
Abstract
Background
It has become evident that gadolinium-based contrast agents (GBCA) may have nephrotoxic potential. Oxidative stress is one of the most important pathways in the pathogenesis of iodinated contrast-induced nephropathy.
Purpose
To investigate the effects of static magnetic fields and gadopentetate dimeglumine (Magnevist®) on oxidant/antioxidant status via measurement of total antioxidant capacity (TAC), total oxidant status (TOS), and serum malondialdehide (MDA).
Material and Methods
Two age- and sex-matched groups of patients not under oxidative stress conditions that underwent magnetic resonance imaging (MRI) were recruited to this study. While contrast-enhanced (Magnevist®, 0.2 mmol/kg) MRI was performed in group 1, MRI without GBCA was performed in group 2. Fasting blood glucose, C-reactive protein, serum creatinine, liver enzymes, uric acid, and lipid parameters were examined in all patients. Peripheral venous blood samples in order to determine TAC, TOS, and MDA were collected before and 6, 24, and 72 h after the MRI procedures. The TOS:TAC ratio was used as the oxidative stress index (OSI). Patients were followed up to 72 h.
Results
There were no significant changes in serum TAC, TOS, and MDA levels (Δserum TAC, Δserum TOS, and ΔMDA) in either group 6, 24, or 72 h after the procedures (P > 0.05). Furthermore, OSI did not change after the procedures in either group (P > 0.05).
Conclusion
Magnetic field and gadopentetate dimeglumine (Magnevist®) do not change the oxidant or antioxidant status at a dose of 0.2 mmol/kg.
Imaging procedures with iodinated radiological contrast agents (ICA) remain to be an important cause of acute kidney injury (AKI) in hospitalized patients. The pathogenesis of contrast-induced nephropathy (CIN) is still controversial, and is likely to be multifactorial. Altered renal hemodynamics, changes in renal parenchymal oxygen supply, and direct tubular toxicity are the main potential mechanisms (1). It has been demonstrated in experimental studies that hypoxia and the formation of reactive oxygen species (ROS) within the kidneys following the administration of ICAs may play a role in the development of CIN. The hyperosmolar stress due to the use of ICAs has also been shown to trigger prompt generation of ROS. ROS may induce direct tubular and vascular endothelial injuries and might further intensify renal parenchymal hypoxia (2).
Gadolinium, a rare-earth lanthanides metal, has been utilized as a contrast agent in magnetic resonance imaging (MRI). Gadolinium-based contrast agents (GBCA) have been traditionally used as a non-nephrotoxic alternative to ICAs for digital subtraction angiography (DSA), especially in patients with chronic renal insufficiency. However, its use has been questioned on the basis of reports of nephrotoxi-city (3, 4). A recent study suggests that the in-vivo release of gadolinium ion through transmetallation and its retention in tissues are closely related with the development of nephrogenic systemic fibrosis (5). Nevertheless, the exact pathogenic mechanism underlying nephrotoxicity of gadolinium-based MRI has not been well studied.
Recently, Xia et al. demonstrated that treatment of primary cultured rat cortical neurons with gadolinium resulted in an increase in intracellular ROS level. The authors concluded that gadolinium-induced cytotoxicity in rat cortical neurons occurs via intracellular oxidative injury (6). However, the specific effects of GBCA on in situ circulatory oxidant status or different tissues including heart, kidney, or liver remain to be undefined.
To our knowledge, it has not been known whether the GBCAs have oxidative properties or not, in humans. We aimed in this study to investigate the effects of gadopentetate dimeglumin (GD) on serum malondialdehide (MDA) level, total oxidant status (TOS), total antioxidant capacity (TAC), and oxidative stress index (OSI).
Material and Methods
We designed a prospective case-control study. Two age- and sex-matched groups of patients not under oxidative stress condition that underwent MRI were recruited to the study. Informed consent was obtained from all patients, and the study protocol was approved by the institute's ethical committee on human research.
Patients with neoplastic diseases, acute or chronic inflammatory conditions (i.e. vasculitic syndromes, infectious diseases), chronic obstructive lung disease, decompensated heart failure, and hyperuricemia as well as smokers and patients under antioxidant vitamin or drug treatment were excluded.
