
Abstract
Background
Isotropic three-dimensional (3D) magnetic resonance imaging (MRI) has been applied to various joints. However, comparison for image quality between isotropic 3D MRI and two-dimensional (2D) turbo spin echo (TSE) sequence of the wrist at a 3T MR system has not been investigated.
Purpose
To compare the image quality of isotropic 3D MRI including TSE intermediate-weighted (VISTA) sequence and fast field echo (FFE) sequence with 2D TSE intermediate-weighted sequence of the wrist joint at 3.0 T.
Material and Methods
MRI was performed in 10 wrists of 10 healthy volunteers with isotropic 3D sequences (VISTA and FFE) and 2D TSE intermediate-weighted sequences at 3.0 T. The signal-to-noise ratio (SNR) was obtained by imaging phantom and noise-only image. Contrast ratios (CRs) were calculated between fluid and cartilage, triangular fibrocartilage complex (TFCC), and the scapholunate ligament. Two radiologists independently assessed the visibility of TFCC, carpal ligaments, cartilage, tendons and nerves with a four-point grading scale. Statistical analysis to compare CRs (one way ANOVA with a Tukey test) and grades of visibility (Kruskal-Wallis test) between three sequences and those for inter-observer agreement (kappa analysis) were performed.
Results
The SNR of 2D TSE (46.26) was higher than those of VISTA (23.34) and 3D FFE (19.41). CRs were superior in 2D TSE than VISTA (P = 0.02) for fluid-cartilage and in 2D TSE than 3D FFE (P < 0.01) for fluid-TFCC. The visibility was best in 2D TSE (P < 0.01) for TFCC and in VISTA (P = 0.01) for scapholunate ligament. The visibility was better in 2D TSE and 3D FFE (P = 0.04) for cartilage and in VISTA than 3D FFE (P < 0.01) for TFCC. The inter-observer agreement for the visibility of anatomic structures was moderate or substantial.
Conclusion
Image quality of 2D TSE was superior to isotropic 3D MR imaging for cartilage, and TFCC. 3D FFE has better visibility for cartilage than VISTA and VISTA has superior visibility for TFCC to 3D FFE and the visibility for scapholunate ligament was best on VISTA.
Magnetic resonance imaging (MRI) of the wrist has been a useful technique to detect abnormalities in the triangular fibrocartilage complex (TFCC), the scapholunate (SL) and lunotriquetral (LT) ligaments, tendons, peripheral nerves, and cartilage (1–4). However, the evaluation of small and complex structures such as ligaments, TFCC can be challenging with a wrist MRI (5–7). Therefore, accurate MRI of the wrist requires a high contrast and high spatial resolution.
For more than a decade, clinical MRI of the wrist has been performed with magnetic field strengths that range from 0.5–1.5 T (4). Recently, a 3.0T whole-body MRI system has become available for clinical use. The higher signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) obtained with 3.0 T MRI can result in the improved visualization of small anatomic structures in the wrist (8). Specifically, isotropic three-dimensional (3D) MRI permits multi-planar image reformations with different slice thicknesses in any imaging plane that may be helpful for the evaluation of complex structures. Isotropic 3D MRI using a gradient recalled echo (GRE) or turbo spin echo (TSE) sequence has been applied to various joints (8–12). However, to our knowledge, a comparison study for image quality between isotropic 3D MRI and 2D TSE sequence of the wrist at a 3T MR system has not been reported.
The purpose of our study was to compare the image quality between isotropic 3D TSE intermediate-weighted sequence and isotropic 3D fast field echo (FFE) and 2D TSE intermediate-weighted sequence of the wrist joint at 3T MRI in healthy volunteers.
Material and Methods
Subjects and MRI
The Institutional Review Board approved this HIPAA-compliant study, and informed consent was obtained. Ten healthy volunteers (four men and six women; age range, 26–31 years; mean age, 28 years) who had no history of operation or injuries of wrist joint were included in the study. MRI was performed in only one side of wrist in all volunteers. Therefore, 10 MR images of wrist were included in the study.
MRI of isotropic 3D turbo spin echo intermediate-weighted sequence with refocusing control (VISTA; Volume Isotropic Turbo Spin Echo Acqusition) and isotropic 3D fast field echo with water selective fluid (WATS-f) sequence and 2D turbo spin echo intermediate-weighted sequences were performed using a 3T whole-body MR scanner (Gyroscan Intera Achieva; Philips Medical Systems, Best, The Netherlands) with a receive-only 8-element phased-array coil. All subjects were imaged in the supine position with an arm by the side, and the dorsum of the hands should be parallel to the magnetic plane. The details of the MR protocol are described in Table1. The VISTA sequence was obtained utilizing a TSE 3D non-selective method, which uses short, non-volume selective TSE refocusing pulses, and thus allows for shorter echo spacing and prevents chemical shift artifacts. The k-space sampling order was low-to-high. Refocusing control was utilized to lower the specific absorption rate (SAR) with only a minor loss of the SNR in TSE scans with a long echo train length. Also, the driven-equilibrium (DRIVE) radio frequency reset pulse was applied at the end of a TSE echo train to accelerate the relaxation time and return to the equilibrium of the magnetization. Therefore, the total scan time can be decreased and flow void artifacts can be reduced by the enhancement of the fluid signal. Fat suppression was done utilizing spectral attenuated inversion recovery (SPAIR), which is a frequency selective adiabatic inversion pulse utilizing the difference in resonance frequencies of water and fat. The 3D FFE with WATS-f sequence is a non-spoiled FFE pulse sequence with the principle of selective excitation technique (ProSet), which is a selective excitation technique that uses a frequency and spatially selective excitation pulse. ProSet can improve the contrast and has no effect on scan time. The ProSet-water excitation provides selective water excitation and eliminates the fat signal by moving fat-induced artifacts.
