
Abstract
Background
Although CT coronary angiography (CTCA) and MR coronary angiography (MRCA) are increasingly used in patients with Kawasaki disease, comparison of coronary artery assessibility and diagnostic performance between the two imaging modalities has been rarely performed.
Purpose
To investigate which imaging modality, CTCA or MRCA, is better for evaluating coronary artery abnormalities in patients with Kawasaki disease.
Material and Methods
Between 2003 and 2011, 56 patients (38 boys/men; age range, 1–24 years) with Kawasaki disease underwent CTCA or MRCA (group A). Of these, 17 underwent both CTCA and MRCA (group B). Visibility of 11 coronary arterial segments in each patient was graded on a four-point scale. Coronary artery aneurysm, stenosis, and occlusion were evaluated by CTCA and MRCA, based on a reference standard obtained from cardiac catheterization, echocardiography, follow-up CTCA and MRCA, and clinical history. Coronary artery assessibility and diagnostic performance were compared between CTCA and MRCA.
Results
In per-segment analysis, more segments were assessable on CTCA than on MRCA in both groups. In per-patient analysis of group B, no significant difference in the assessibility was found between CTCA (95.0%, 128.3/135 segments) and MRCA (92.4%, 124.8/135 segments) (P > 0.05). Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of CTCA vs. MRCA were 93.1% vs. 77.9% (P, 0.001), 99.2% vs. 99.7% (P = 0.65), 96.8% vs. 98.7% (P = 0.65), 98.2% vs. 94.1% (P < 0.001), and 98.0% vs. 94.9% (P = 0.008), respectively, in group A, and 91.8% vs. 70.4% (P < 0.001), 99.5% vs. 99.5% (P = 1.000), 98.5% vs. 98.0% (P = 1.000), 97.2% vs. 91.1% (P = 0.006), and 97.6% vs. 92.3% (P = 0.004), respectively, in group B.
Conclusion
Although CTCA and MRCA show comparable assessibility in per-patient analysis, CTCA shows higher diagnostic performance than MRCA for evaluating coronary artery abnormalities in patients with Kawasaki disease.
Kawasaki disease, first described in Japan by Tomisaku Kawasaki in 1967, is an acute, self-limiting vasculitis of unknown etiology (1). It predominantly affects infants and young children under the age of 5 years; there is a regional preponderance in Asians and Pacific islanders (2). Although high-dose intravenous immunoglobulin infusion is an effective treatment for the acute phase of the disease, approximately 5% of patients still develop coronary artery aneurysms. These aneurysms undergo remodeling over time and may be complicated by steno-occlusive lesions (3). Of note, the risk of ischemic heart disease is higher in the first year after onset of the illness, and in larger and longer coronary aneurysms (1). Given the dynamic process of the involved coronary arteries, the morphology of coronary aneurysms should be accurately depicted during the initial examination and the development of steno-occlusive lesions in the affected coronary artery segments should be identified as early as possible during follow-up. In this respect, non-invasive and accurate coronary artery imaging is essential for assessing coronary artery abnormalities in patients with Kawasaki disease.
Although catheter coronary angiography (CCA) is frequently regarded as a diagnostic reference standard, it cannot be routinely performed for diagnostic purposes in children and adolescents due to its invasiveness and radiation hazard. Echocardiography (ECHO) is limited in its ability to assess distal coronary arteries, and evaluation of coronary arteries becomes gradually more difficult as a patient grows. In recent years, imaging techniques of CT coronary angiography (CTCA) and MR coronary angiography (MRCA) have noticeably improved. As a result, CTCA and MRCA have been increasingly used for assessing coronary artery abnormalities in patients with Kawasaki disease (4–14). Nonetheless, to the best of our knowledge, only one study has compared CTCA and MRCA with CCA (the gold standard) for assessing coronary artery abnormalities in patients with Kawasaki disease (13). Therefore, the objective of this study was to investigate which imaging modality, CTCA or MRCA, is better for assessing coronary artery abnormalities in patients with Kawasaki disease.
