
Abstract
Background
Suboptimal stent-graft placement at the lower anastomosis during transjugular intrahepatic portosystemic shunt (TIPS) may result in early shunt stenosis and occlusion owing to incomplete covering of the parenchymal tract by the covered part of the stent-graft.
Purpose
To determine the optimal portal venous projection view for stent-graft placement during TIPS and the potential influence of the portal vein anatomy.
Material and Methods
On 76 cirrhotic patients (48 men and 28 women) selected for TIPS, rotational, three-dimensional (3D), catheter-directed angiography of the portal vein was performed. The 3D portograms were reviewed by two independent interventional radiologists to determine the optimal angiographic projection views for stent-graft placement. Intra-observer and inter-observer reliabilities were tested and subgroups of patient portal vein anatomy were categorized.
Results
Among all patients, the optimal portal venous projection views for stent-graft placement during TIPS centered around 27° (±14°) right oblique and 3° (±7°) craniocaudal. Of these, 56% were within the standard deviations. Intra-observer reliabilities were 0.60 and 0.62 for the two radiologists, respectively. Inter-observer reliability was 0.48. Anatomical variations in the patient population were: normal portal vein (67%), trifurcation at main portal vein (16%), right posterior portal vein as the first branch of main portal vein (3%), no right posterior portal vein (1%), and other variations (13%). Anatomical subgroups did not influence the best angiographic projection view significantly (F4,295 = 0.91, P = 0.457).
Conclusion
The mean optimal angiographic projection view for TIPS stent-graft placement was 27° right oblique and 3° craniocaudal. Patient anatomic variations do not play a significant role in determining the optimal angiographic view for TIPS stent-graft placement.
Transjugular intrahepatic portosystemic shunt (TIPS) is utilized in selected patients with severe symptoms of portal hypertension like upper variceal bleeding and refractory ascites (1–3). To keep the shunt open, a vascular stent should be inserted; however, expanded-polytetrafluoroethylene (e-PTFE) covered stents provide better long-term patency than bare stents (4–6). Typically this stent-graft (Viatorr, WL Gore and Associates, Flagstaff, AZ, USA) is placed over the tract so that the proximal 2 cm bare metal part of the stent is placed in the (right) portal vein and the e-PTFE fabric is completely covering the parenchymal tract avoiding any direct contact in between liver parenchyma and the blood flow. The distal part of the stent-graft should land at the hepatic vein inflow into the inferior vena cava. Suboptimal stent-graft placement with incomplete covering of the parenchymal tract by the e-PTFE fabric can result in early shunt stenosis and occlusion and potentially in recurrent symptoms of portal hypertension (7).
Therefore, the portal vein (PV) entry site of the stent-graft should be in the right branch of the PV approximately 1–2 cm (3) or 2–3 cm (4, 5) from the bifurcation to remain intrahepatic. The distal part of the stent-graft should extend to the right hepatic vein–inferior vena cava junction (8, 9) and the proximal extent should be within the right PV or the main branch of the portal vein (10). It is clear that optimal view of the portal venous system is needed by a portogram at this stage to allow accurate estimation of the length of the stent graft and correct positioning of the covered part of the TIPS stent-graft.
Conventional portography provides two-dimensional (2D) venograms of the PV that assist planning and placement of the stent-graft. However, given the complexity of the portal anatomy and its variants (11–14), 2D portograms from an anteroposterior projection view might be suboptimal for accurate stent-graft placement due to insufficient information on the spatial relationship of the veins.
By using the three-dimensional rotational angiography (3DRA) technique, a 3D representation of the portal anatomy can be reconstructed based on a large number of 2D venograms projection views. This allows viewing the PV from any 2D projection view by rotating the volume rendered image. Potentially, the added spatial information in the 3D portogram could lead to more accurate stent-graft placement.
In the literature, best practice of the portal vein projection view for TIPS with regard to optimal placement of the stent-graft at the site of the portal vein has not been described, neither is the usefulness of 3D portography in such a procedure. The purpose of the present study was to assess the optimal portal vein projection view for TIPS stent-graft placement and to determine if variation in patient portal vein anatomy may influence the best angiographic projection view.