MR sequence parameters
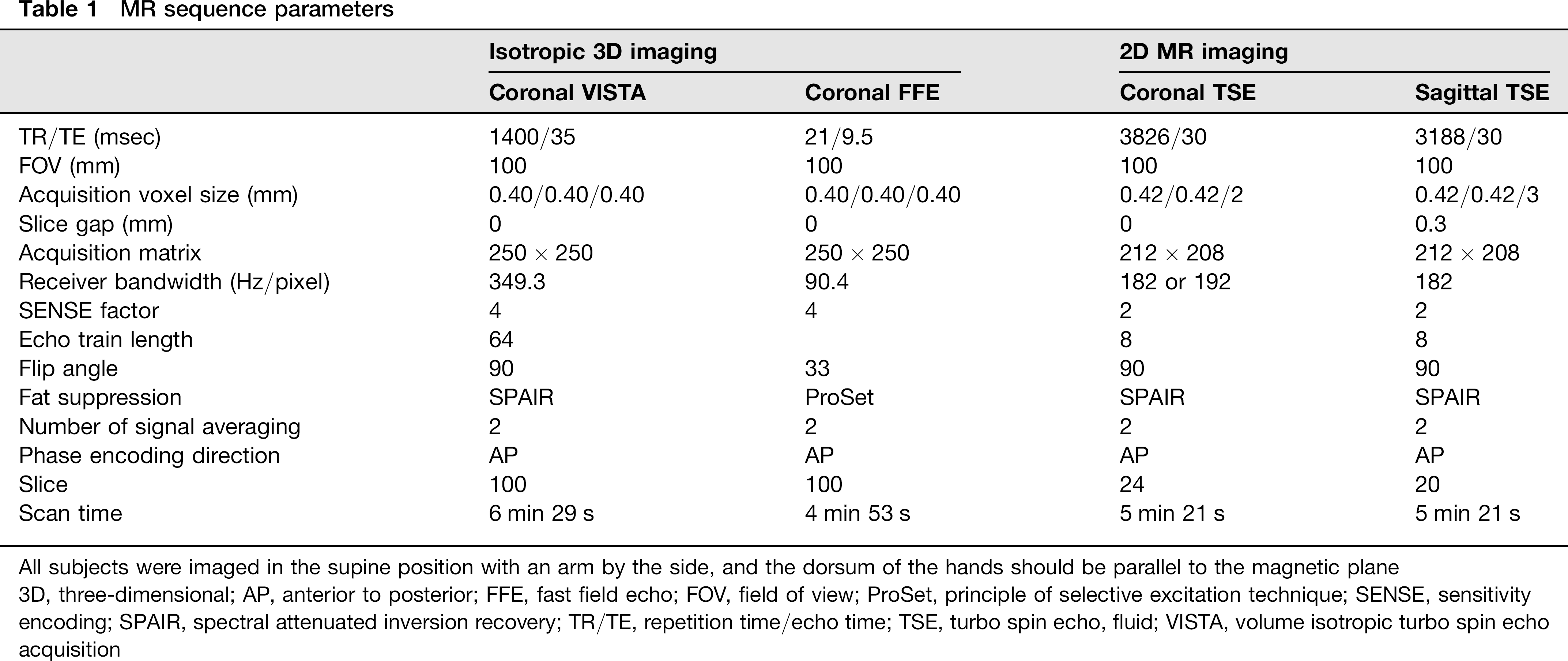
All subjects were imaged in the supine position with an arm by the side, and the dorsum of the hands should be parallel to the magnetic plane
3D, three-dimensional; AP, anterior to posterior; FFE, fast field echo; FOV, field of view; ProSet, principle of selective excitation technique; SENSE, sensitivity encoding; SPAIR, spectral attenuated inversion recovery; TR/TE, repetition time/echo time; TSE, turbo spin echo, fluid; VISTA, volume isotropic turbo spin echo acquisition
To quantitatively assess the SNR at parallel imaging, we measured noise via noise-only acquisitions (13). The bottle phantom containing 2000 mL of white mineral oil (liquid petroleum at 20°C, FAC phantom assembly; In vivo Corp., Orlando, FL, USA) was scanned with VISTA, 3D FFE, and 2D TSE sequences. The phantom was positioned at the center of the images and scanned in the sagittal plane. Noise-only data were acquired with the RF turned off for parameter of each sequences. Both object and noise-only data were reconstructed offline to apply parallel imaging calibration weights, homodyne partial Fourier phase correction and multichannel image combination to the noise-only data. To calculate the SNR of the phantom, regions of interest (ROIs) were placed in the reconstructed object images to measure mean signal intensities and duplicated in the noise-only reconstructions to measure noise.
Image analysis
Quantitative analysis: We measured the SNR in VISTA, 3D FFE, and 2D TSE sequences with the following calculation: SNR = mean of the object (Mobject)/standard deviation of the noise in the object (SDobject). As SDobject is biased by proper signal variation, it was estimated from the mean of the noise image at the same location. For a Rician distribution in the absence of the signal, the SDobject is calculated as the mean of the noise image/1.253 (14). Thus, the SNR = Mobject/SDobject = 1.253 × Mobject/Mnoise, where Mnoise is the mean of the noise image. To obtain the mean value of the object and the noise image, we applied 407 mm2 sized ROIs at the same position of the phantom image and noise data.
Also, image contrast ratios (CRs) were calculated between fluid and cartilage, TFCC, scapholunate (SL) ligament for coronal images of both isotropic 3D MRI and 2D TSE sequence (15–17). Polygonal ROIs were placed in the respective tissues, with each area as large as possible to avoid the inclusion of confounding structures (e.g. cortex, blood vessel) and the signal intensities (SI) were measured. ROIs were placed in the fluid of the triquetral-pisiform recess or radiocarpal joint, cartilage of the radiocarpal joint, central disc of TFCC, and SL ligament. To ensure consistency, all ROIs (size range, 4.4–30.4 mm2; mean size, 11.9 mm2) were made by the same radiologist (JYJ). The contrast ratios were calculated as follows: (SItissue1 2 SItissue2)/ (SItissue1 + SItissue2) where SItissue1 is mean SI of the reference tissue and SItissue2 is mean SI of the compared tissue. The three CRs per sequences were calculated as follows: CR of fluid-cartilage, CR of fluid-TFCC, CR of fluid-SL ligament.
