (iopamidol, Iopamiro 300, Bracco, Milan, Italy; or iobitridol, Xenetix 300, Guerbet, Brussels, Belgium) was administered intravenously followed by a flush of 40 mL saline. Portal venous phase (65-s delay) contrast-enhanced MDCT images were chosen for the study.
Evaluation of MDCT characteristics and clinical symptoms
All CT studies were assessed by two abdominal radiologists in consensus, both of whom had more than 7 years of experience in the field of abdominal imaging. Readers were blinded to clinical information, CT reports, and urine analysis results. MDCT examinations were reviewed in reverse chronological order, so that if a patient underwent more than one CT examination, the later examination was reviewed. Evaluation of renal veins were performed using a DICOM viewer (OsiriX 4.0) on transverse sections.
The radiologists evaluated the presence or absence of left renal vein entrapment and measured the right and left renal vein diameters. For measurement of renal vein diameters, cursors were placed in the vessel wall at the widest portion and perpendicular to the longitudinal axis of the vessel. On portal phase MDCT images, left renal veins with an anterior–posterior diameter of the aortomesenteric portion smaller than 50% of that of the hilar portion was defined as anterior NCP (3). Patients with retro-aortic course of left renal vein were defined as having posterior NCP (2).
In patients with NCP, complete records were then reviewed to determine if proteinuria and isomorphic hematuria were previously identified by urine analysis. The time interval between CT examinations and urine analysis ranged from 1 to 92 days (average 26 days).
We examined erythrocyte and total protein measurements on urine analysis reports. Positive urine analysis in a patient was defined as at least three urine analysis reports describing proteinuria and/or isomorphic hematuria. Patient age, sex, and medical history were also reviewed.
Statistical analysis
Student's t test was performed to assess differences in the mean diameters of renal veins. The prevalence of NCP by sex was examined using univariate logistic regression analysis. Pearson's correlation coefficient r was calculated for the association between diameter of left renal veins and presence of positive urine analysis, varicocele and pelvic congestion. All values are expressed as mean ± standard deviation, and a P value of 0.05 was considered significantly different. Statistical analyses were performed using GraphPad Prism 5 for Mac (GraphPad Software, San Diego, CA, USA).
Results