Individual demographic data and co-morbidities were recorded for all patients. Systolic and diastolic blood pressure was measured before and after the administration of DG by a standardized automated device (Omron M6 Comfort, Matsusaka, Mie, Japan).
Contrast-enhanced MRI studies (Magnevist® [Berlex Lab., Wayne, NJ, USA], brand of gadopentetate dimeglumine, 0.2 mmol/kg) were performed in group 1 (n = 40), while MRI studies without any contrast material were applied to group 2 (n = 40). Mean age of patients in group 1 were 42.5 ± 8.1 years and 44.1 ± 11.4 years in group 2. Contrast-enhanced MRI was performed for lumbar disc herniation in 33 patients, and evaluation of symptoms after laminectomy or diskectomy for lumbar disc herniation in seven patients. MRI without any contrast agent was performed for the diagnosis of chondral lesions of the knee joints in all patients in group 2.
Fasting blood glucose, C-reactive protein, serum creati-nine, liver enzymes, uric acid, and lipid parameters were studied in all patients. Peripheral venous blood samples for determining TAC, TOS, OSI, and MDA were collected before, 24, and 72 h after the MRI procedures. Patients were followed up to 72 h. Fixed dose of GD (0.2 mmol/kg) was administered to all patients in group 1.
Time schedules and specimens for laboratory measurements which were performed during the study are shown in Table 1. Serum creatinine, albumin, uric acid, serum electrolytes, total cholesterol, low-density lipoprotein, and triglyceride levels, liver enzymes, fasting blood glucose, hemoglobin A1c, and C-reactive protein levels were studied with (Roche Cobas Integra 800 Chemistry Analyzer, Basel, Switzerland). Albumin/creatinine values were measured in morning spot urine with (Roche Cobas Integra 800 Chemistry Analyzer, Basel, Switzerland).
Test and procedures applied to patients
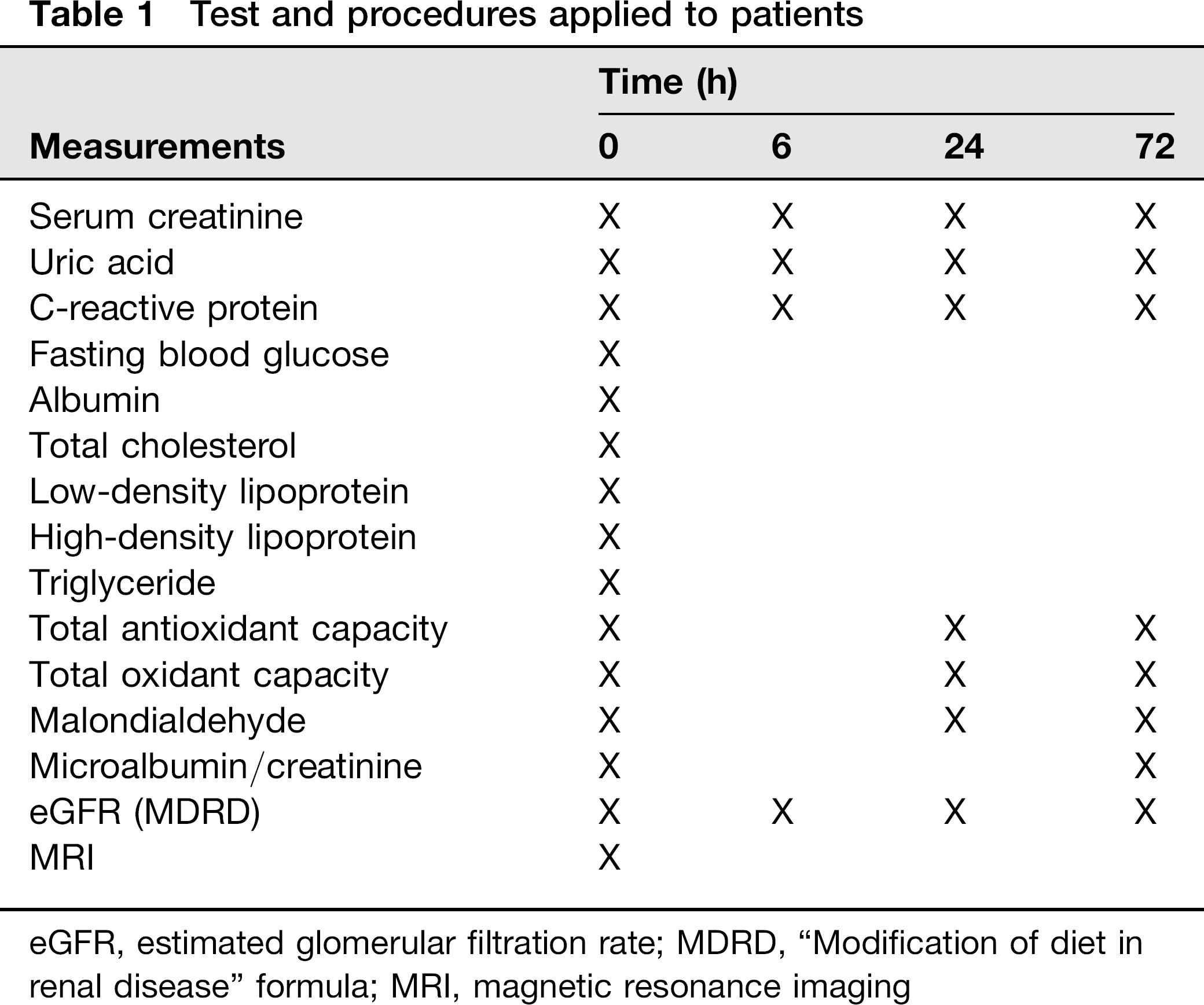
eGFR, estimated glomerular filtration rate; MDRD, “Modification of diet in renal disease” formula; MRI, magnetic resonance imaging
Serum samples were centrifuged and stored at −80°C until analysis. Serum levels of MDA were measured with high-pressure liquid chromatography by using a MDA kit (Chromosystems, Munich, Germany).
Measurement of the TAC