Qualitative analysis: Visibility of the various anatomic structures was assessed by two radiologists who specialized in the musculoskeletal system (YCY/JYJ with 8 and 6 years of experience, respectively). Two radiologists independently evaluated MRI using picture archiving and a communication system (PACS, Centricity Radiology RA 1000; GE Healthcare, Chicago, IL, USA) in random order. At the time of image analysis, the radiologists could not be blinded to the parameters of each sequence. The reformation of 3D isotropic MR images was performed simultaneously during image analysis using Aquarius NET 1.8.2.6 (TeraRecon, Inc., San Mateo, CA, USA). Reformatted images with a slice thickness of 0.4 mm in the axial, sagittal and coronal planes were generated semi-automatically with a few mouse clicks after digital imaging and communications in medicine (DICOM) files of coronal images with each of the 3D sequences were imported to the program network from the PACS. The two radiologists graded the visibility of various anatomic structures, including TFCC, intercarpal ligaments, intercarpal cartilage, nerves and tendons using the 4-point scale as follows: a score of 1 indicated that a structure was not visible; a score of 2 indicated that a structure was visible but not able to be analyzed; a score of 3 indicated that a structure was visible and able to be analyzed; and a score of 4 indicated that a structure was excellently visible, with sharp outlines. In general, SNR, uniformity, and artifacts were used to grade the visualization (sharpness) of anatomic structures (18). Specifically, components of the TFCC which were classified into the central disc, meniscus homologue, and ulnar attachment were analyzed separately with the coronal plane of each of the MR sequences. Among intercarpal ligaments, the visibility of the SL and lunotriquetral (LT) ligaments was assessed on the coronal plane of each MR sequences. For the visibility of the intercarpal cartilage, the apposing cartilage of the radiocarpal joint was assessed on coronal plane of each MR sequences. Also, the visibility of median and ulnar nerves was evaluated on axial plane of each MR sequences except 2D TSE sequence. Finally, flexor and extensor tendons were evaluated on sagittal planes of each MR sequences.