Material and Methods
Patient selection
Patient demographics
Angiographic technique – 3D portography
The technique of the TIPS-procedure is extensively described elsewhere (9). Briefly, under general anesthesia, the right hepatic vein is catheterized via right jugular access. After wedged CO2-portography the proximal right PV is targeted using a coaxial puncture set (Rösch-Ushida, Cook Medical, Bjaeverskov, Denmark).
An abdominal 3DRA was performed after the puncture and catheterization of the PV through a calibrated 5 French (F) pigtail catheter (Cook Medical, Bjaeverskov, Denmark) to obtain a 3D portography (Fig. 1). All the rotational scans were performed by using a flat-panel angiography system (Allura Xper FD20, Philips Healthcare, Best, The Netherlands). The rotational angiographic images were acquired by rotating the X-ray source and image detector C-arm around the patient from right oblique (RAO) 90° to left oblique (LAO) 90°; 120 images were acquired at an image detector field of view of 48 cm and at a speed of 15 images/s. A volume of 30 mL contrast material was injected in the PV at a rate of 3 mL/s. Image acquisition started 2 s after contrast material injection. The acquisition time of images was 8 s. Volume-rendered 3D images were reconstructed (Xtravision, Philips Healthcare, Best, The Netherlands), after the image acquisition to a matrix of 2563 pixels.
3D portography images of a female patient at (a) anterior-posterior view, and at (b) right anterior oblique 24° craniocaudal 4°. The entry point into the proximal right portal vein may be located (a) in between both arrows which is a distance of more than 1 cm; in the oblique view (b) the entry point is more likely to be at the level of the arrow, just in front of the bifurcation to the posterior and anterior branch of the right portal vein (c) corresponding oblique 2D-angiographic view used for inserting the stent-graft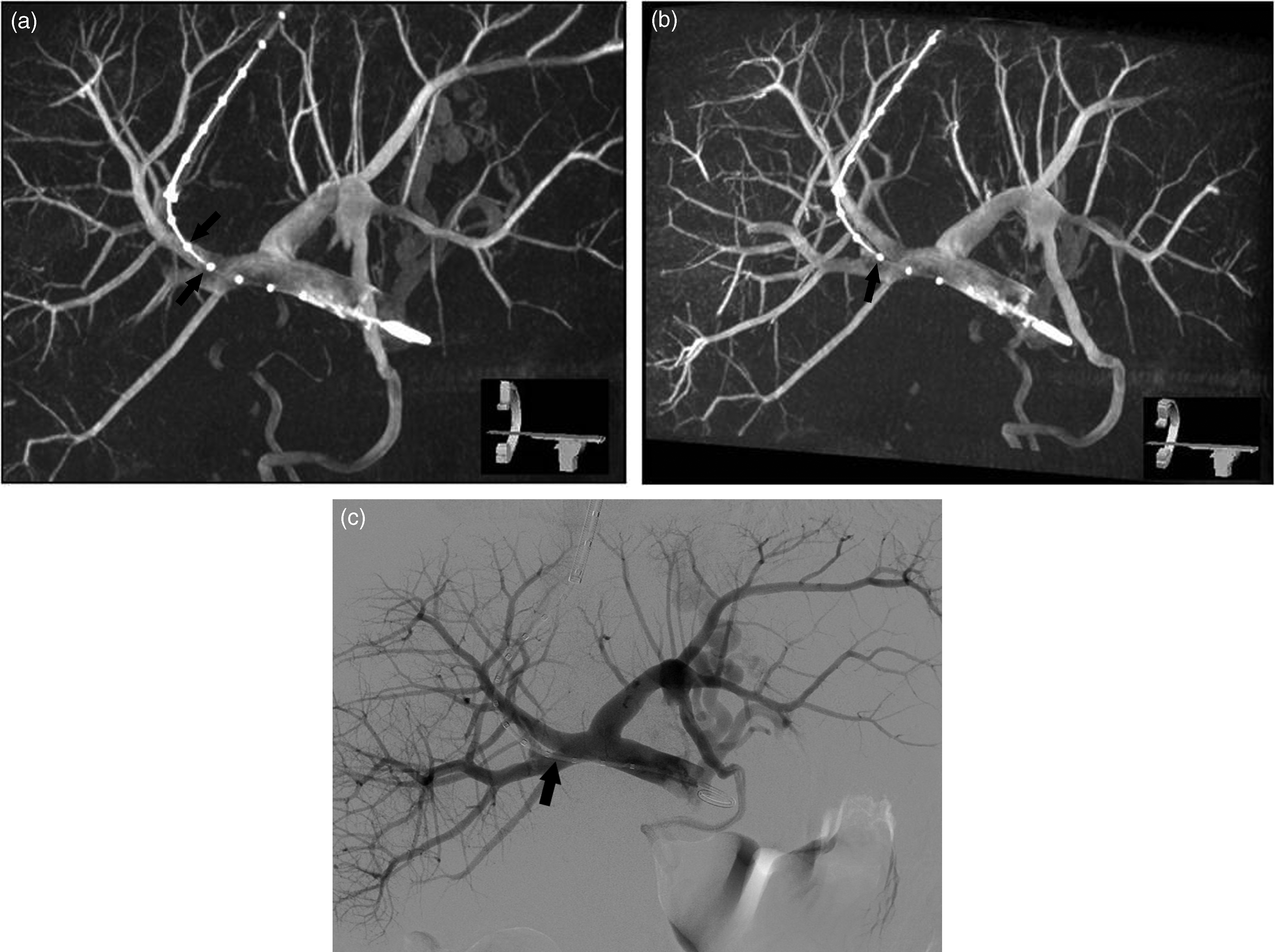
Finally, after parenchymal tract predilatation (5 mm diameter angioplasty balloon) an e-PTFE-covered stent-graft (Viatorr, WL Gore and Associates, Flagstaff, AZ, USA) is inserted. The stent-graft is post dilated up to 8 mm or 10 mm in case of refractory ascites or variceal bleeding, respectively.