The prevalence of left renal vein entrapment was 10.9% (109 of 1000 patients; 59 men and 50 women) in our study. Anterior NCP (Fig. 1) was identified in 4.1% (41 patients; 24 men and 17 women), posterior NCP (Fig. 2) was identified in 6.5% (65 patients; 33 men and 32 women) and circum-aortic left renal vein was identified in 0.3% (3 patients; 2 men and 1 woman) of patients. There was no difference by sex in the prevalence of NCP (P = 0.44).
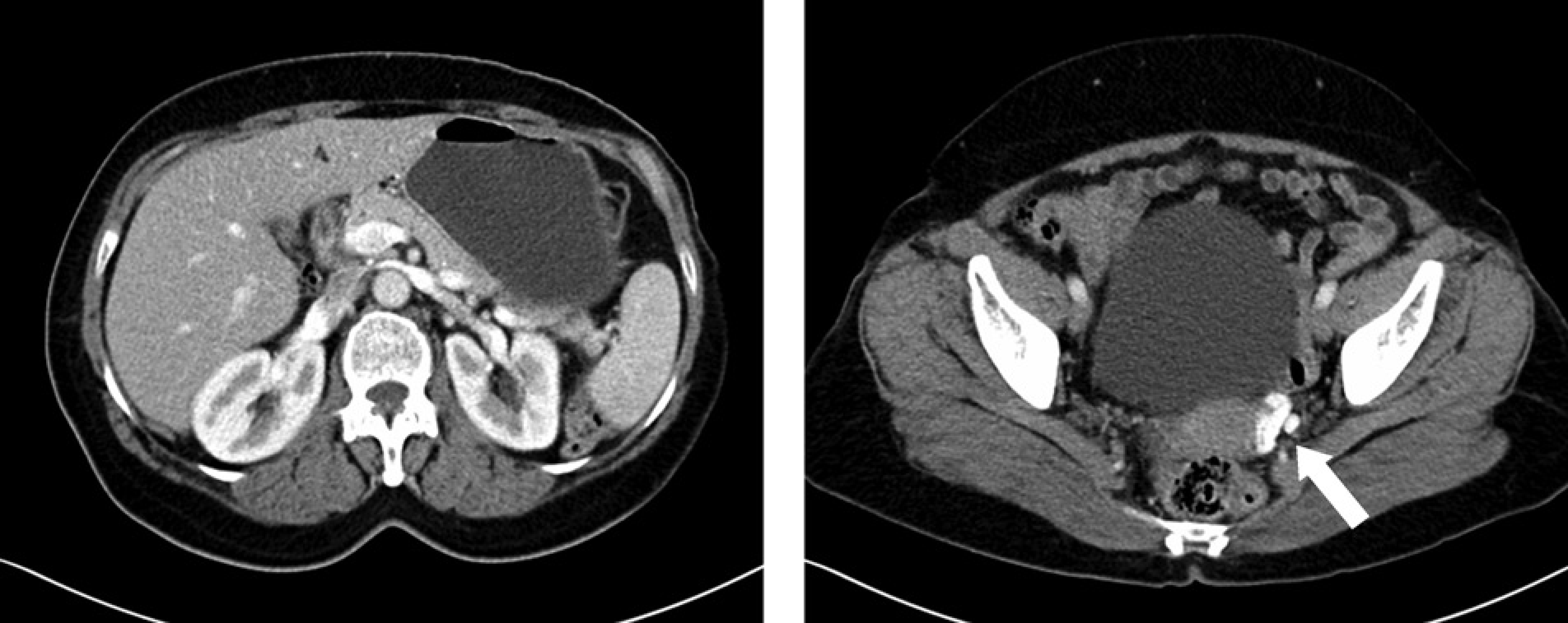
(a) A 59-year-old female patient with anterior left renal vein entrapment. Transverse portal phase contrast-enhanced MDCT images of upper abdomen demonstrates left renal vein entrapment between aorta and superior mesenteric artery; (b) Varicose dilatation of left ovarian vein (white arrow) and reflux of contrast medium from renal vein is seen

Patients with posterior left renal vein entrapment. Transverse portal phase contrast-enhanced MDCT images of upper abdomen demonstrates retro-aortic course of left renal vein. (a) A 35-year-old female patient with mixed proteinuria, hematuria, and left flank pain; (b) a clinically asymptomatic 50-year-old female patient
Among all patients, the diameter of the normal right and left renal veins was examined to determine variation by age (Table 1). Vessel diameters increased to maximal values for patients between the ages of 20 and 40 years, and then decreased again in older patients.
Normal renal vein diameters

*Values are given as mean ± standard deviation
LRV, left renal vein; RRV, right renal vein
Mean diameter of 1000 right renal veins was 8.8 × 1.9 mm and that of 891 normal left renal veins, 8.9 × 1.8 mm. The difference was not significant (P = 0.1).
Mean diameters of 65 entrapped posterior and 41 entrapped anterior left renal veins were 8.9 ± 1.8 mm, and 10.3 ± 2 mm, respectively. This difference was not significant (P = 0.43). However, the mean diameter of entrapped anterior left renal veins was significantly larger than that of contralateral right renal veins (P = 0.04).
Electronic medical records of symptomatic patients showed that seven patients had a known cause of hematuria and/or proteinuria: chronic kidney failure (n = 1), acute kidney failure (n = 1), systemic sclerosis (n = 2), Cushing syndrome (n = 1), abdominal trauma (n = 1), and chemotherapy (n = 1). After exclusion of these patients, five patients with posterior NCP and four patients with anterior NCP showed persistent and/or intermittent isomorphic hematuria and/or proteinuria in urine analysis (Table 2). Nine of 102 patients (8.8%) among whole population with NCP showed hematuria or proteinuria in urine analysis.