Material and Methods
This retrospective study was approved by our institutional review board and the requirement for written informed consent was waived. All numerical data are expressed as the mean ± standard deviation.
Patient population
A total of 56 patients (38 boys/men, 18 girls/women; age 13.2 ± 5.7 years; range, 1–24 years) with Kawasaki disease, who underwent CTCA (n = 58) or MRCA (n = 39) between 2003 and 2011, were included in this study. The age at onset of Kawasaki disease ranged from 2 months to 12 years 9 months (4.1 ± 3.4 years). Of these, 17 (13 boys/ men, 4 girls/women; age 13.9 ± 5.2 years; range, 2 months to 24 years; age at the disease onset, 4.3 ± 3.7 years; range, 3 months to 12 years 9 months) underwent both CTCA (n = 26) and MRCA (n = 26). Patients were classified into two groups: those who underwent either CTCA or MRCA were categorized into group A, and those who underwent both CTCA and MRCA were categorized into group B (Table 1). In 19 of the 56 patients, CCA (n = 29) was also performed. Of these 19 patients, CTCA and MRCA were performed in eight patients; only CTCA was performed in nine patients; and only MRCA was performed in two patients. All patients had undergone ECHO as an initial or follow-up study. The inter-study interval between CCA, CTCA, and MRCA, ranged from 1-193 months (29.6 ± 31.2 months).
Patient characteristics
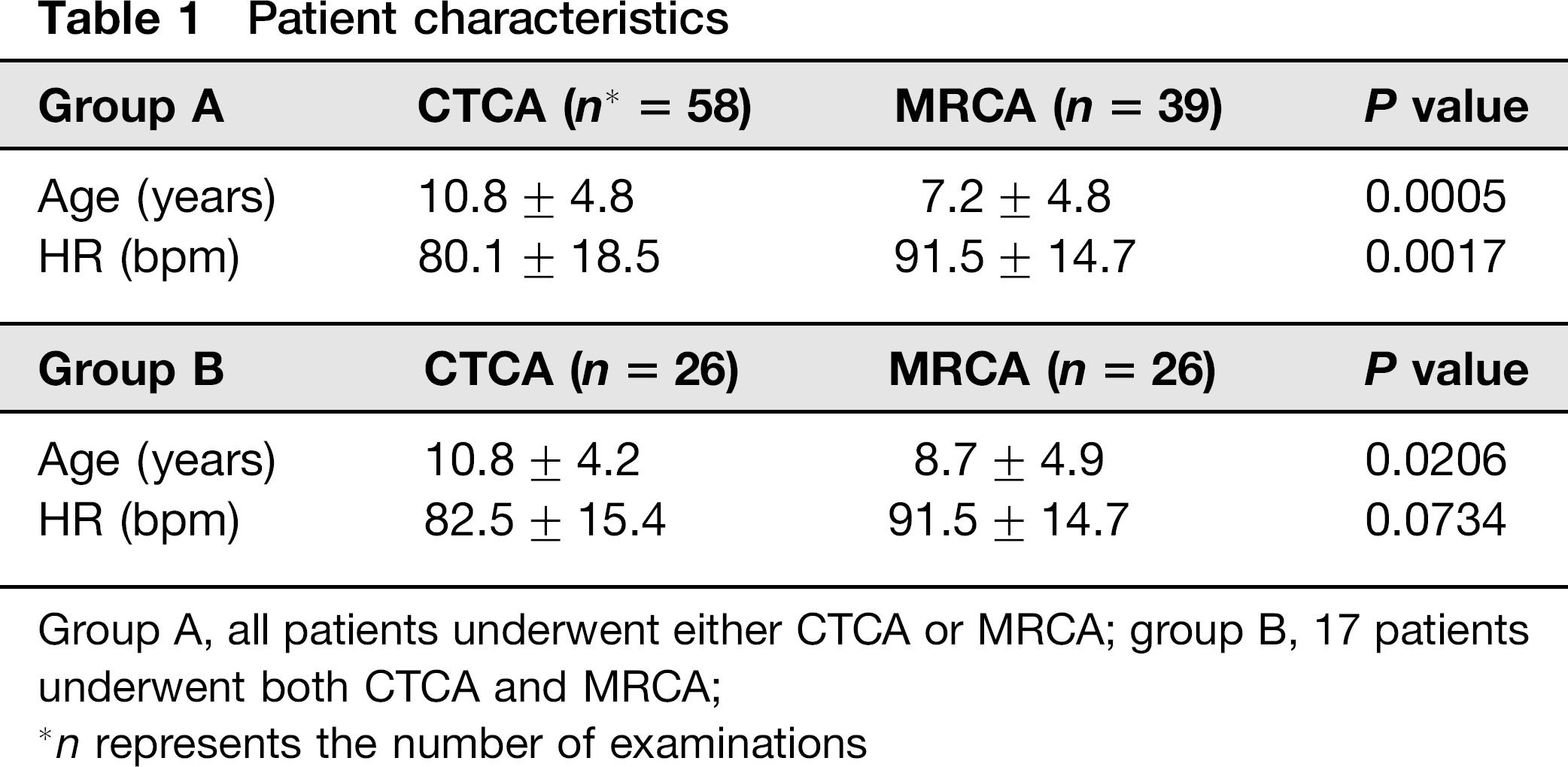
Group A, all patients underwent either CTCA or MRCA; group B, 17 patients underwent both CTCA and MRCA;
n represents the number of examinations
CTCA
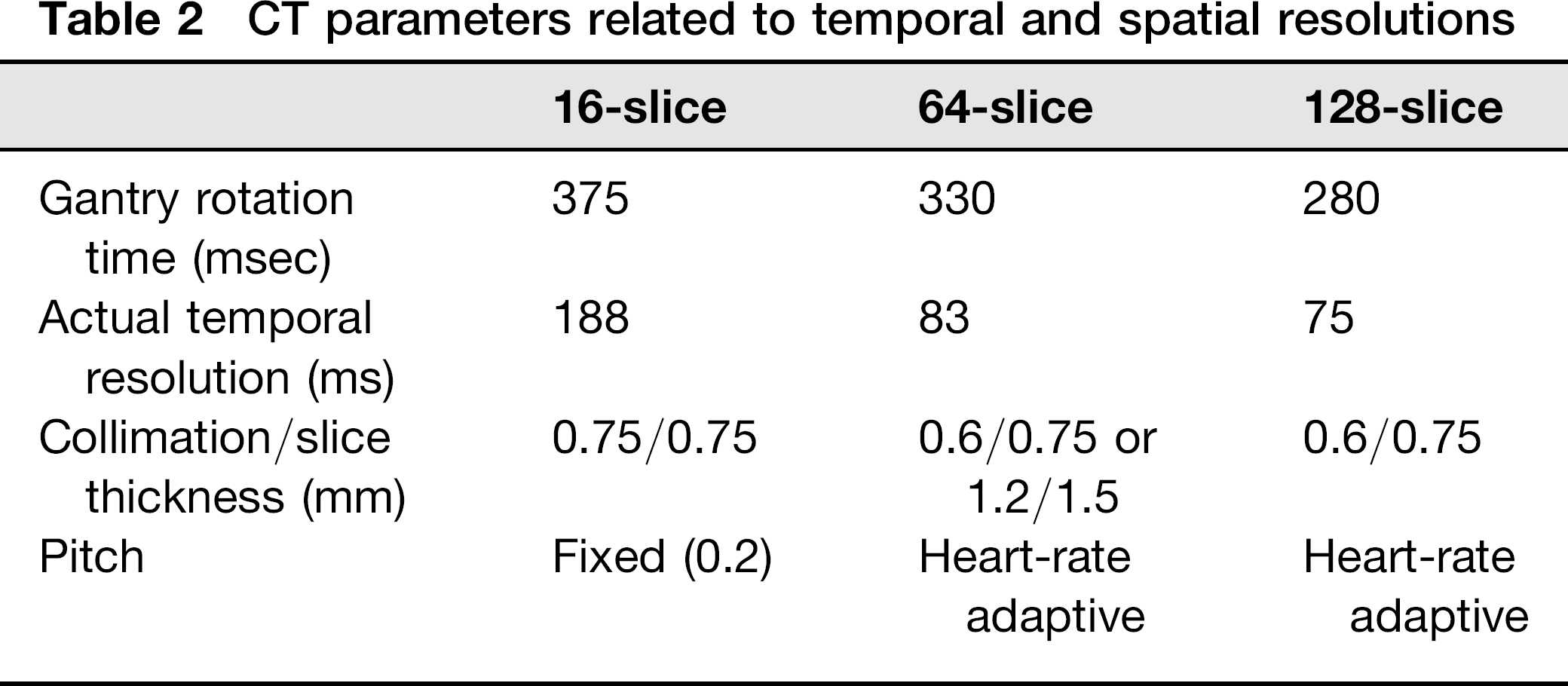
CTCA was performed using a single-source 16-slice scanner (SOMATOM Sensation 16; Siemens Healthcare, Forchheim, Germany; n
CT parameters related to temporal and spatial resolutions
Radiation dose optimization
Dose parameters of CTCA, such as kV, mAs, and volume computed tomography dose index (CTDIvol), were determined according to body-size adapted protocols (15-17). Eighty kVp was used in three studies, 100 kVp was used in 14 studies, and 120 kVp was used in 41 studies. Attenuation-based, combined tube current modulation (CARE Dose 4D; Siemens Healthcare) was used to reduce CT radiation dose while maintaining image quality (16, 18). In addition, ECG-controlled tube current modulation, in which 20% or 4% of full radiation dose was used outside the target cardiac phase for coronary artery imaging, was used for retrospective ECG-gated spiral scanning to reduce radiation dose (14,15).
Administration of intravenous contrast agent
Dual-phase intravenous injection of an iodinated contrast agent (iomeprol-400, 400 mgI/mL; Bracco Imaging SpA, Milan, Italy; weight-based amount, 1.0-1.5 mL/kg) followed by a saline chaser, was performed with a dual-head power injector via an arm vein. Ten seconds after administration of the contrast agent, bolus tracking was started to detect threshold enhancement of 100 HU in the descending aorta (17,19-21). Delay time was set to 7 or 8 s after reaching the threshold. Thus, the overall scan delay for CT scanning was 17 s or longer. The injection rate was adjusted according to the size of the angiocatheter and the maximum allowable injection rate estimated by an experienced CT nurse.
Image processing
Thin axial CT data were transferred to a commercially available workstation (AW; GE Healthcare, Milwaukee, WI, USA, or Leonardo; Siemens Healthcare) for multiplanar and three-dimensional image reconstruction of coronary arteries using oblique or curved multiplanar reconstruction (MPR), maximum-intensity projection (MIP), and volume rendering.
MRCA
MRCA was performed in 36 of 39 patients using a 1.5-T MRI system (Gyroscan Intera; Philips Healthcare, Best, The Netherlands) with a five-element, cardiac phased-array coil. In the remaining three patients, MRCA was performed using a 1.5-T MRI system (Achieva; Philips Healthcare) with a five-element, cardiac phased-array coil in one patient or with a 32-element, cardiac phased-array coil in two patients. Nitroglycerin was used in one patient and beta-blockers were not used in any patients.