Study design
Two interventional radiologists with 20 years (GM) and 13 years (SH) of experience, respectively, reviewed the 3D portograms twice independently. Each radiologist blindly reviewed the same set of 76 patient 3D portograms twice, i.e. no reference to the review results from the first round when reading the same image at the second time. For every 3D portogram, each radiologist chose the optimal angiographic projection view for the TIPS stent-graft placement. The optimal projection view was defined such that it should provide the best working view of the portal structure during the stent-graft deployment phase of the TIPS procedure. Each chosen angiographic projection view was indicated by the degree of the X-ray gantry rotation and angulation in relation to the patient, i.e. RAO/LAO 0–90° and craniocaudal (CRAN)/caudalcranial (CAUD) 0–45° (physically achievable by the X-ray gantry during TIPS procedures).
Additionally, patient PV anatomy was reviewed and categorized in subgroups based on Covey classification (10): (i) the classic PV anatomy; (ii) trifurcation at the main PV to left PV, right anterior PV and right posterior PV; (iii) right posterior PV as the first branch of main PV; (iv) non-existing right posterior PV; and (v) other variations.
Statistical analysis
The optimal projection views that were chosen for all 76 patients from the same round of reading were plotted using the rotation and angulation degrees of the X-ray gantry as axes (Fig. 2). The mean optimal angiographic projection view was then calculated as the centroid of the plot using k-mean cluster analysis. Standard deviations of the reading results were calculated on both rotation and angulation axes. The intra-observer and inter-observer reliabilities were calculated by the analysis of variance (ANOVA). When calculating the reliabilities, outliers were excluded based on the following criterion: the difference between the point and centroid is larger than 2× standard deviation.