Statistical analysis
We analyzed statistical differences in CRs between three sequences using a one-way ANOVA with a Tukey HSD (Honestly Significant Difference) test and grades of visibility between three sequences using the Kruskal-Wallis test. A P value < 0.05 was considered to indicate a statistically significant difference. Inter-observer agreement to evaluate MRI for the visibility of anatomic structures was calculated using κ statistics. Inter-observer agreement is rated as: a less than chance agreement for a κ value < 0; slight agreement for a κ value between 0.01 and 0.20; fair agreement for a κ value between 0.21 and 0.40; moderate agreement for a κ value between 0.41 and 0.60; substantial agreement for a κ value between 0.61 and 0.80; and almost perfect agreement for a k value between 0.81 and 0.99 (19).
Results
Quantitative analysis
In the phantom study, the SNR of 2D TSE (46.26) was the best one and that of VISTA (23.43) was superior to that of 3D FFE (19.41). The mean CRs of fluid-TFCC, fluid-cartilage, and fluid-SL ligament were higher in 2D TSE than both isotropic 3D MR images (Table2). CRs of fluid-cartilage were significantly superior in a 2D TSE than in a VISTA sequence (P = 0.02). The mean CRs of fluid-cartilage were higher in 3D FFE (0.31) than VISTA (0.26). However, there was no statistically significant difference. CRs of fluid-TFCC were significantly better in 2D TSE (P < 0.01) and VISTA (P = 0.01) than 3D FFE. The mean CRs of fluid-TFCC were higher in 2D TSE (0.77) than VISTA (0.67), although there was no statistically significant difference. The mean CRs of fluid-SL ligament in 2D TSE (0.61) was higher than those in VISTA (0.54), 3D FFE (0.52), however, without any statistically significant difference.