Initial survey images were obtained in three orthogonal planes to help determine the position of the heart. A reference image was then obtained to evaluate the individual coil sensitivities for subsequent sensitivity-encoding (SENSE) imaging. To determine the motion of the coronary arteries, multiphase four-chamber cine MRI was obtained using a steady-state free precession (SSFP) pulse sequence and the following parameters: TR, 2.6 msec; TE, 1.3 msec; flip angle, 60°; in-plane resolution, 1.25 × 1.25 mm; slice thickness, 8 mm; NEX, 1; the number of cardiac phases, 50-80; and SENSE factor, 2.5). The motion of the coronary artery was visually assessed to determine the rest period of cardiac motion. Based on this visual assessment, a subject-specific trigger delay and an acquisition window at either end-systole or mid-diastole were determined for MRCA. MRCA was acquired using either a target-volume or a whole-heart approach.
Target-volume coronary angiography
A three-point plan technique was used to determine the coordinates of target-volumes (usually two target-volumes: each for the right coronary artery [RCA] and for the left coronary artery [LCA]). Navigator-gated, electrocardiography-triggered, fat-suppressed, thee-dimensional segmented k-space SSFP sequence (TR, 5.8 msec; TE, 2.9 msec; flip angle, 90°; voxel size, 0.9 × 0.9 × 3 mm; NEX, 1; and SENSE factor, 2.0) was used for target-volume MRCA. Navigator acceptance window ranged from 3 mm to 5 mm depending on patient body size. A T2 preparation pulse (50 msec) was used to improve coronary artery visualization. A volume shim was applied to the entire heart to improve magnetic field homogeneity. In this target-volume approach, distal coronary segments were commonly excluded from the evaluation. The scan time for target-volume MRCA ranged from 30 min to 1 h, depending on the gating efficiency.
Whole-heart coronary angiography
In the whole-heart approach, MRCA images of the entire heart were obtained in a transaxial plane by using balanced SSFP sequence (TR, 4.8 msec; TE, 2.4 msec; flip angle, 90°; NEX, 1; and SENSE factor, 2.0) with almost isotropic voxel size (1.35 × 1.34 × 1.5 mm) (22). Thus, in contrast to the target-volume approach, the coronary arteries including the distal segments were included in their entirety for the assessment. Other parameters were the same as those used in the target-volume approach. The scan time for whole-heart MRCA was shorter than that for target-volume MRCA, ranging from 5 min to 30 min depending on the gating efficiency and the cardiac coil. In both approaches, the field of view and the imaging matrix were adjusted according to the patient's body size.
Image processing
All MRCA data were transferred to a commercially available workstation (Easy Vision or View Forum; Philips Healthcare) to produce MPR, MIP, and volume-rendered images. In addition, another software tool (SoapBubble Tool; Philips Healthcare, Best, The Netherlands) was used to produce curved planar reformatted coronary artery imaging coupled with two-dimensional projection (23).
Image analysis and assessment
The coronary artery tree was divided into 11 segments, according to a modified American Heart Association (AHA) scheme (Fig. 1) (21): the proximal RCA (segment 1), the middle RCA (segment 2), the distal RCA (segment 3), the posterior descending artery (segment 4), the left main artery (segment 5), the proximal left anterior descending (LAD) artery (segment 6), the middle LAD artery (segment 7), the distal LAD artery (segment 8), the proximal left circumflex (LCx) artery (segment 9), the middle LCx artery (segment 10), and the distal LCx artery (segment 11). Side branches were excluded from the analysis.
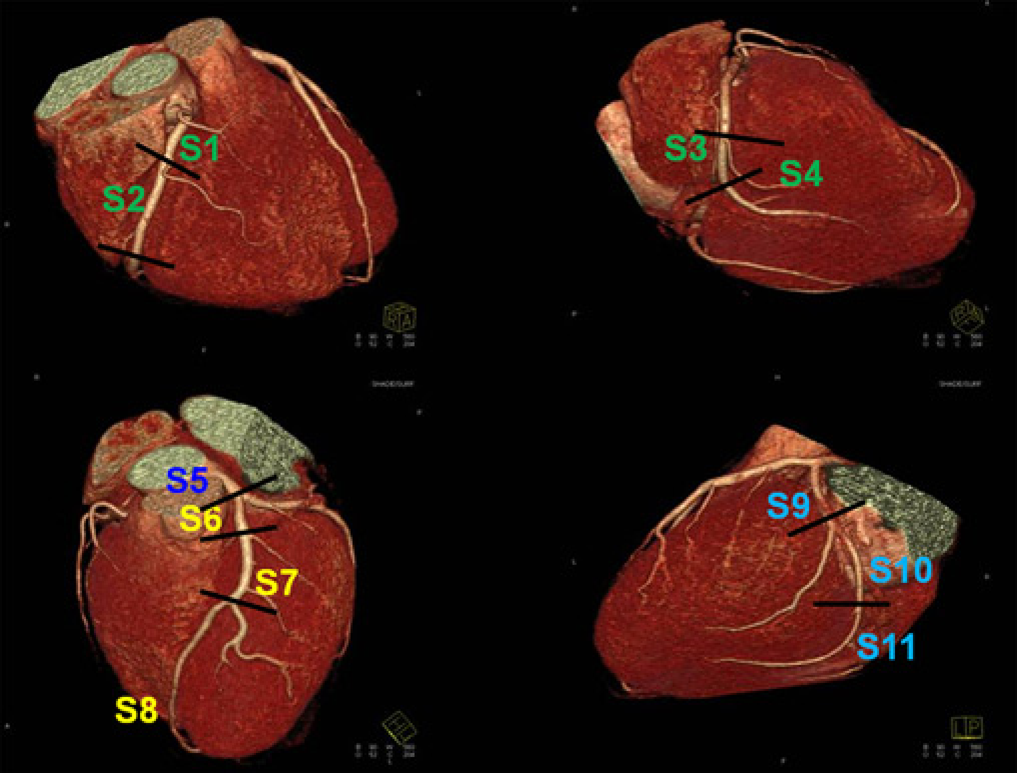
Modified segmental model of coronary artery anatomy based on the American Heart Association classification system: the proximal right coronary artery (RCA) (S1), the middle RCA (S2), the distal RCA (S3), the posterior descending artery (S4), the left main artery (S5), the proximal left anterior descending (LAD) artery (S6), the middle LAD artery (S7), the distal LAD artery (S8), the proximal left circumflex (LCx) artery (S9), the middle LCx artery (S10), and the distal LCx artery (S11)
Two experienced radiologists assessed coronary artery visibility and coronary artery abnormalities on CTCA and MRCA in consensus. Coronary artery visibility was graded on a four-point scale for each coronary artery segment (Fig. 2): 1, excellent (no artifacts, unrestricted evaluation); 2, good (minor artifacts, good diagnostic quality); 3, adequate (moderate artifacts, acceptable for routine clinical diagnosis); 4, poor (severe artifacts impairing accurate evaluation). Scores ≤ 3 were considered to be a clinically assessable image quality. Reasons for poor visibility were determined as follows: poor vessel signal; calcium deposits; overlapped adjacent structures (such as cardiac chambers or cardiac veins); and motion artifacts. In addition to non-assessable segments (score = 4), some segments were absent because most distal coronary artery segments were not included in target-volume MRCA. There were 91 and 49 absent segments in group A and group B, respectively. For the per-patient analysis in group B, 49 absent segments were excluded from the evaluation and the visual grades on multiple CTCAs or MRCAs were averaged for each patient.