TAC of serum was determined with a novel automated measurement method developed by Erel (7) (Real Assay Total Antioxidant kit) (catalog no: RL0017). By this method, hydroxyl radical, the most potent reactive oxygen species (8), is produced. In the assay, ferrous ion solution, which was present in Reagent 1, was mixed with hydrogen peroxide, which was present in Reagent 2. The sequential process produced radicals, such as brown-colored dianisidinyl radical cation, produced by the hydroxyl radical. Using this method, the antioxidative effect of the sample against the potent-free radical reactions, which was initiated by the produced hydroxyl radical, was measured. The assay had excellent precision values lower than 3%. The results were expressed as mmol Trolox Equiv./L.
Measurement of TOS
TOS of serum was determined with a novel automated measurement method developed by Erel (9) (Real Assay Total Oxidant kit) (catalog no: RL0024). Oxidants present in the sample oxidized the ferrous ion-o-dianisidine complex to ferric ion. The oxidation reaction was enhanced by glycerol molecules, which were abundantly present in the reaction medium. The ferric ion makes a colored complex with xylenol orange in an acidic medium. The color intensity, which can be measured spectrophotometrically, is related with the total amount of oxidant molecules present in the sample. The assay was calibrated with hydrogen peroxide, and the results were expressed in terms of micromolar hydrogen peroxide equivalent per liter (mmol H2O2 Equiv./L).
Oxidative stress index (OSI)
The ratio (%) of the total peroxide to the total antioxidant potential gave the OSI which is an indicator of the degree of oxidative stress.
MRI imaging
MRI scans of lumbosacral region (group 1) were obtained with a GE Signa 1.5-T unit (Signa HDe 1.5 T, GE Healthcare, Milwaukee, WI, USA) using a spine array coil. The following spin-echo sequences were used: Axial localizer (spoiled gradient), sagittal T1 (TE minimum full/TR, 400), sagittal T2 (TE, 100; TR, 4000), sagittal proton density (TE, 10-20; TR, 2000), axial T1 (TE minimum full/TR, 400) (thickness, 4 mm; spacing, 0.4 mm, matrix, 512 × 512, FOV, 26 cm). GD was preferred as the contrast material for MRI and was administered to group 1 patients at a dose of 0.2 mmol/kg.