Image contrast ratios
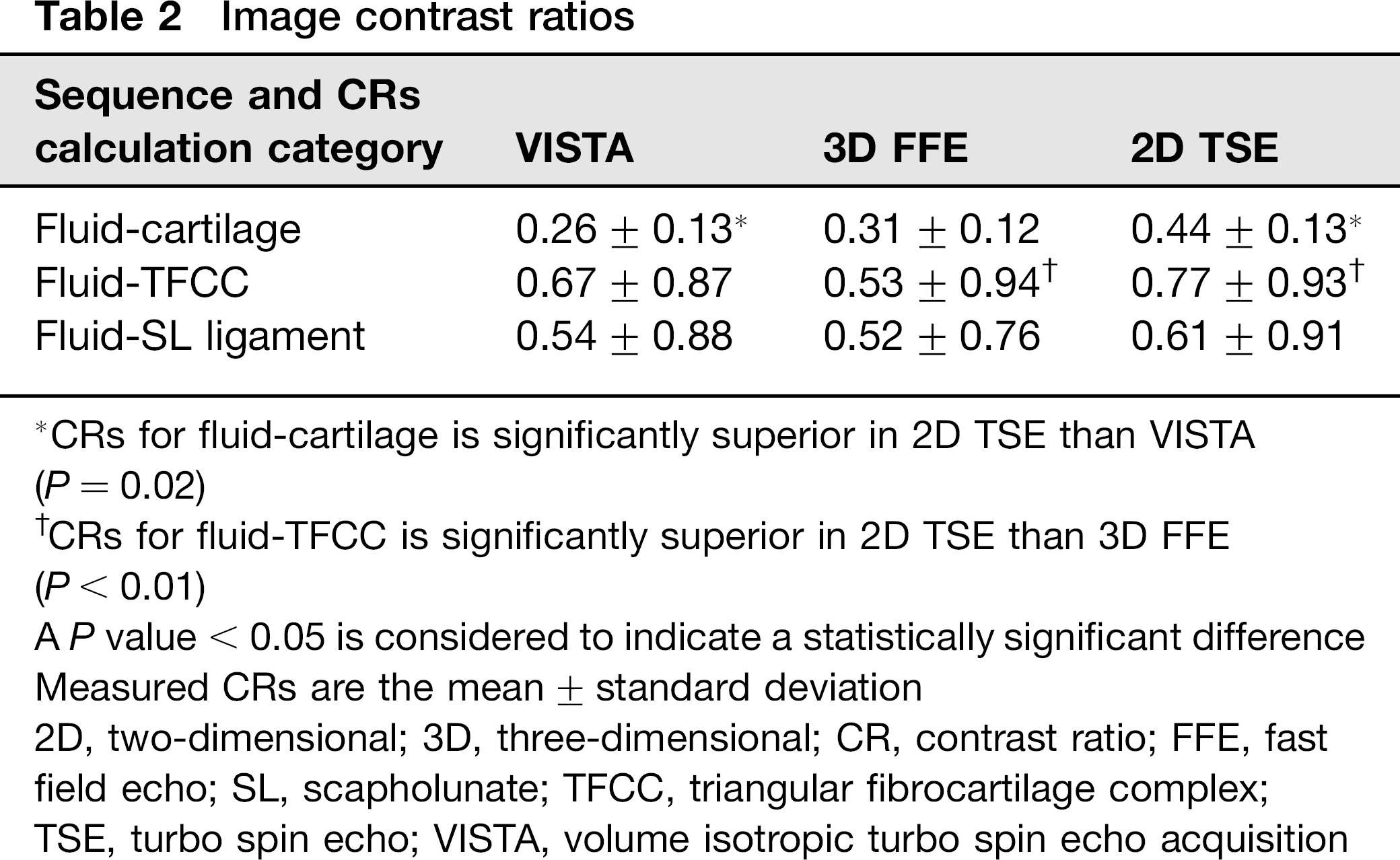
CRs for fluid-cartilage is significantly superior in 2D TSE than VISTA (P = 0.02)
CRs for fluid-TFCC is significantly superior in 2D TSE than 3D FFE (P < 0.01)
A P value < 0.05 is considered to indicate a statistically significant difference Measured CRs are the mean ± standard deviation
2D, two-dimensional; 3D, three-dimensional; CR, contrast ratio; FFE, fast field echo; SL, scapholunate; TFCC, triangular fibrocartilage complex;
TSE, turbo spin echo; VISTA, volume isotropic turbo spin echo acquisition
Qualitative analysis
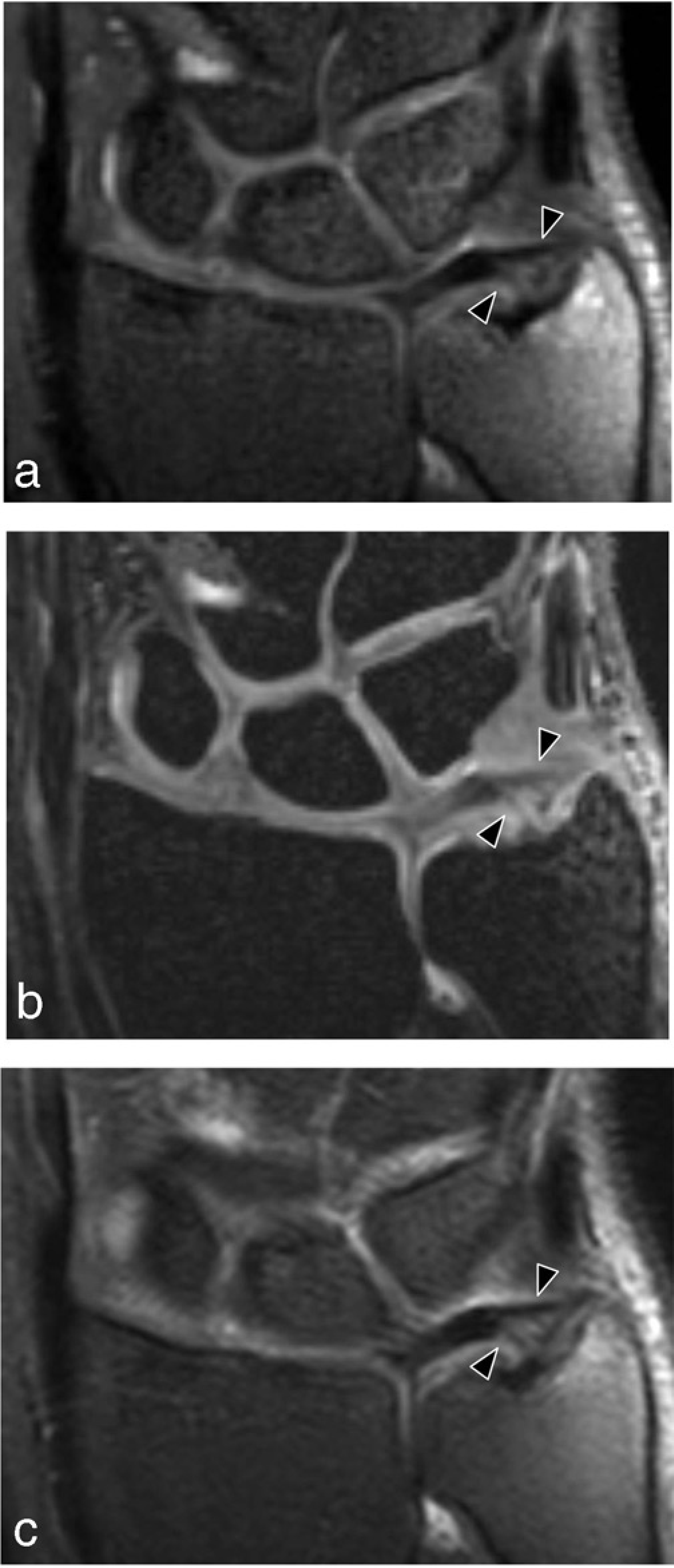
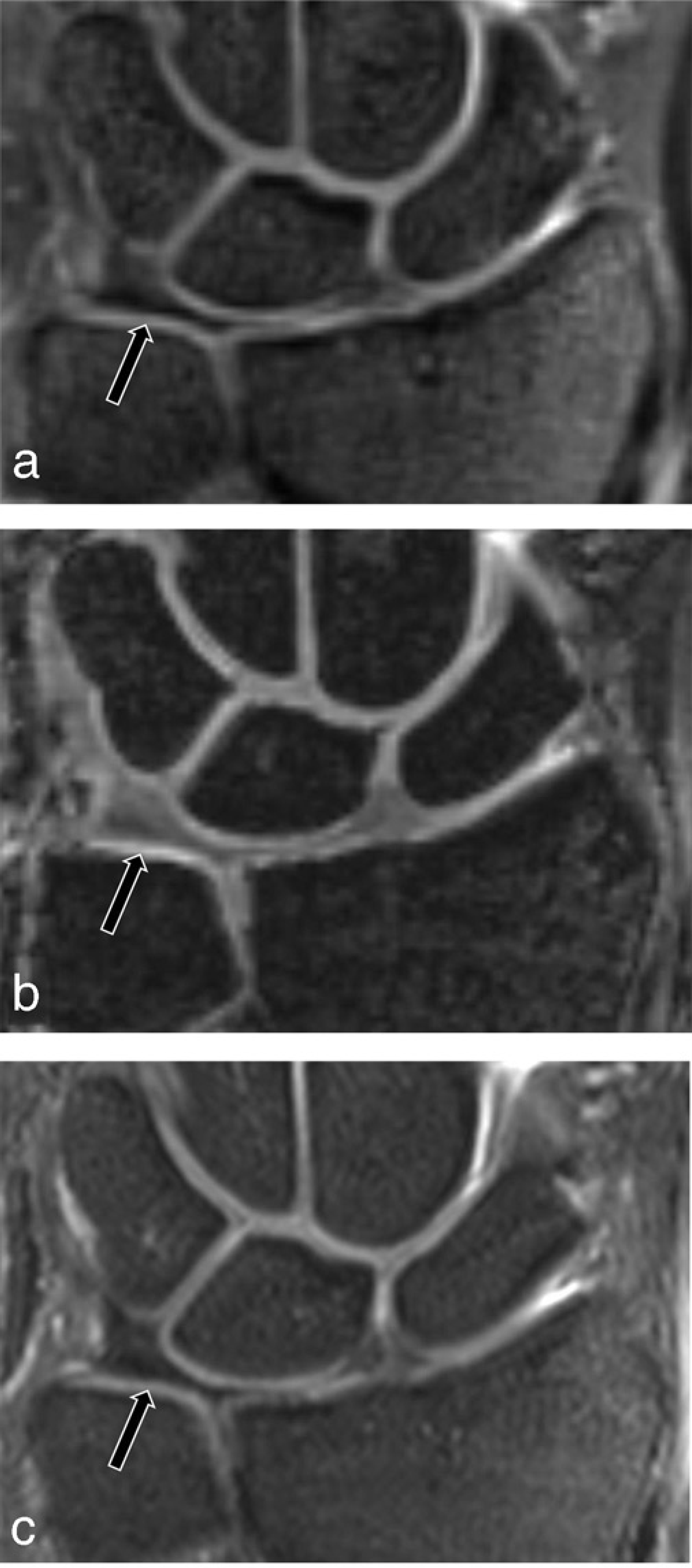
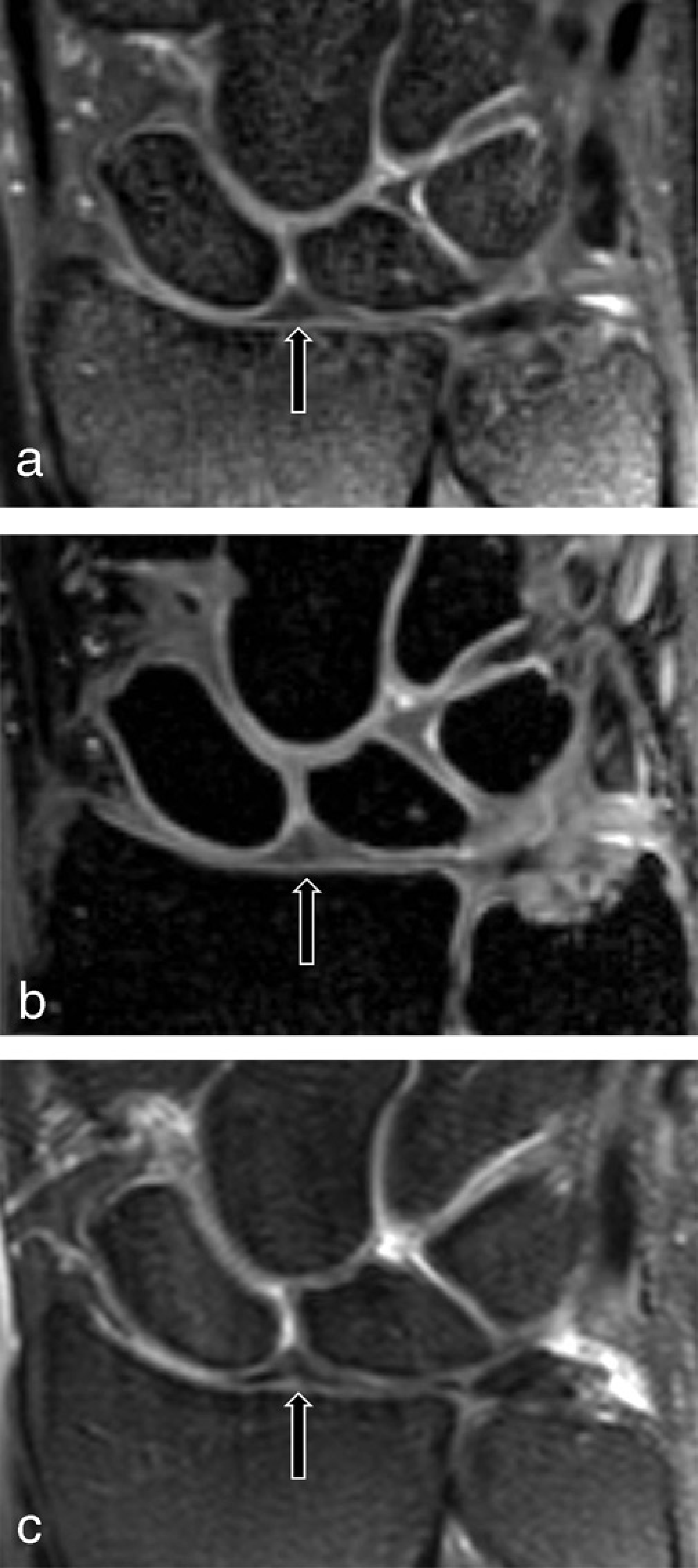
The results of the qualitative scores for the visibility of various anatomic structures are given in Table3. The visibility of cartilage was significantly better on 2D TSE and 3D FFE than on VISA (P = 0.04) (Fig. 1). The visibility of ulnar attachment and meniscus homologue of TFCC were best in 2D TSE and those of VISTA were significantly better than 3D FFE (P = 0.02 and P < 0.01) (Fig. 2). The visibility of central disc of TFCC was better on 2D TSE and VISTA than on 3D FFE, although there is no statistically significant difference (Fig. 3). Also, the visibility of the SL ligament was best in VISTA and that was significantly better in 2D TSE than 3D FFE (P < 0.01) (Fig. 4). The visibility of LT ligament was best on VISTA and better on 2D TSE than 3D FFE. However, there was no statistical significance. Inter-observer agreements for the visibility were in substantial agreement or moderate agreement (Table4). Inter-observer agreements for the visibility were the highest (k value = 0.80) for the evaluation of a LT ligament in a 2D TSE, median nerve in VISTA, central disc of TFCC in 3D FFE. Inter-observer agreement for the visibility was the lowest (k value = 0.41) for the evaluation of ulnar attachment of TFCC in 2D TSE.