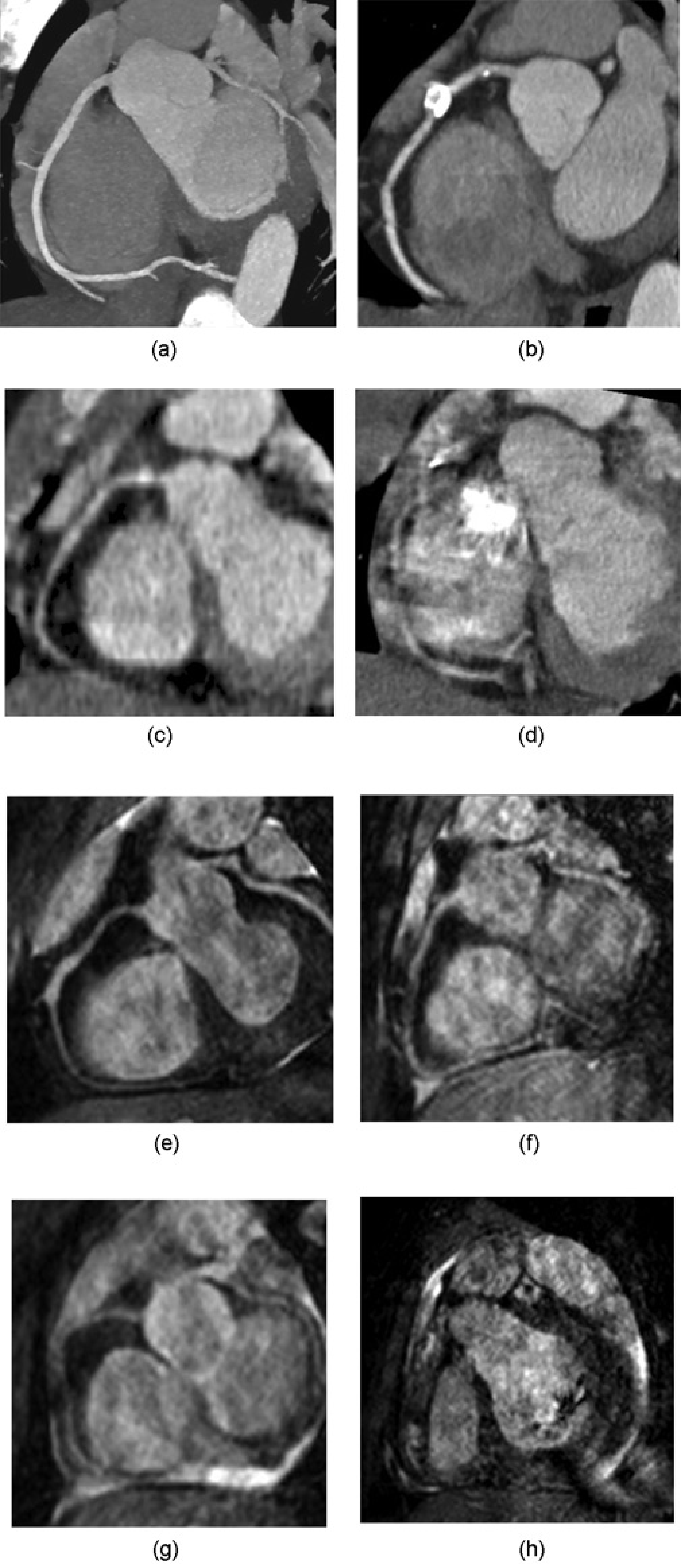
Visual grades of coronary artery visibility on CTCA (a–d, grades 1–4) and MRCA (e–h, grades 1–4). Coronary artery visibility was graded on a four-point scale for each coronary artery segment: grade 1, excellent (no artifacts, unrestricted evaluation); grade 2, good (minor artifacts, good diagnostic quality); grade 3, adequate (moderate artifacts, acceptable for routine clinical diagnosis); grade 4, poor (severe artifacts impairing accurate evaluation)
For the assessment of coronary artery abnormalities including aneurysm, stenosis, and occlusion, a reference standard was determined by CCA, ECHO, follow-up CTCA and MRCA, and clinical history. Segments were considered aneurysmal when the internal diameter was ≥1.5 times that of an adjacent segment. Aneurysms were measured perpendicular to the long axis of the vessel at the site showing the greatest diameter. Aneurysms were categorized as small (internal diameter <5 mm), medium (internal diameter 5 mm to ≤8 mm) or giant (internal diameter > 8 mm). A semi-quantitative scale was used to grade the degree of luminal stenosis as a percentage: no stenosis, 1-29%; mild stenosis, 30-49%; moderate stenosis, 50-69%; severe stenosis, 70-99%; and occlusion, 100% stenosis (24).
Statistical analyses
In group A, coronary artery assessibility was compared between CTCA and MRCA, for the three different CT scanners, and between the two MRCA approaches (target-volume vs. whole-heart). In group B, coronary artery assessibility were compared between CTCA and MRCA using the χ2 test after excluding absent segments. Segment-based sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of CTCA and MRCA in identifying coronary artery abnormalities based on the reference standard were compared between CTCA and MRCA using Fischer's exact test. Statistical analyses were performed using a commercially-available program (SPSS; version 18.0; SPSS, Inc., Chicago, IL, USA). P values < 0.05 were considered to indicate a statistically significant difference.
Results
CT radiation dose
In seven of 58 examinations, radiation dose estimates could not be calculated because their CT dose reports were not available. Thus, radiation dose of CTCA was estimated for the remaining 51 examinations. The CTDIvol and dose-length product (DLP) values for CTCA were 15.3 ± 12.0 mGy (range, 1.9–51.9 mGy) and 229.0 ± 198.0 mGy.cm (range, 13.0–902.00 mGy.cm), respectively. CT dose estimates calculated by multiplying a DLP value and an appropriate conversion factor based on the International Commission on Radiological Protection (ICRP) Publication 103 (25) were 2.6 ± 2.6 mSv (range, 0.2–15.6 mSv). CTDIvol, DLP, and dose estimate values of three different CT scanners are described in Table 3.
