
Abstract
Thymic tumors represent a broad spectrum of neoplastic disorders and pose considerable diagnostic difficulties. A non-invasive imaging study to determine the nature of thymic lesions can have significant impact on management of such tumors. 18F-flurorodeoxyglucose (18F-FDG) positron emission tomography-computed tomography (PET-CT) has shown promising results in characterization of thymic tumors. The objective of this article is to provide an illustrative tutorial highlighting the clinical utility of 18F-FDG PET-CT imaging in patients with thymic tumors. We have pictorially depicted the 18F-FDG PET-CT salient imaging characteristics of various thymic tumors, both epithelial and non-epithelial. Also discussed is the dynamic physiology of thymus gland which is to be kept in mind when evaluating thymic pathology on 18F-FDG PET-CT, as it can lead to interpretative pitfalls.
The thymus is a lymphatic organ that plays a vital role in the development and maturation of the immune system during childhood, specifically T cells (1). It predominantly develops from the thymic primordia arising from the third and fourth pharyngeal pouches, with lymphocytes migrating later on from liver during intrauterine development (2). It is a dynamic organ with great variation in size as well as location, in health and disease. Tumors of the thymus are uncommon. Epithelial thymic neoplasms account for approximately 50% of thymic tumors, while lymphomas (25%) and other tumors (e.g. teratoma) comprise the remainder (3). Preoperative radiological evaluation plays a major role in differentiation between various thymic tumors, but poses a considerable challenge to the radiologist. The morphological findings of thymic lesions have many degrees of overlap among different entities, and thymic tumors, mainly epithelial tumors, show a broad spectrum of biological and morphological features (4). 18F-flurorodeoxyglucose (18F-FDG) positron emission tomography-computed tomography (PET-CT) has gained widespread popularity in oncology imaging and being used for staging, restaging, response monitoring, and prognostication of various tumors (5). 18F-FDG PET-CT has also shown promising results in characterization of thymic tumors. 18F-FDG uptake in thymus can be normal physiological uptake or can represent thymic hyperplasia, primary thymic tumors, lymphomatous involvement, or metastasis. Correlation with findings from CT component of PET-CT might help in better characterization, by integrating metabolic information with anatomical details (6). Because of its anatomical and functional variability, thymus continues to be source of difficulty when interpreting 18F-FDG PET-CT. Familiarity with 18F-FDG PET-CT patterns of physiological and common pathological conditions of thymus is crucial for correct interpretation of such findings. Here we present a pictorial overview of 18F-FDG PET-CT findings in various physiological and pathological conditions affecting the thymus.
PET-CT imaging
PET-CT imaging combines anatomical information provided by CT with functional information provided by PET, in a single setting. The most common tracer used for PET-CT imaging of thymic tumors is 18F-FDG. Before 18F-FDG PET-CT, all patients fast for at least 4-6 h. Blood glucose levels are monitored and ideally should be <7.7 mmol/L. 18F-FDG (∼370 MBq-10 mCi for an adult) is then injected intravenously. The patients rest in a quiet room and after a 45-60-min uptake period, PET-CT is acquired. First, CT is acquired from skull base to mid thigh. This CT image is used for attenuation correction as well as anatomical localization. After CT acquisition, PET acquisition of the same axial range is started with the patient in the same position on table. After completion of PET acquisition, the reconstructed attenuation corrected PET images and CT images are fused and available for analysis. Intravenous contrast agent is not routinely administered for the CT part of PET-CT. Use of intravenous contrast might enhance the detection of vascular invasion by thymic tumors. Unfortunately, contrast enhancement might also introduce over correction artefacts and thereby reduce the reliability of standardized uptake value (SUV) (7). As SUV plays an important role in evaluation of thymic tumors, use of intravenous contrast is not currently recommended. Other PET tracers which have been evaluated and shown promising results for thymic neoplasms include 11C-Acetate and 11C-Choline, which image the lipid metabolism (8, 9).