Visualization grading of various anatomic structures

The visibility is significantly better than other sequence
The visibility is significantly best
The visibility of cartilage is significantly better on 2D TSE and 3D FFE than on VISA
A P value < 0.05 is considered to indicate a statistically significant difference
Data are mean grade of visibility ± standard deviation
2D, two-dimensional; 3D, three-dimensional; FFE, fast field echo; LT, lunotriquetral; R, radiologist; SL, scapholunate; TSE, turbo spin echo; VISTA, volume isotropic turbo spin echo acquisition
Inter-observer agreement for visibility of various anatomic structures
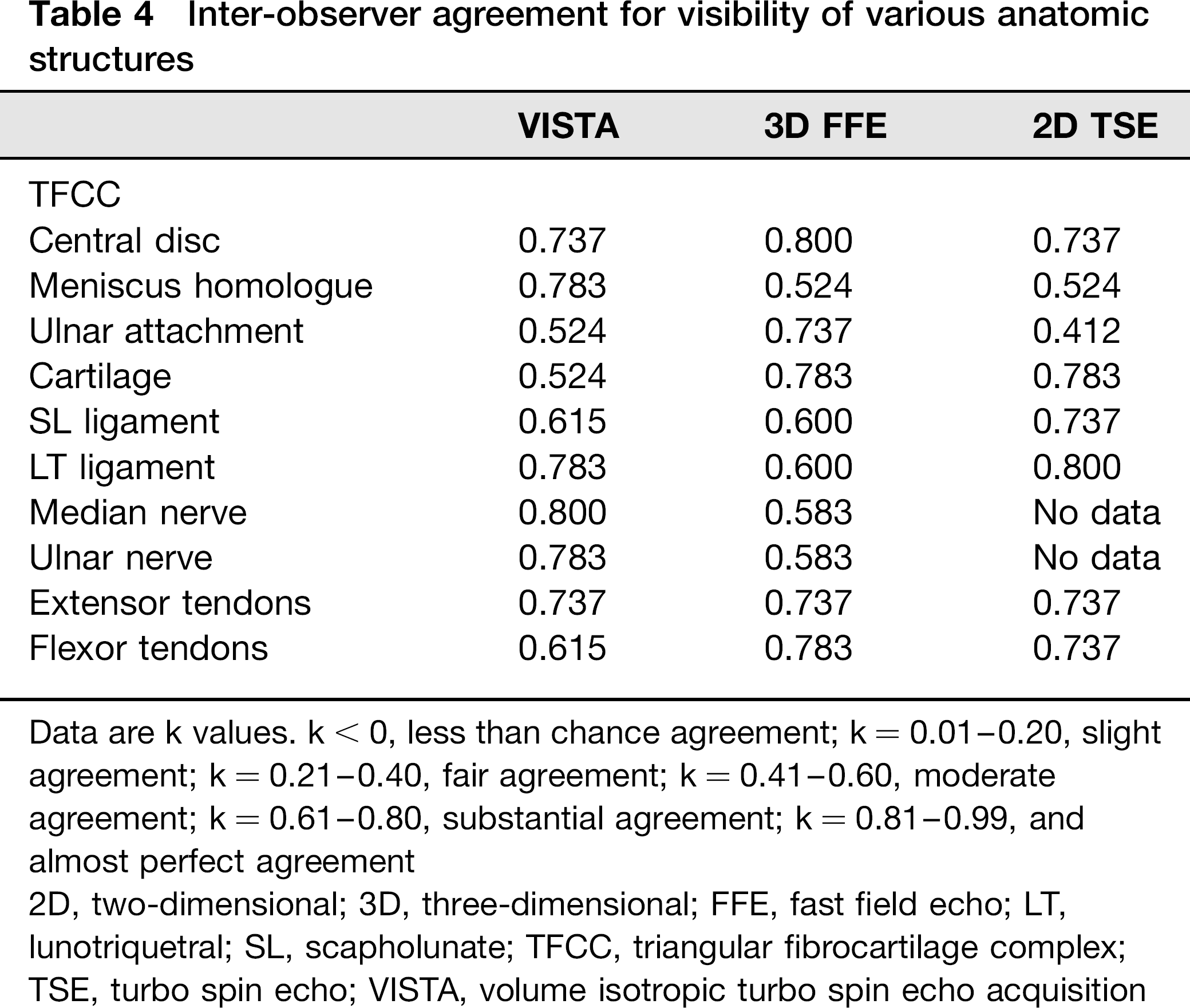
Data are k values. k < 0, less than chance agreement; k = 0.01–0.20, slight agreement; k = 0.21–0.40, fair agreement; k = 0.41–0.60, moderate agreement; k = 0.61–0.80, substantial agreement; k = 0.81–0.99, and almost perfect agreement
2D, two-dimensional; 3D, three-dimensional; FFE, fast field echo; LT, lunotriquetral; SL, scapholunate; TFCC, triangular fibrocartilage complex; TSE, turbo spin echo; VISTA, volume isotropic turbo spin echo acquisition
Coronal reformatted image of VISTA sequence with 0.4 mm slice thickness (a), coronal reformatted image of isotropic 3D FFE sequence with 0.4 mm slice thickness (b), and coronal 2D TSE intermediate-weighted MR image with fat suppression with 2 mm slice thickness (c) of a healthy 29-year-old woman show well-defined intercarpal cartilages (arrow heads) of radiocarpal joint. The visibility was graded as 4 on 2D TSE and isotropic 3D FFE and as 3 on VISTA by two radiologists Coronal reformatted image of VISTA sequence with 0.4 mm slice thickness (a), coronal reformatted image of isotropic 3D FFE sequence with 0.4 mm slice thickness (b), and coronal 2D TSE intermediate-weighted MR image with fat suppression with 2 mm slice thickness (c) of a healthy 29-year-old woman show ulnar attachment of TFCC (arrowheads). The visibility score was 4 on 2D TSE and VISTA and as 3 on isotropic 3D FFE by two radiologists Coronal reformatted image of VISTA sequence with 0.4 mm slice thickness (a), coronal reformatted image of isotropic 3D FFE sequence with 0.4 mm slice thickness (b), and coronal 2D TSE intermediate-weighted MR image with fat suppression with 2 mm slice thickness (c) of a healthy 26-year-old man show the central disc of TFCC (arrow). The visibility score was 4 on 2D TSE and VISTA and as 3 on isotropic 