Radiation dose values between CT scanners
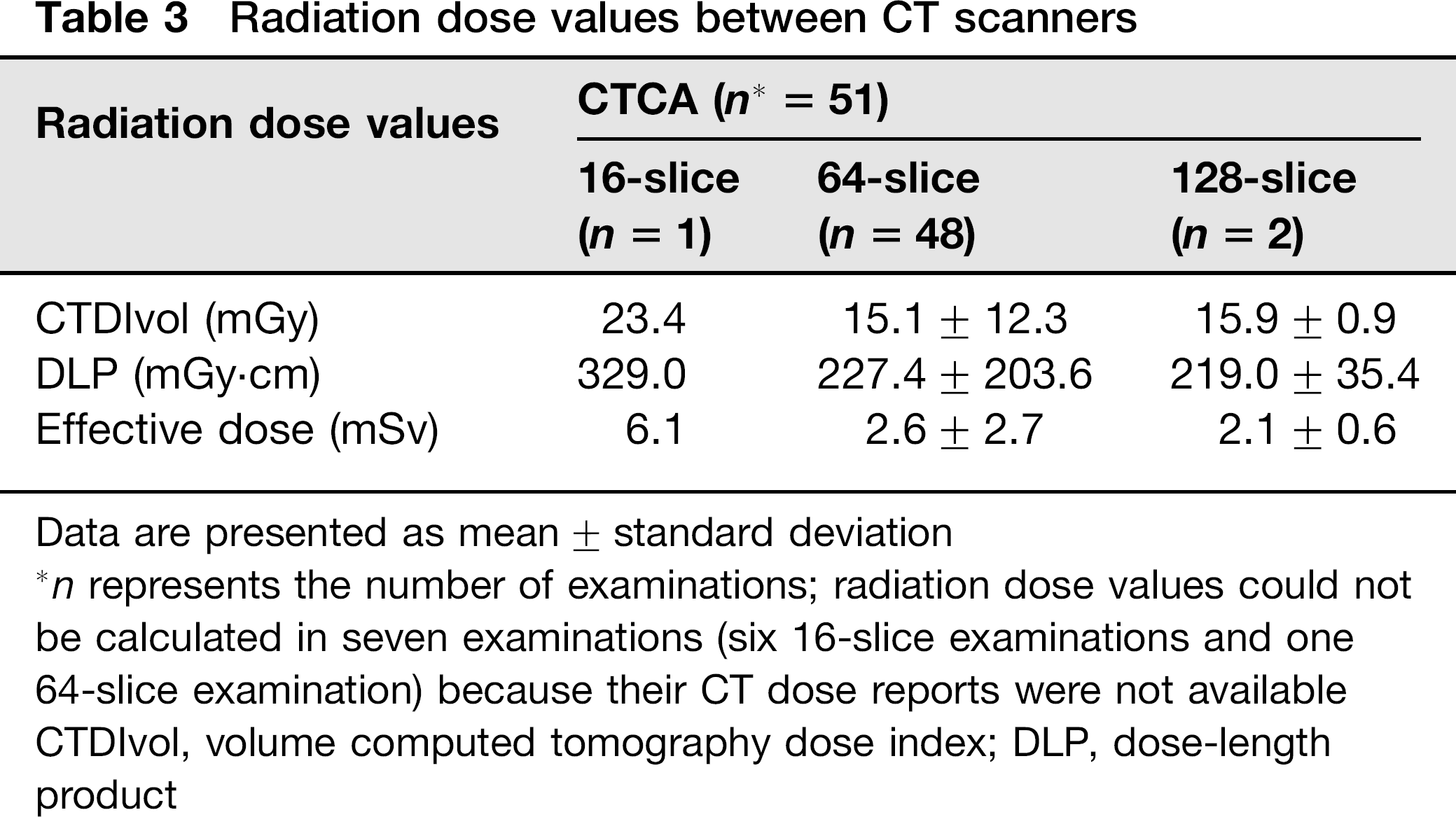
Data are presented as mean ± standard deviation
n represents the number of examinations; radiation dose values could not be calculated in seven examinations (six 16-slice examinations and one 64-slice examination) because their CT dose reports were not available CTDIvol, volume computed tomography dose index; DLP, dose-length product
Visibility of coronary artery segments
In group A, 540 (84.6%) of 638 segments were assessable on CTCA (n = 58) and 306 (71.3%) of 429 segments were assessable on MRCA (n = 39) (Table 4). In group B, 255 (89.2%) of 286 segments on CTCA (n = 26) and 212 (74.1%) of 286 segments on MRCA (n = 26) were assessable (Table 4).
Comparison of coronary artery visibility between CTCA and MRCA in groups A and B
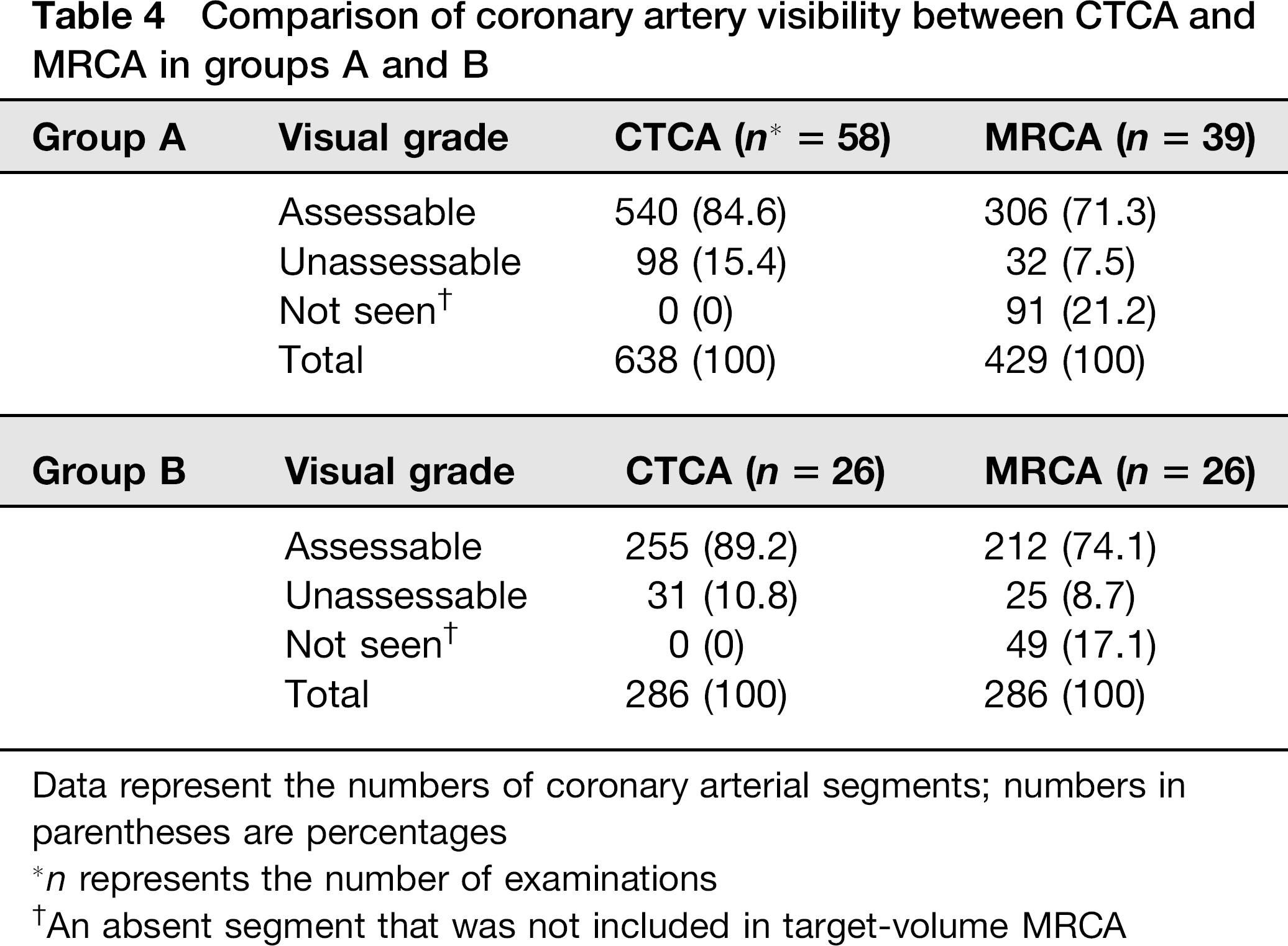
Data represent the numbers of coronary arterial segments; numbers in parentheses are percentages
n represents the number of examinations
An absent segment that was not included in target-volume MRCA
In the per-patient analysis in group B, no significant differences in coronary artery assessibility were observed between CTCA and MRCA (Table 5). Regarding the different CT scanners, the highest level of coronary artery assessibility was noted with the 128-slice scanner, followed by the 64-slice scanner and the 16-slice scanner (Table 6). In MRCA, the whole-heart approach (85.2%) yielded a higher number of assessable segments than the target-volume approach (67.7%) (Table 7).