A plot of the reading results on both right anterior oblique/left anterior oblique and craniocaudal/caudalcranial axes. The mean optimal angiographic projection view, right anterior oblique 27° (±14°) craniocaudal 3° (±7°), is derived as the centroid point of the reading results. Fifty-six percent of the results were within the standard deviation of the results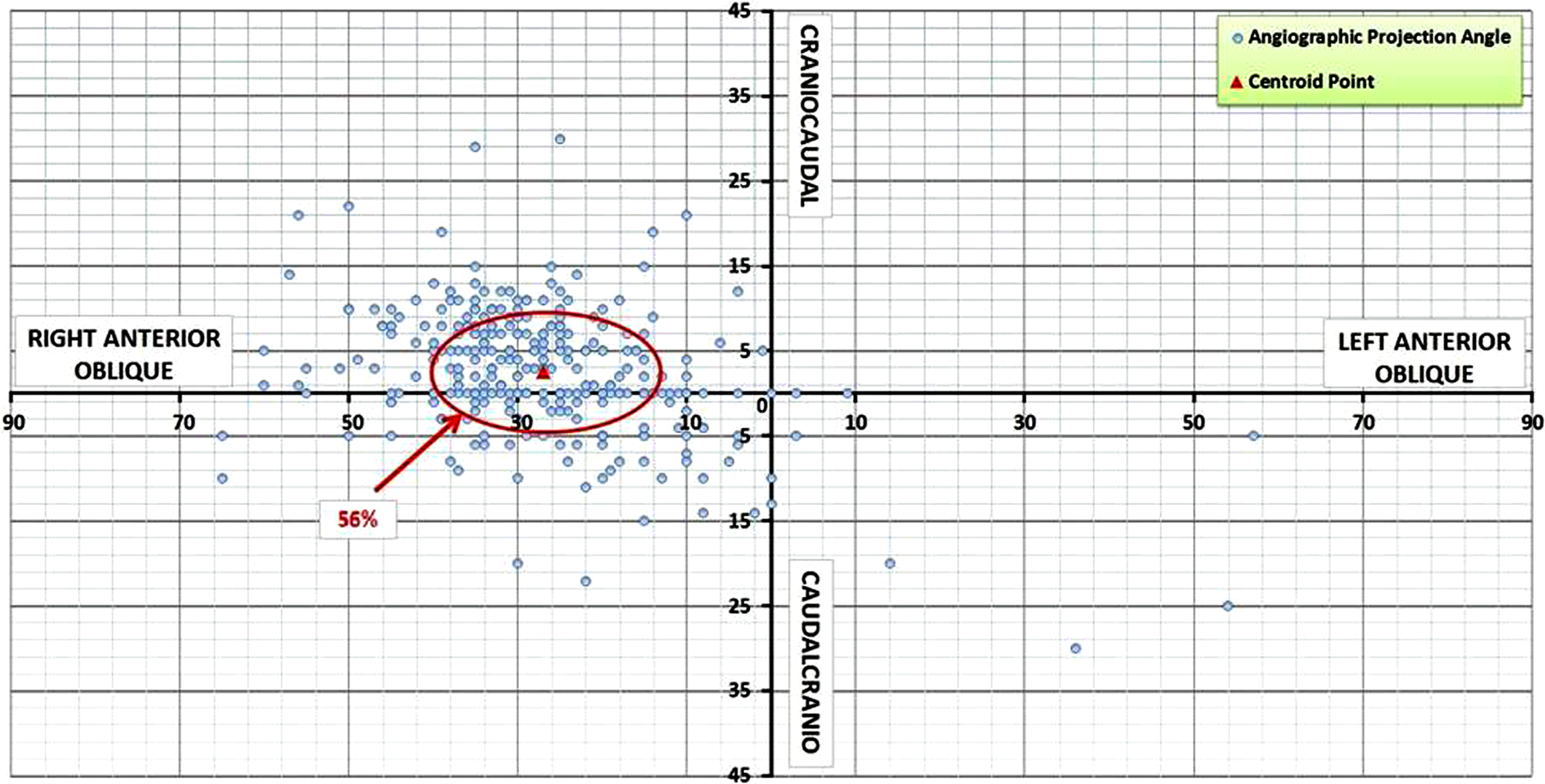
The reading results were divided into five subgroups according to the classification of PV anatomy. The anatomic variation influence in the reading was analyzed by the ANOVA F-test. For a significance level of 0.05 (P value < 0.05), an F value (i.e. F4,295 in the present study) of > 2.40 is considered to indicate statistical difference.