3D FFE by two radiologists Coronal reformatted image of VISTA sequence with 0.4 mm slice thickness (a), coronal reformatted image of isotropic 3D FFE sequence with 0.4 mm slice thickness (b), and coronal 2D TSE intermediate-weighted MR image with fat suppression with 2 mm slice thickness (c) of a healthy 27-year-old man show membranous portion of the scapholunate ligament (arrow). The visibility score was 4 on VISTA and 2D TSE and as 3 on isotropic 3D FFE by two radiologists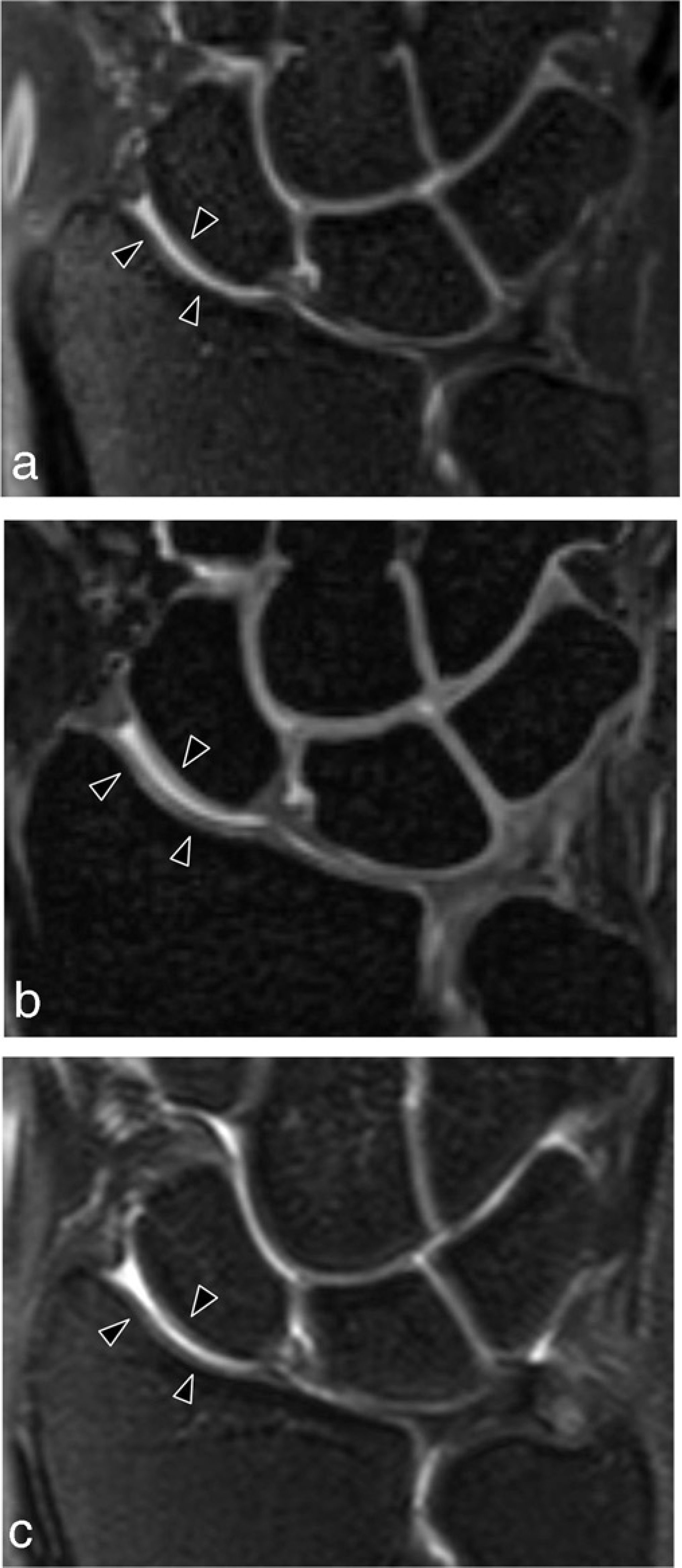
Discussion
Recently, MRI at high field strength such as 3.0 T, which can potentially provide superior spatial resolution by higher SNR has become increasingly available for musculoskeletal application (20–22). Saupe et al. reported that TSE and 3D FFE sequences at 3 T MRI of the wrist provide higher SNRs and CNRs as compared with those provided at 1.5 T MRI (18). Recently isotropic 3D MRI with multi-planar reformation of the wrist has been feasible with preserving image quality and acceptable acquisition time (8, 23). Isotropic 3D MRI is conceptually attractive for small joints such as a wrist joint because this sequence provides potentially improved visualization of small and complex anatomy by facilitating multi-planar image reformation in any desired imaging plane with different slice thicknesses after a scan acquisition. Isotropic 3D MRI has been clinically available with the TSE sequence as well as the GRE sequence at the 3T MR system of various joints (8–11, 23).
The main imaging techniques for MRI of the wrist has been 2D SE, TSE, and GRE including 3D GRE sequences (4, 24, 25). Many methods of 3D GRE imaging have been shown to be useful in cartilage evaluation, but have not replaced 2D FSE in the evaluation of internal derangements (26, 27). The GRE sequence has some disadvantages such as: susceptibility artifacts in the presence of metal or calcified structures, magic angle effects, and limited accuracy in the defection of degenerative changes in tendons and ligaments and a lack of tissue contrast necessary for musculoskeletal diagnosis (9, 12, 28). Fast spin-echo (FSE) sequences have favorable contrast characteristics for the assessment of hyaline cartilage, ligaments, tendons, and fibrocartilage (9, 29, 30). In a previous report, the CNRs of bone-muscle and those of bone-cartilage for 2D FSE sequence were high as compared to those for 3D FFE sequences on 3 T MRI of the wrist (18).