Comparison of patient-based coronary artery visibility between CTCA and MRCA in group B after excluding absent
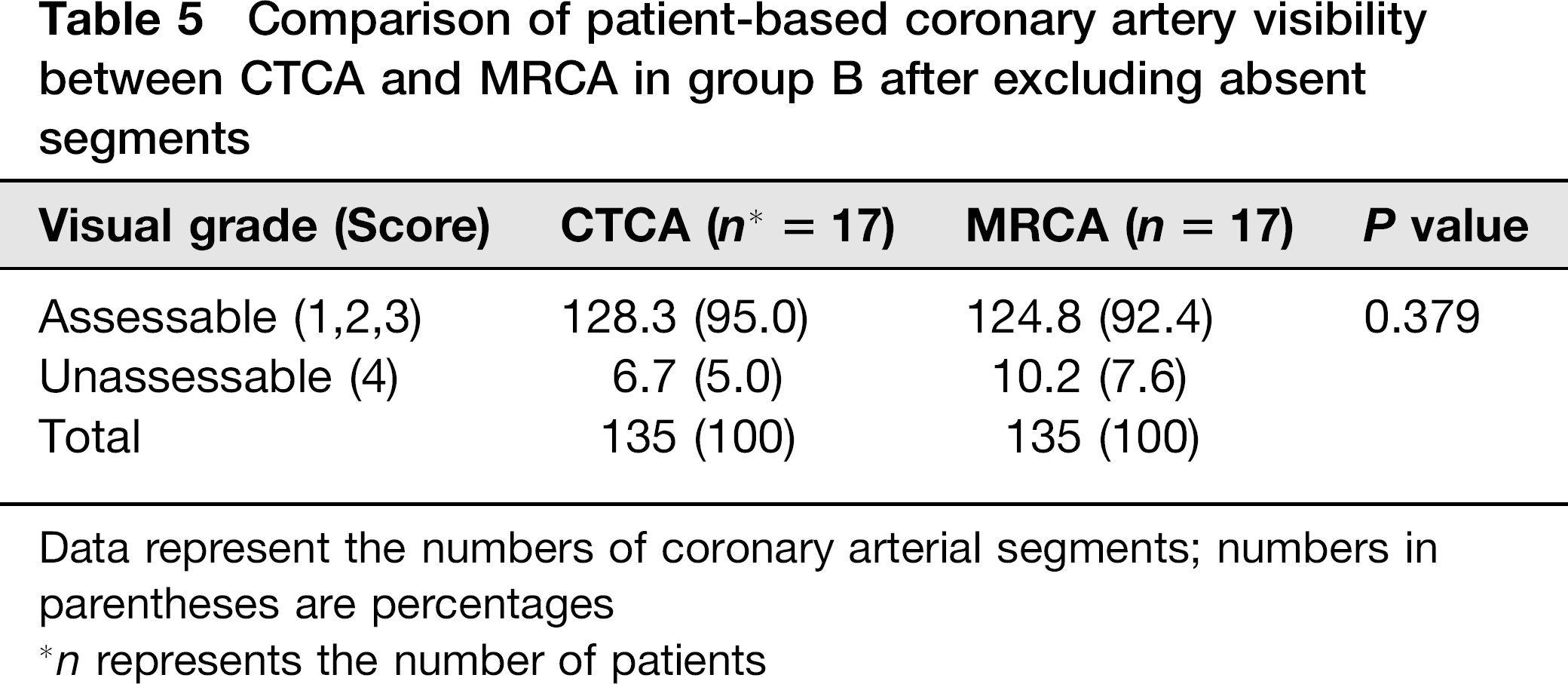
Data represent the numbers of coronary arterial segments; numbers in parentheses are percentages
n represents the number of patients
Comparison of coronary artery visibility between CT scanners

Data represent the numbers of coronary arterial segments; numbers in parentheses are percentages
n represents the number of examinations
Comparison of coronary artery visibility between target-volume and whole-heart MRCA approaches

Data represent the numbers of coronary arterial segments; numbers in parentheses are percentages
n represents the number of examinations
An absent segment that was not included in target-volume MRCA
Diagnostic performance for detecting coronary artery abnormalities
The number of aneurysms, stenosis, and occlusions was 76, 34, and 12, respectively, in group A, and 37, 14, and 4, respectively, in group B (Figs. 3–5). Out of a total of 76 aneurysms, 26 (34.2%) were giant. In group A, sensitivity, specificity, PPV, NPV, and accuracy of CTCA vs. MRCA were 93.1% vs. 77.9% (P> 0.001), 99.2% vs. 99.7% (P = 0.653), 96.8% vs. 98.7% (P = 0.652), 98.2% vs. 94.1% (P < 0.001), and 98.0% vs. 94.9% (P = 0.008), respectively. In group B, they were 91.8% vs. 70.4% (P < 0.001), 99.5% vs. 99.5% (P = 1.000), 98.5% vs. 98.0% (P = 1.000), 97.2% vs. 91.1% (P = 0.006), and 97.6% vs. 92.3% (P = 0.004), respectively (Table 8).
Diagnostic performance of CTCA and MRCA in groups A and B
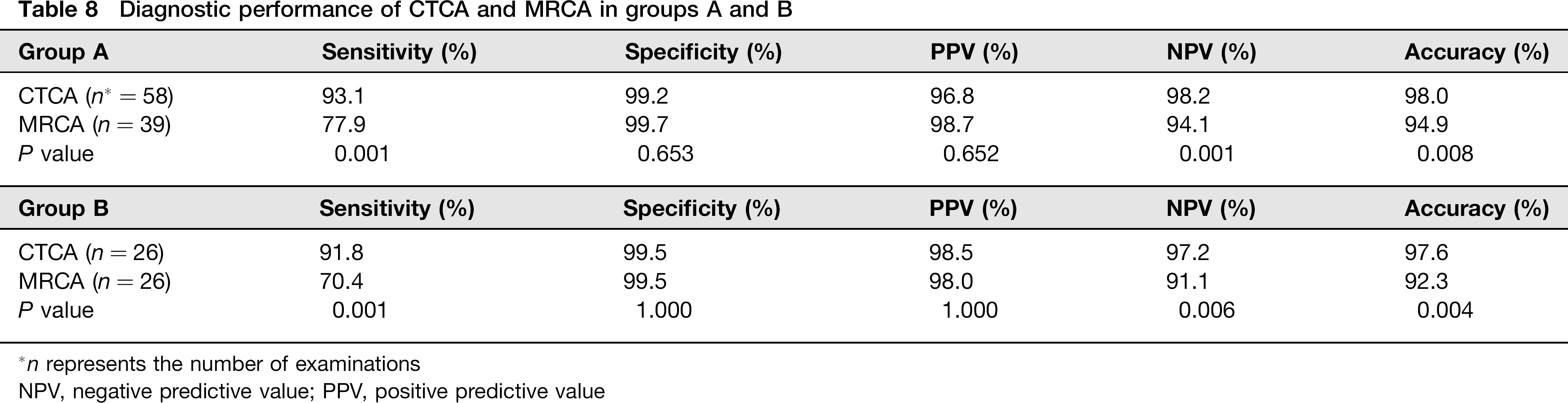
n represents the number of examinations
NPV, negative predictive value; PPV, positive predictive value
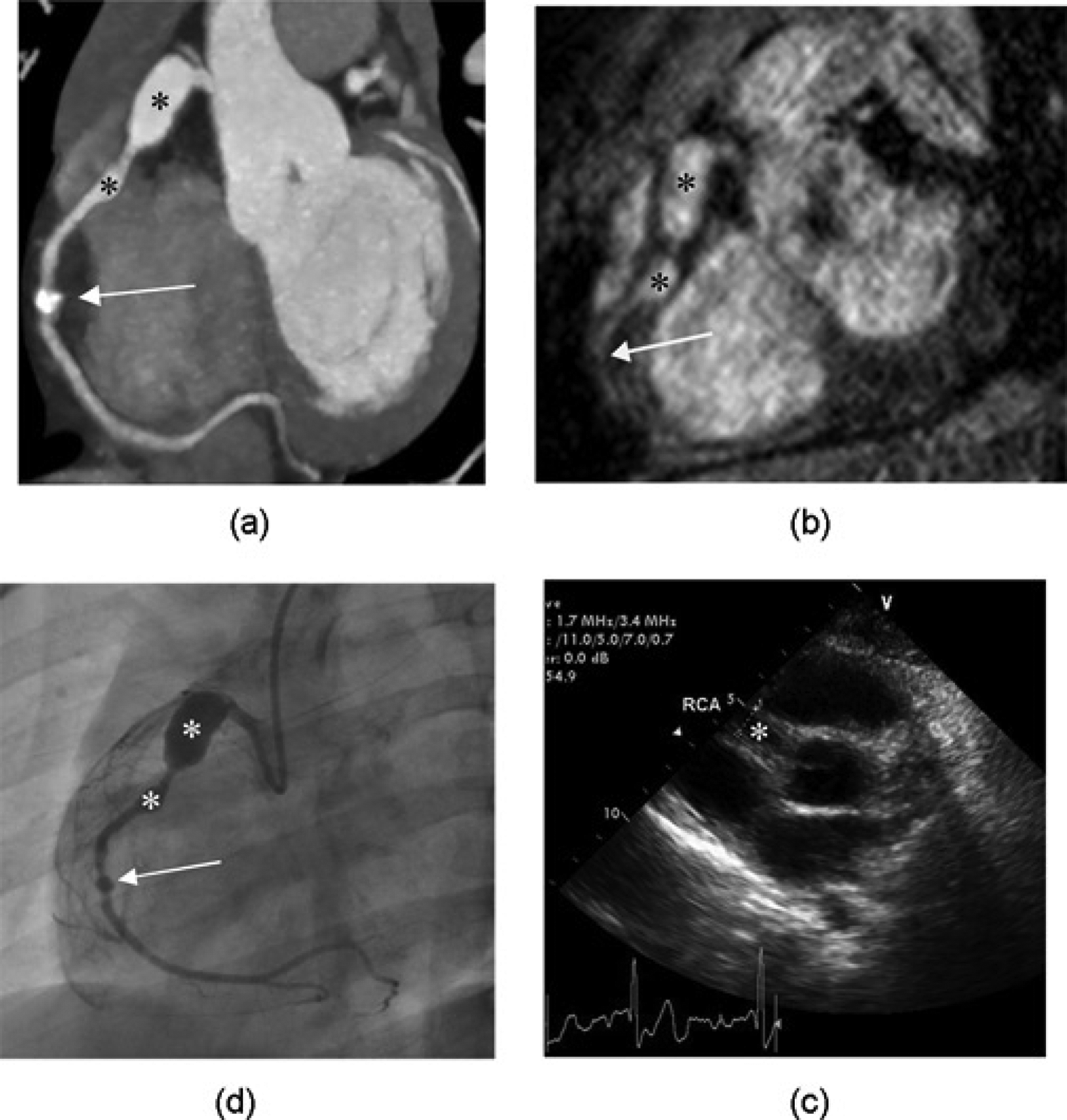