Presence of isomorphic hematuria and proteinuria in patients with NCP
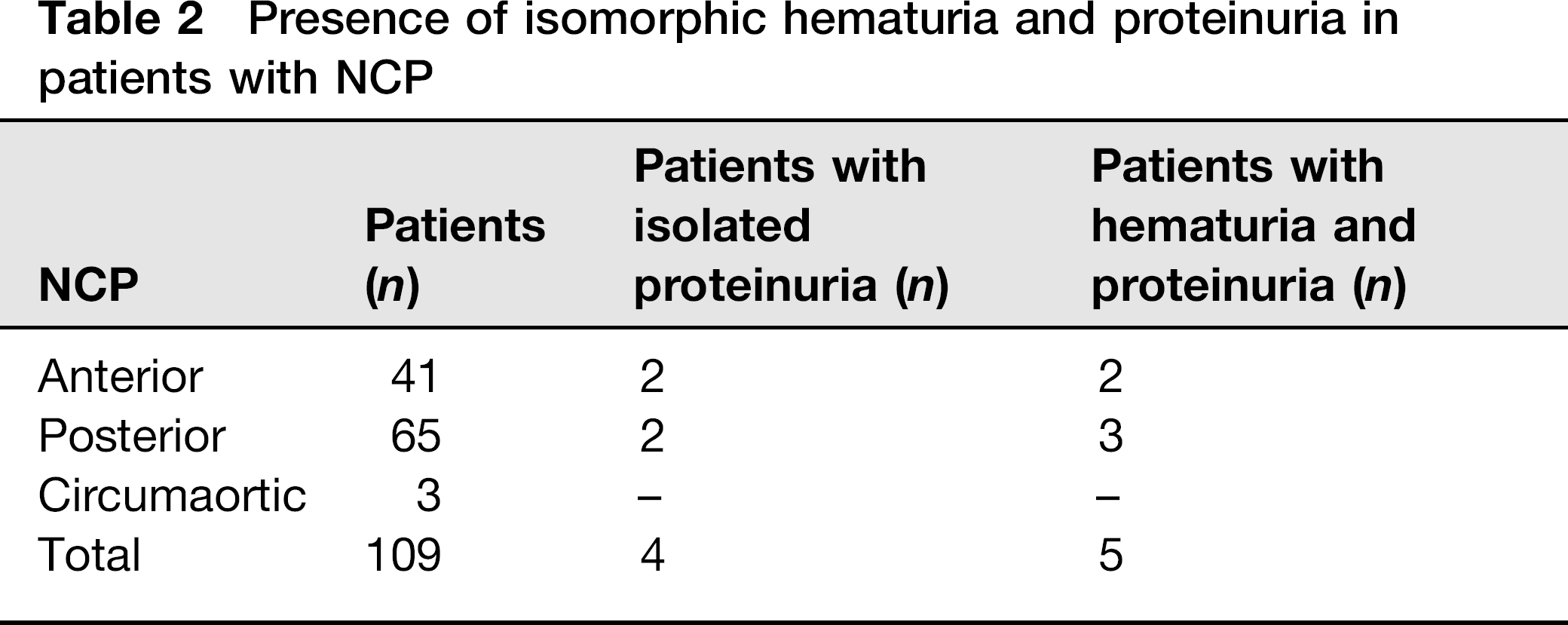
Mixed proteinuria and hematuria was the most frequent finding (n = 5), followed by isolated proteinuria (n = 4) in patients without any other known cause. Varicocele was seen in four patients and pelvic congestion was seen in two patients with anterior left renal vein entrapment. The correlation between left renal vein diameters and presence of positive urine analysis, varicocele and pelvic congestion was weak (r = 0.32).
Discussion
NCP refers to left renal vein entrapment between the abdominal aorta and the superior mesenteric artery or the vertebrae. The terms NCP and NCS, however, are not synonymous. NCP with associated clinical symptoms due to renal vein obstruction is referred to as NCS. The exact prevalence is unknown. Limited data are available on the prevalence or incidence of left renal vein entrapment in the general population, and it is thought to be underdiagnosed because of non-specific urine analysis findings and complaints (10–13).
In our study, MDCT detected NCP in 10.9% of the patients, and there was no difference in prevalence based on sex. The prevalence of anterior and posterior left renal vein entrapment was 4.1% and 6.5%, respectively. Reed et al. (14) reviewed abdominal CTs of 433 patients for the presence of retro-aortic and circumaortic left renal vein and found a prevalence of 6.2%, consistent with our results.