Normal thymus
Despite the advances made in imaging technology and in understanding the dynamic physiology of the thymus, its variations in size and shape continue to be a source of misinterpretation. The size as well as 18F-FDG uptake of normal thymus varies with age and should be kept in mind when evaluating thymus on 18F-FDG PET-CT (10, 11) (Fig. 1). In the first two decades of life thymus is readily visible at CT in the perivascular space (10). It classically appears quadrilateral with convex borders in children <5 years, gradually becoming triangular with straight or concave borders as the age increases (10). 18F-FDG uptake in thymus is more commonly seen in younger age groups (12). It can persist well beyond puberty into late third decade of life (11). Positive association is seen between CT attenuation (Hounsfield unit [HU]) and 18F-FDG uptake, with uptake decreasing with age as the fatty infiltration of thymus increases (11). Additionally, ectopic thymic tissue may be found in the vicinity of the superior vena cava, brachiocephalic vessels, and aorta or rarely, in the posterior mediastinum. It could be mistaken for pathology on 18F-FDG PET-CT.
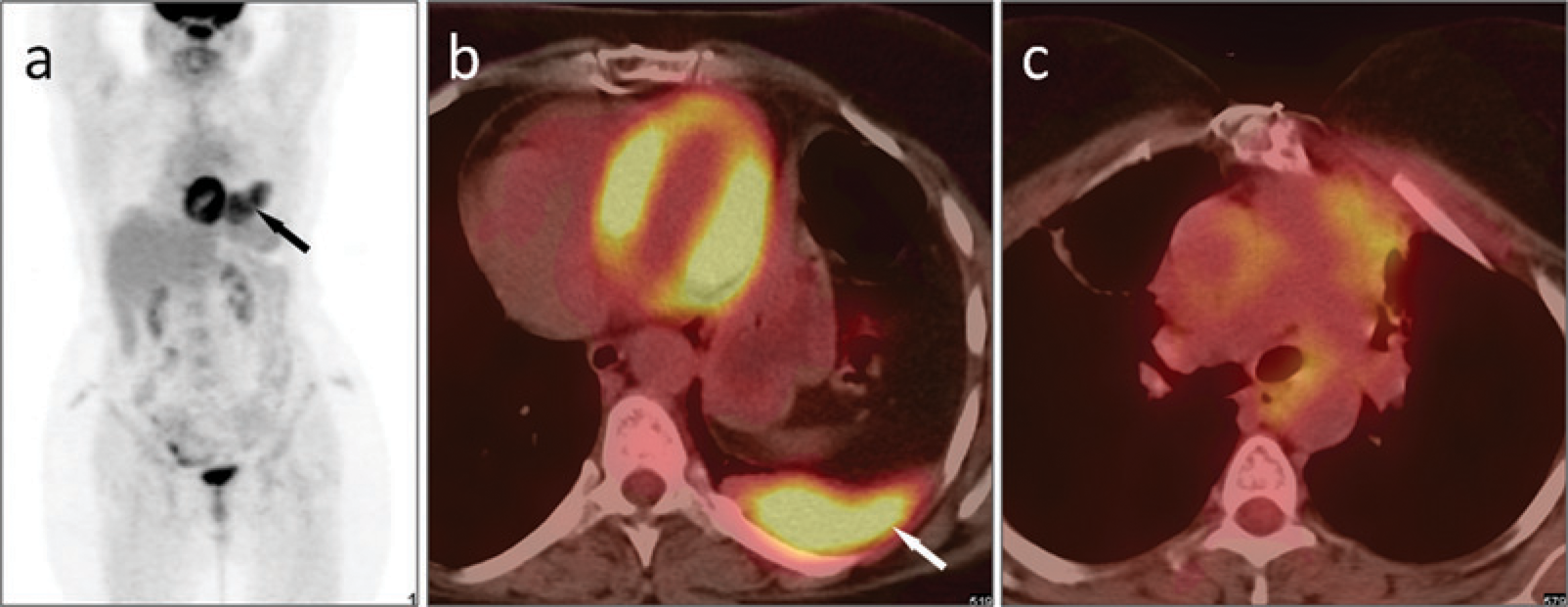
Impact of age on 18F-FDG PET-CT characteristics of thymus. 18F-FDG PET-CT images of a 5-year-old boy (a) with no history of any chemotherapy. Note the quadrangular shape of thymus with convex borders (arrow) showing soft tissue attenuation (56 HU) and increased 18F-FDG uptake (SUVmax 3.2). On the right is 18F-FDG PET-CT image of a 57-year-old man (b). The thymic tissue (arrow) has undergone fatty infiltration (−30 HU) with no significant 18F-FDG uptake (SUVmax 0.9). As the age increases the thymus is infiltrated with fat thereby reducing CT attenuation as well as 18F-FDG uptake
Thymic hyperplasia
Thymic hyperplasia is categorized into true thymic hyperplasia and lymphoid thymic hyperplasia. True thymic hyperplasia is characterized by increase in size and weight of the gland but with preservation of microscopic features (13). It is seen during recovery from a recent stress such as infection, chemotherapy, radiotherapy, steroid therapy, burns, et cetera, or less commonly associated with hyperthyroidism or pure red cell aplasia (14). Once the body recovers from the stress, thymus can increase to 50% larger than its original size, a phenomenon called “rebound hyperplasia”. Post-chemotherapy rebound hyperplasia is commonly seen in children but can be seen in adults. The differentiation of rebound hyperplasia form thymic a neoplasm is difficult even with 18F-FDG PET-CT. In cases of thymic hyperplasia the thymus usually losses its bilobed appearance and appears oval in CT. In one series the classic triangle or inverted V shape of thymic 18F-FDG uptake was observed in 60% of patients in that series, unilateral and focal midline uptake represented additional patterns of thymic uptake in 40% of patients (12). It has been suggested that standardized uptake value (SUVmax) may be useful in differentiating thymic rebound from mediastinal