A boy with Kawasaki disease diagnosed at 4 years old. CTCA at 10 years old (a). MRCA with targeted-volume approach at 5 years old (b). CCA at 6 years old (c). ECHO at 4 years old (d). Three aneurysms are shown in the proximal and middle RCA on CTCA (a) and CCA (c) with a good agreement. However, the small calcified saccular aneurysm (arrow) in the middle RCA is not clearly seen on MRCA, in contrast to the first two aneurysms (asterisks) (b). In addition, the overall image quality of MRCA is worse than that of CTCA. ECHO is even worse (d); only the first aneurysm is identified
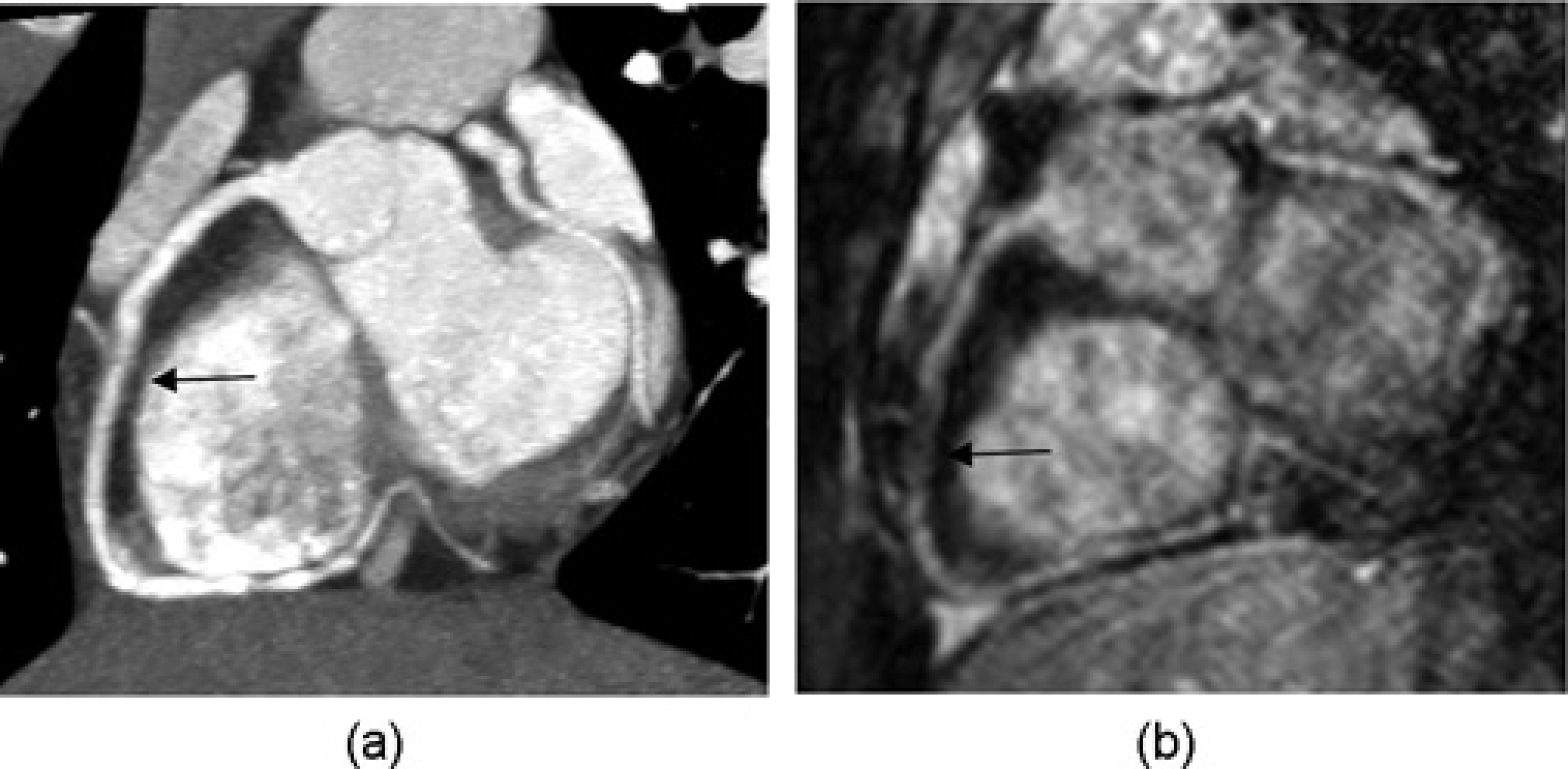
A boy with Kawasaki disease diagnosed at 2 years old. CTCA at 9 years old reveals a mild luminal narrowing (arrow) with myointimal thickening in the middle RCA (a). MRCA at 8 years old overestimates the luminal stenosis (arrow) (b)

A woman with Kawasaki disease diagnosed at 13 years old. CTCA at 22 years old shows heavily calcified aneurysms involving the proximal and middle RCA (a). The accurate assessment of luminal stenoses of the coronary artery aneurysms on CTCA is limited by blooming artifacts from severe intramural calcifications. By contrast, MRCA at 18 years old clearly demonstrates multiple stenoses (arrows) between the aneurysms (b), which is one of advantages of MRCA over CTCA
Discussion
In this study including a relatively large series of patients with Kawasaki disease, CTCA yielded more assessable coronary artery segments than MRCA in the per-segment analysis. This difference can be attributed to the substantial number of absent segments (accounting for 17.1–21.2% of the total coronary artery segments) on target-volume MRCA. MRCA using the target-volume technique has a limited coverage of the coronary artery system, especially the distal segments. In this study, the absent segments on target-volume MRCA (91 of 638 segments) mainly comprised the distal segments of the coronary arteries: the distal LAD artery (28 segments, 30.8%), the PDA (27 segments, 30%), and the distal LCx artery (25 segments, 27.5%). This observation is comparable with results from previous studies using target volume MRCA (26, 27).