MRI of the knees (group 2) was performed with 1.5-T MR scanner (Signa HDe 1.5 T, GE Healthcare, Milwaukee, WI, USA) 1.5 Intera, Philips, Best, The Netherlands). The MR examination took about 15 - 20 min per patient. Pulse sequences comprised: sagittal proton-density-weighted sequence (TR, 2618 ms; TE, 15 ms; slice thickness, 4 mm; slice gap, 0.30; matrix, 256 × 256); sagittal T2-weighted turbo spin-echo (TR, 2618 ms; TE, 100 ms; slice thickness, 4 mm; slice gap, 0.30; matrix, 256 × 256); coronal short Tau inversion recovery (STIR) (TR, 1689 ms; TE, 15 ms; TI, 160 ms; slice thickness, 3 mm; slice gap, 0.30; inversion time, 160 ms; matrix, 512 × 512); sagittal fat-suppressed, three-dimensional, spoiled gradient-echo sequence (TR, 20 ms; TE, 7.827 ms; slice thickness, 1.5 mm; no intersection gap; matrix, 512 × 512); and axial T2-weighted turbo spin-echo (TR, 6140 ms; TE, 100 ms; slice thickness, 3 mm; slice gap, 0.30; matrix, 512 × 512). The images were acquired with a field of view of 17 cm (proton-density-weighted sequence, sagittal T2 turbo spin-echo sequence), and 15 cm (all other sequences).
Statistical methods
Statistical analysis was performed with SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics was shown as mean ± standard deviation for continuous variables. We used analysis of variance with a repeated measure to examine the group differences for serum TAC, TOS, MDA, OSI levels over the various time