In our results, the 2D TSE sequence had superior SNRs than both isotropic 3D MR images. Also, this sequence had the highest mean value of CRs for fluid-cartilage, fluid-TFCC, fluid-SL ligament and significantly superior CRs for fluid-cartilage than those of VISTA and significantly superior CRs for fluid-TFCC than those of both isotropic 3D MR images. Our results were similar to previous studies.
In a comparison study between 2D FSE and isotropic 3D FSE at 3T MRI of the knee joint, Ristow et al. reported that effective CNR for fluid-cartilage and effective SNR were higher for 2D FSE than for the 3D FSE (31). Also, Gold et al. reported that fluid-cartilage CNR of 2D FSE was superior to that of 3D FSE XETA (extended echo-train acquisition) at 1.5T MRI of the knee joint, likely due to the longer repetition time (TR) used in 2D FSE (32). The SNR in parallel imaging is proportional to the SNR of a non-accelerated image divided by the square root of the acceleration factor (33). Therefore, in our study, the relative reduction in SNR due to parallel imaging is seen in isotropic 3D MR images as compared with 2D TSE. Also, voxel volume is one of the major imaging parameters for determining SNR and CNR. In general, a small voxel can be used to minimize of partial volume effects by an improved spatial resolution. However, it inevitably results in a decrease in the SNR and CNR. In our study, a small voxel which was used in 3D MR images result in that the SNR and a portion of CRs of 3D MR images were lower than these of 2D TSE.
In our results, the visibility on each of the MR sequences was different depending on anatomic structures. The visibility of TFCC was best in 2D TSE and the visibility of cartilage was better in 2D TSE than VISTA although that did not differ in 2D TSE and 3D FFE. It could be caused by a blurring in reformatted images of isotropic 3D MRI by the greater T2 decay during the long echo train. In a comparison study between 2D FSE and isotropic 3D FSE at 3T MRI of the knee joint, Ristow et al. reported that the image quality of a 2D FSE was rated higher than that of 3D FSE for anatomical structures including ligaments, cartilage, meniscus and a higher amount of image blurring was noted in the 3D FSE images (31). In another comparison study between isotropic 3D FSE cube and 2D FSE at 1.5T MRI of the wrist joint, it was reported that axial reformations of 3D FSE cube images suffer from blurring, likely due to T2 decay during the long echo train, limiting the overall image quality compared with that of 2D FSE images (23). Image blurring can be reduced by increasing the bandwidth at the expense of the SNR (20). The interaction between image blurring, acquisition time, bandwidth, and SNR is complex, with as many combinations as possible (34). Therefore, additional studies are needed to determine how bandwidth, echo train length, and parallel imaging acceleration of TSE can be optimized to minimize blurring while maintaining a sufficient SNR and clinically acceptable imaging times. Also, the results of this study may have been influenced by the two radiologists that are familiar with 2D TSE sequence rather than reformatted images of isotropic 3D MR images.
In our results comparing the VISTA and 3D FFE, the mean of the CRs of fluid-TFCC and the visibility of TFCC scored significantly higher on VISTA than 3D FFE. The visibility of the SL ligament was rated significantly higher on VISTA than 3D FFE and the mean of the CRs of fluid-SL ligament were higher on VISTA than 3D FFE, although the difference is not statistically significant. On the other hand, the visibility of the cartilage scored significantly higher on 3D FFE than VISTA and the mean of the CRs of fluid-cartilage were higher on 3D FFE than VISTA although the difference is not statistically significant. Therefore, our results suggest that 3D FFE offer a potentially superior evaluation for cartilage than VISTA but also that VISTA can provide a potentially superior evaluation for TFCC, ligaments as compared to 3D FFE.
2D MRI, which is obtained with standard orthogonal planes and a relatively thick slice thickness (2 mm), can have artifacts such as magic angle and partial volume effects because small structures of the wrist are oriented in various directions (31). Therefore, 2D sequences can potentially have a limit to fully assess the anatomic structures of wrist joint as compared with 3D isotropic MR images. In contrast, 3D isotropic MRI permits multi-planar reformation in any desired plane with thin slice thickness without slice gaps after a scan acquisition. These advantages of 3D isotropic MRI can decrease the partial volume effects and magic angle effects. Therefore 3D isotropic MRI with multi-planar reformation could be improve the visibility of anatomic structures. In our study, two radiologists analyzed the visibility of anatomic structures on orthogonal plane images of both 3D and 2D sequences to direct comparison of image quality between three sequences. However, the visibility of anatomic structures on isotropic 3D MR images with oblique multi-planar reformation could be superior to that on 2D MR images with orthogonal plane because isotropic 3D MR images can reformat oblique multi-planar images for various directions of complex anatomic structures in the wrist. Although the image quality of the isotropic 3D MR images scored lower as compared with 2D TSE sequences in our results, it may not induce a significant decline for diagnostic performances. Further comparison studies of diagnostic performance for internal derangement of the wrist joint between isotropic 3D MR images and 2D TSE sequence are needed.
This study had several limitations. First, only healthy volunteers were included in our study and the number of healthy volunteers was relatively small. Further studies will be required to compare the diagnostic accuracy of isotropic 3D MR images and 2D MR images with a correlation to arthroscopic findings and to compare the image quality between isotropic 3D MR images and 2D MR images on various MR scanners in large number of subjects. Second, blinding of the two radiologists to the sequence type was not possible because the individual sequences had specific morphologic features that may have made the sequences easily identifiable. Therefore, it may have introduced a bias.
In conclusion, the image quality of a 2D TSE intermediate-weighted sequence was superior to isotropic 3D MR imaging for cartilage, TFCC in a quantitative and qualitative analysis. 3D FFE has better visibility for cartilage than VISTA and VISTA has superior visibility for TFCC to 3D FFE and visibility for the scapholunate ligament on VISTA was best.