The per-patient analysis, after excluding the absent segments in group B, also showed that coronary artery assessibility was comparable between CTCA and MRCA. Although there are a few studies directly comparing coronary artery visibility between CTCA and MRCA in adults, to the best of our knowledge, such studies have not been performed in children and adolescents. In adults, CTCA consistently shows higher coronary artery assessibility than MRCA (28, 29). The lower assessibility achieved with MRCA was attributed to lower spatial resolution, insufficient image quality, and a lower technical success rate. The discrepancy between the present study and these adult studies may be due to differences in the study populations, such as the size of the coronary arteries and heart rates.
We also found that CTCA showed higher sensitivity, NPV, and diagnostic accuracy than MRCA. In group B, MRCA identified one false-positive and eight false-negative segments with steno-occlusive lesions, whereas CTCA identified one false-positive and three false-negative segments. CTCA could not assess lumen patency accurately in three patients due to heavy calcifications, and it could not delineate the segment distal to the thrombosed aneurysm in one patient.
The lower diagnostic performance of MRCA is probably due to lower spatial resolution and poorer image quality. Other researchers (7, 8) reported a good agreement between MRCA and CCA in a small group of patients with Kawasaki disease having only aneurysms. In this regard, it should be underscored that a substantial number of steno-occlusive lesions in addition to aneurysms were included in this study. As a result, we believe that CTCA, with a higher diagnostic performance, may be the preferred imaging modality for Kawasaki patients with steno-occlusive coronary artery lesions. Similarly, Arnold et al. (13) reported that CTCA was more accurate than MRCA in detecting stenotic lesions in patients with Kawasaki disease, using CCA as a reference standard. Our results are also in agreement with a meta-analysis study in adults with atherosclerotic coronary artery disease (30).
CTCA and MRCA have been studied as useful non-invasive imaging tools in patients with Kawasaki disease. In clinical practice, we are forced to choose CTCA or MRCA as the best imaging modality; thus, the strengths and weaknesses of CTCA and MRCA should be kept in mind. Compared with CTCA, MRCA is limited by a longer scan time and a lower spatial resolution. The longer scan time of MRCA is likely to decrease its technical success rate, particularly in young children. Heavy intramural calcifications preclude the accurate assessment of coronary artery stenosis using CTCA due to the so-called “blooming artifact” (31, 32). In this study, three of eight patients with heavy calcifications underwent MRCA, providing a better assessment of lumen patency (Fig. 5). Therefore, MRCA may be the preferred method for assessing coronary artery abnormalities in patients with Kawasaki disease if heavy calcifications are present. MRCA provides the comprehensive evaluation of myocardial perfusion and viability in patients with Kawasaki disease (33). In fact, we performed myocardial perfusion MRI and viability imaging in six MRCA studies that were not included in this analysis.
The radiation hazards of CTCA should be noted, particularly in a young population, and radiation dose of CTCA should be minimized if clinically indicated. To accomplish this, we used several dose-saving strategies, such as a body size-adapted protocol including low tube voltage techniques, attenuation-based and ECG-controlled tube current modulations, and prospectively ECG-triggered sequential scanning. As a result, CT dose parameters (CTDIvol, 15.3 ± 12.0 mGy; DLP, 229.0 ± 198.0 mGy.cm; effective dose, 2.6 ± 2.6 mSv) were lower than those of previous studies in patients with Kawasaki disease (11, 13). In a study using 16-slice retrospective ECG-gated CT, the CTDIvol and DLP were 36.1 ± 6.7 mGy and 404.6 ± 98.8 mGy.cm, respectively (11). In another study using 64-slice retrospective ECG-gated CT, the dose estimate was 12 ± 4.8 mSv (13). Notably, in this study, the CT dose estimates were considerably low, only 0.6 ± 0.5 mSV (range, 0.2–1.3 mSv) in five patients under the age of 2 years, who underwent prospective ECG-triggered sequential CT scanning. Although the radiation dose of CTCA can be reduced considerably, MRCA is still a viable non-invasive coronary artery imaging technique in children with Kawasaki disease who only have coronary artery aneurysms.
This study has several limitations. First, heterogeneous imaging techniques might affect the comparison between CTCA and MRCA. However, this is inevitable when considering that only a small subset of patients with Kawasaki disease need CTCA or MRCA and the follow-up intervals are usually long. In fact, the mean inter-study interval in this study was 29.6 months and that was 32.6 months in a previous study (4). Given the rapid recent technical developments of CTCA and MRCA, it would be difficult to use the same imaging protocols for a long-period retrospective study in patients with Kawasaki disease. Second, CCA was not performed in all patients due to the invasive nature of the technique. Therefore, our reference standard was based on a combination of ECHO, CTCA, MRCA, CCA, and clinical history. Third, the age of the patients at CTCA was significantly higher than that at MRCA, and the heart rate at CTCA was considerably slower than that at MRCA (Table 1). A possible explanation for this is that CTCA was mostly performed in older children who could hold their breath, while MRCA was largely performed in younger children who could not. These differences in age and heart rate might influence our results. Finally, nitroglycerin was not used for MRCA except one patient, because we were not sure of its effects during longer scan times. Typically, sublingual nitroglycerin (0.4 mg per dose) elicits a vasodilatory response within 2–5 min, with maximal effects at 3–15 min, and little residual activity by 20–30 min (34). Nonetheless, the sublingual administration of nitroglycerin induced a 25.35% ± 6.51 increase in coronary lumen diameter, accompanied by improved coronary artery visibility on whole-heart MRCA (35). Thus, the more frequent use of nitroglycerin for CTCA in this study might influence our results.
In 2004, the AHA guidelines for Kawasaki disease stratified patients into five risk levels depending on their relative risk of myocardial ischemia, translating into stratified patient management and surveillance (2). CTCA and MRCA were not included in the 2004 guidelines, but are anticipated to be included in future guidelines. This study supports the necessity of such an update in the guidelines for patients with Kawasaki disease.
In conclusion, although coronary artery assessibility is comparable between CTCA and MRCA in per-patient analysis, CTCA shows higher diagnostic performance than MRCA for evaluating coronary artery abnormalities in patients with Kawasaki disease.