intervals. Univariate paired test was used to examine the differences between pre-procedural and post-procedural TAC, TOS, MDA, and OSI levels. Fisher Exact was used for categorical data. Partial correlation analysis was used to control for the confounding factors in correlation analysis. Statistical significance was set at ≤ 0.05.
Results
Demographic features and baseline laboratory findings are shown in Table 2. We did not observe significant adverse effect or hemodynamic changes related to the procedures in either group.
Baseline demographic and laboratory values of the patients
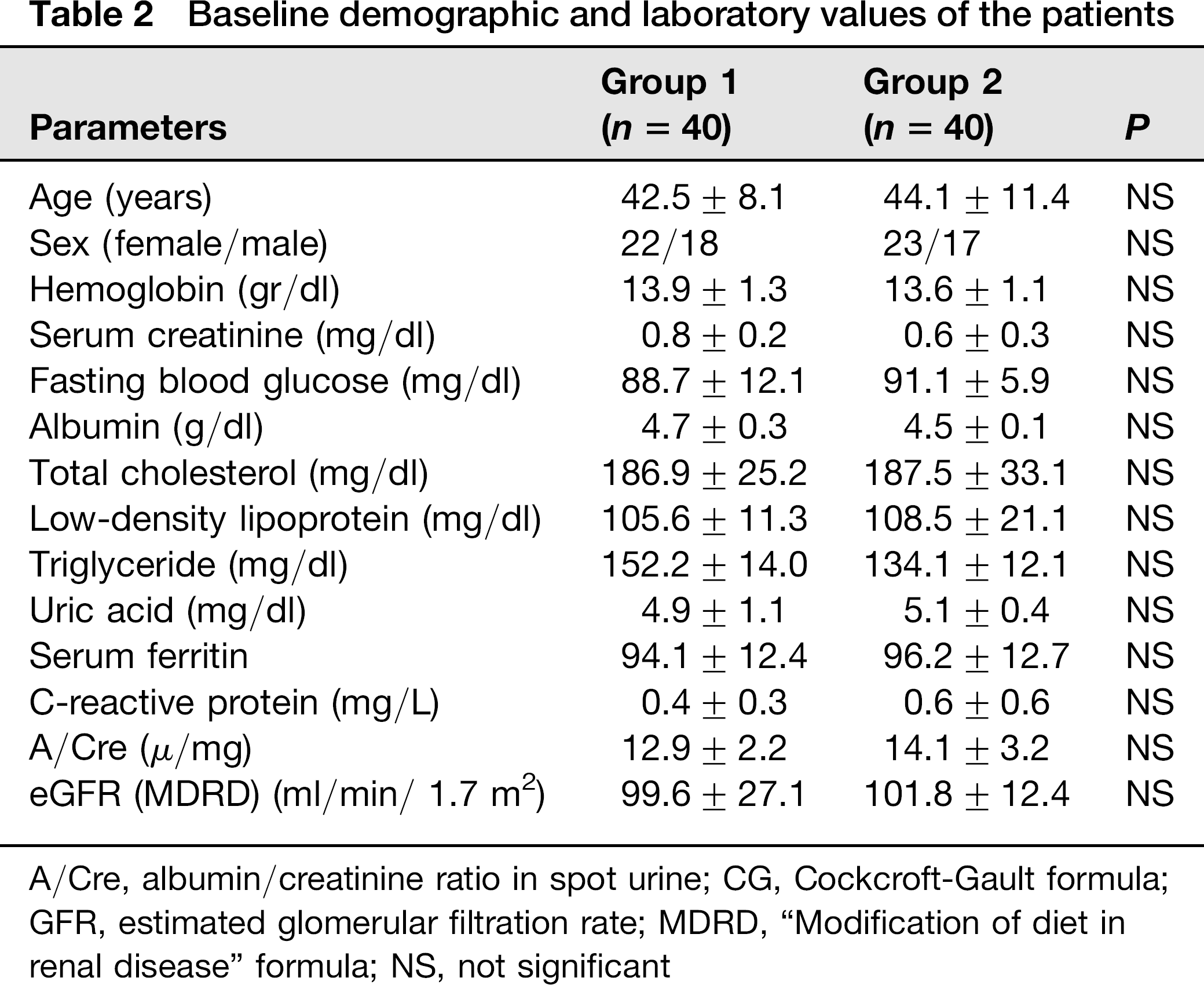
A/Cre, albumin/creatinine ratio in spot urine; CG, Cockcroft-Gault formula; GFR, estimated glomerular filtration rate; MDRD, “Modification of diet in renal disease” formula; NS, not significant
The comparative baseline values of TAC, TOC, OSI, and MDA levels in groups during the study are represented in Table 3. Serum TAC, TOS, OSI, and MDA levels were not different at baseline in both groups (P > 0.05). There were no significant changes in serum TAC, TOS, and MDA levels and median values (Δserum TAC, Δserum TOS, and ΔMDA) after 6, 24, or 72 h of the procedures in none of the groups (P > 0.05) (Table 3). Furthermore, OSI was found to be unchanged after the procedures in both groups (P > 0.05) (Table 3). There was no relationship between oxidant or antioxidant status, and clinical diagnosis of patients.