Results
All 3D portograms showed sufficient image quality for the radiologists to determine the optimal angiographic project views for TIPS stent-graft placement. In each of the four groups, the optimal angiographic projection views chosen for all the patients formed a clear centroid, i.e. the mean optimal projection view.
Mean optimal projection views reading results
CAUD, caudial; CRAN, cranial; LAO, left anterior oblique; RAO, right anterior oblique
The two readings from radiologist 1 lead to an intra-observer reliability of 0.60. Eleven outliers were identified in the reading results and excluded from the calculation of the reliability. Radiologist 2 had an intra-observer reliability of 0.62 with 15 excluded outliers in the reading results. The inter-observer reliability between the two radiologists was 0.48.
Patient portal vein anatomy subgroups
MPV, main portal vein; PV, portal vein; RPPV, right posterior portal vein
Discussion
The reading results in the present study show that the optimal angiographic projection with regard to the best view on the portal landing zone of the stent-graft during TIPS creation typically lies in the range of RAO 15° to 40° with slight angulation (CRAN 10° to CAUD 5°).
For the majority of TIPS patients in the study, the optimal projection view was near RAO 27° CRAN 3°. The mean values from all four readings agree with each other. The intra-observer reliabilities (0.60 and 0.62) indicate reasonably consistent reading results were obtained from each radiologist independently. However, the inter-observer reliability was fairly low. This suggests certain degree of subjective preference in recognizing the optimal angiographic projection views for TIPS stent-graft placement: radiologist 1 has a preference of CRAN 6° while radiologist 2 prefers CAUD 1° (Table 2). This is a significant difference (7°) considering the standard deviations in the reading results were from 4° to 7° on the CRAN/CAUD axis.
Despite the clear centering of the chosen optimal angiographic projection views, a spread of projection views was shown. This may reflect the individual difference in the patient PV anatomy and potentially also the variation in entry point of the puncture needle in the PV during TIPS creation. The anatomical variation of the selected patient population showed a majority of normal portal anatomy, a notable minority of main PV trifurcation, rare cases of the right posterior PV as the first branch of the main PV and absent right posterior PV, and several unclassified variants. These findings are in agreement with the literature data (6, 7, 10–14). No statistically significant influence from the anatomical variants in determining the optimal angiographic projection view in TIPS stent-graft placement was found.
Three-dimensional (3D) visualization of the portal venous system can also be made based on multidetector computed tomography (MDCT) (15, 16) imaging, performed prior to the TIPS procedure. The optimal 3D portal venous obliquity for distal stent-graft insertion can then be used during TIPS stent-graft insertion. This technique is in analogy with optimal tube obliquity prediction using angiographic magnetic resonance (angio-MR) imaging prior to uterine fibroid embolization as described by Naguib et al. (17).
There are some limitations of this study. This was not a randomized study comparing the use of 3D rotational portography to conventional 2D portography for optimal stent-graft placement and subsequently potential decrease of early or late instent stenosis or occlusion. Further, this was a monocenter trial using one type of 3D rotational abdominal angiography technology. Finally, no assessment of potential difference in radiation dose between 3D rotational portography and conventional 2D portography was made. This might become a major issue as TIPS procedures are not of free of radiation-induced skin or other injuries (18).
In general, 3D portography was satisfying in determining the optimal angiographic projection view for TIPS stent-graft placement. This angiographic technique could be particularly beneficial for interventional radiologists who have limited experience in conducting TIPS procedure, or when the patient anatomy is complex. In situations where 3D portography is not applicable, we suggest to start at the reported mean optimal angiographic projection angle in searching for the patient individual projection view for TIPS stent-graft placement. Doing so could potentially reduce the amount of 2D venograms and contrast injection.
Finally, based on the collected data it is unclear in how many cases this 3D imaging technology might influence the distal landing zone or total length of the stent-graft.
In conclusion, the mean optimal angiographic projection view for TIPS stent-graft placement in this study was RAO 27° and CRAN 3°. In case of residual superposition of vascular structures in this particular position, a rotational 3D-portogram is a valuable alternative in order to determine the best C-arm position for stent-graft deployment. Our findings in patient anatomic variants agree with the literature, however, the variations do not play a significant role in determining the optimal projection angiographic view for TIPS stent-graft placement.