We found no significant difference in the mean diameters of normal left renal vein and normal right renal veins, consistent with observations of Satyapal et al. (15). Normal vein diameters increased with increasing age, with the largest diameter in individuals 20–40 years of age, then decreasing progressively. Decreased renal vein diameter in elderly compared to the young subjects might be related to decreased elasticity and reduced compliance of vessels. In patients with anterior NCP, the left renal vein was significantly wider than the contralateral right renal vein; in patients with posterior NCP, the difference was not significant.
Unrecognized NCS may result in anemia, hypertension, and repeated urine analysis and imaging studies to investigate the cause of hematuria and proteinuria. The pathophysiology of NCS is not fully understood. Some patients with NCP are asymptomatic; 86.3% of patients with NCP were asymptomatic in our study. Symptoms are often related to a patient's body position, and aggravated during upright standing and relieved by recumbency. The severity of clinical symptoms varies, and many findings are non-specific, thereby overlapping with other clinical entities (1). Common symptoms are orthostatic proteinuria, hematuria, varicocele, gonadal vein syndrome, and left flank pain (16–21).
Orthostatic proteinuria and hematuria might be related to increased inferior vena cava pressure due to gravity when an individual is in the upright position, which worsens pressure elevation in left renal vein. Persistent asymptomatic isomorphic microscopic hematuria with unknown etiology is a cause to suspect NCS, given that hematuria is the most commonly reported symptom associated with NCS. Hematuria is attributed to the rupture of thin-walled varices into the left collecting system due to increased venous pressure (22, 23). The dysmorphic red blood cells are the marker for glomerular bleeding and the isomorphic red blood cells for non-glomerular bleeding in urine. We looked for isomorphic hematuria to exclude glomerulo-pathy related hematuria. Orthostatic proteinuria is another symptom of NCS that is commonly reported (5, 20, 21). The cause of proteinuria in NCS is not clear, but is thought to be related to elevated venous pressure, perhaps induced by the enhanced action of angiotensin II (24, 25). Previous studies showed that left renal vein entrapment is an important cause of proteinuria (6, 26).
Pain and hypertension are other symptoms associated with NCP. Left flank pain radiating to the left lower quadrant due to pelvic venous congestion or left ureteral colic, from the passing of blood clots down the left ureter, have been described. In this study, we did not investigate pain symptoms in patients with NCP because pain is a subjective symptom, and it is difficult to identify its origin definitively. Five patients with hypertension also had hematuria and/or proteinuria in urine analysis in our study. Notably, spontaneous resolution of NCP has been described in children, sometimes after several years of persistence (27).
MDCT is a fast and reliable method that enables detection of a compressed left renal vein and may prevent an unnecessary biopsy. Portal venous phase MDCT scanning is adequate for the diagnosis of left renal vein entrapment. Multiphase MRI of the upper abdomen is another reliable imaging technique for the evaluation of renal veins. Other techniques include sonography, color Doppler sonography, and angiography, although these modalities have some limitations. The presence of an entrapped left renal vein on imaging requires subsequent urine analysis and evaluation of clinical findings such as hematuria, proteinuria, left flank pain, varicocele, pelvic congestion, and hypertension.
Our study has some limitations. First, we may have underestimated the prevalence of NCS due to our inability to assess pain symptoms arising from left renal vein compression. It is difficult to accurately determine the cause of pain, because the symptoms overlap with those of other diseases causing left abdominal pain. A second limitation is the lack of biopsy results to confirm the absence of co-existing diseases that may cause hematuria and/or proteinuria in the presence of NCP. Seven patients with NCP had comor-bidities that could lead to hematuria and/or proteinuria. We were unable to determine the exact cause of these symptoms; we assumed that co-existing diseases are the cause of dysmorphic hematuria or proteinuria in these cases.
In conclusion, the current study shows that renal nut-craker may be an underdiagnosed phenomenon. Attention should be paid for evaluation of left renal vein anatomy in patients with symptoms like proteinuria and/or isomorphic hematuria, left flank pain, and varicocele.