Oxidative stress biomarkers’ characteristics of the study groups
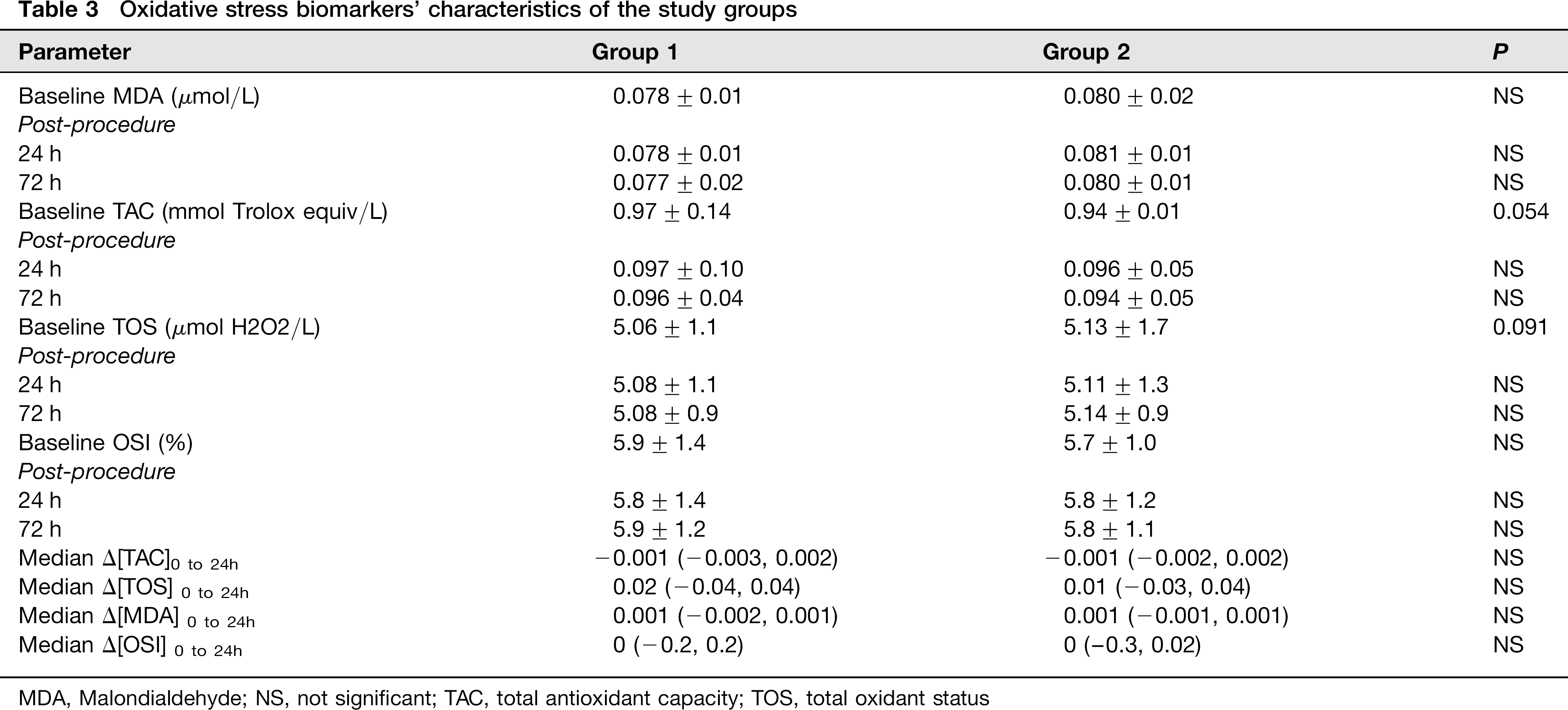
MDA, Malondialdehyde; NS, not significant; TAC, total antioxidant capacity; TOS, total oxidant status
Discussion
GBCA have significantly lower viscosity and are used at significantly lower volumes (4 to 11 times less) than ICAs, making them potentially less nephrotoxic. While GBCA are initially thought to be a safe alternative to ICAs for patients with chronic renal insufficiency, some clinical studies and case reports of gadolinium-associated acute renal failure have now been recorded, particularly in patients with underlying renal insufficiency.
In an experimental study, at the high dose of gadoverse-tamide (15 mmol/kg), all of the rats, and at the intermediate dose (5 mmol/kg), five of 10 animals showed microscopic vacuolization in the proximal convoluted tubules of the kidneys (10). Recently, Elmståhl et al. demonstrated that the histomorphological changes caused by gadolinium are similar to those caused by ICA, and are not related with the dose of contrast material in ischemic porcine kidneys (11). Furthermore, the same authors have also demonstrated that ICA (Iohexol) molecules were less nephrotoxic than the gadolinium chelates (gadopentetate and gadodiamid) in ischemic porcine kidneys (12).
In humans, early studies revealed that GBCA are relatively safe molecules in healthy persons (13) and in patients with kidney disease (14). In contrast, a number of recent studies suggested that GBCA agents exhibit variable degrees of nephrotoxicity. Nevertheless, the quality of these studies is poor, and the evidence of nephrotoxicity of gadolinium-based contrast agents is conflicting. Many of these studies are retrospective (15–17). Risk factor(s) has not been evaluated in many of such studies (16, 17). Types and doses of GBCA evaluated in these studies are not homogenous (16–18). The GBCA are classified into four main categories on the basis of their chemical structure and their charge. The various properties of the chelates have implications for possible toxicity and the risk of liberation of free ionic form (Gd3+) from its chelate (19). Therefore, different types of GBCA may have different toxicity potential. Furthermore, serum creatinine has been used for the assessment of renal function in many of the studies (15–17). A small sample size prospective randomized controlled study showed that gadobutrol has no benefit over ICA-based (Iohexol) angiography in patients with severely impaired renal function (20). In our prospective study, the same agent (GD) at a same dose (0.2 mmol/kg) was used in all patients. Renal function was assessed with glomerular filtration rate, microalbumin/creatinine ratio, and serum creatinine, during the study.
Direct tubular toxicity, renal ischemia, hemodynamic changes, hyperosmolality, and oxidative stress have been implicated in the pathogenesis of CIN, but their respective role remains to be unclear (21–24). Experimental findings in vitro and in vivo illustrate enhanced formation of ROS within the kidney following the administration of ICA, which may play a role in the development of CIN. Clinical studies support this possibility, suggesting a protective effect of ROS scavenging or reduced ROS formation with the administration of N-acetyl cysteine. Some authors have suggested that preventive strategies should include inhibition of ROS generation or ROS scavenging. On the other hand, many of the risk factors (renal failure, advanced age, diabetic nephropathy, congestive heart failure), predisposing to CIN are prone to enhanced renal parenchymal hypoxia and ROS formation.
What about the relationship between GBCA and oxi-dative stress? Mangafodipir (Manganese diprydoxyl phosphate) is a manganese-based contrast agent used in MRI that concentrates in the liver and displays pleiotropic antioxidant properties. Mangafodipir, a special superoxide dismutase (SOD) mimic with catalase and glutathione reductase activities, protects normal cells from apoptosis induced by H2O2 (25). On the other hand, two recent reports have shown that GBCAs cause rat cortical neurotoxicity by inducing intracellular oxidative stress (26). There are no clear data about GBCA in humans. We believe we have demonstrated for the first time that gadopentetate dimeglumine does not change the oxidant status in humans. On the other hand, there were not any factors other than gadopen-tetate dimeglumine administration and magnetic field that would have effect on the oxidative status during the study in our patients.
It is well-known that the effects of various oxidants and antioxidants in serum are additive. Thus, the measurement of different oxidants and antioxidants separately is not practical, and may not accurately reflect the true oxidative status of the organism. Serum levels of TAC, TOS, and OSI were measured as a reliable, sensitive and inexpensive direct measurement method (7, 9) in this study. Furthermore, in a recent study, it has been demonstrated that OSI alone has been shown to reflect oxidative status better than TOS or TAC (27). We have just demonstrated for the first time that TAC, TOS, MDA, and OSI values did not change after the MRI with or without gadopentetate dimeglumine.
Sirmatel et al. showed that the 1.5 T static magnetic fields used in the MRI apparatus did not yield a negative effect; on the contrary, it produced the positive effect of decreasing oxidative stress in men following short-term exposure (28). We did not detect either a negative or a positive effect of magnetic field on the oxidative stress markers in our patients.
To the best of our knowledge, there are no data regarding the influence of GBCAs on oxidant status, which is believed to have a role in development of acute kidney injury due to many conditions including contrast mediated nephropathy. In the present study, we investigated this topic for the first time and found that oxidant and antioxidant status were not influenced by the use of gadopentetate dime-glumine at a dose of 0.2 mmol/kg. In our opinion, this is a minor but important contribution to the data about GBCA-related toxicity.
In conclusion, either contrast-enhanced MRI (gado-pentetate dimeglumine, 0.2 mmol/kg) or MRI performed without contrast agents do not change oxidant and anti-oxidant status in humans. Studies including larger sample size are required to confirm these findings.