lymphoma, with a thymic SUVmax ≥3.4 being a strong predictor of lymphoma (15) (Fig. 2). In spite of overlap in SUVmax, it is helpful in differentiating rebound hyperplasia from thymic neoplasia (16). Lymphoid thymic hyperplasia is characterized by presence of lymphoid follicles with germinal centers and usually seen in association with immune disorders (myasthenia gravis, thyrotoxicosis, HIV infection). In Graves’ disease, thymic hyperplasia seems to be an effect rather than a cause of hyperthyroidism. Co-existing enlargements of the thyroid and thymus has been reported on 18F-FDG PET-CT in Graves’ disease (17). In most such cases, 18F-FDG uptake of the thymus was mild and diffuse.
A 13-year-old girl underwent follow up 18F-FDG PET-CT 4 months after completing chemotherapy for Hodgkin's lymphoma. (a) Maximum intensity projection (MIP) PET images show symmetrical wing shaped uptake in mediastinum (arrows). No other area of abnormal uptake was seen. (b) Non-contrast CT images of thorax reveal enlarged both lobes of thymus with smooth margins (arrows) and showing homogenous 18F-FDG uptake on fused PET-CT image (C, arrows), with a SUVmax of 3.1. A diagnosis of rebound thymic hyperplasia after chemotherapy was made on 18F-FDG PET-CT. The patient was kept on follow-up and doing fine at 3 years
Thymoma
Thymomas are benign or low grade malignant tumors. They are the most common anterior mediastinal primary neoplasms in adults and represent 20% of mediastinal neoplasms in this age group (13). Although usually asymptomatic, 20–30% patients may present with pressure symptoms, myasthenia gravis, pure red cell aplasia, or other immune disorders. As per World Health Organization (WHO) classification, thymomas are divided into two groups depending on whether the neoplastic epithelial cells and their nuclei have a spindle and/or oval shape (type A) or whether these cells have a dendritic or plump (epithelioid) appearance (type B) (18). Tumors that combine these two morphologies are designated type AB. Type B tumors are subdivided further into three subtypes designated B1, B2, and B3, respectively, on the basis of the proportional increase of the epithelial component and the emergence of atypia of the neoplastic cells. Although CT and MRI has been found to be useful in diagnosing thymoma, they have limited value in differentiating among the various WHO histologic subtypes and predicting prognosis (19, 20). 18F-FDG PET-CT has shown promising results in distinguishing different histological subtypes and help in preoperative characterization of thy-momas (Figs. 3–6). The cellular uptake of 18F-FDG in thymic epithelial cells is mediated by glucose transporter (GLUT). Kaira et al. recently reported that there is positive correlation between 18F-FDG uptake and GLUT1 expression in thymic epithelial tumors (21). Visual grading of uptake, SUVmax, pattern of uptake, and contour of tumor on PET-CT can be used for differentiation among histological subtypes (22). Sung et al. (23) reported that low-risk thymoma have a heterogeneous uptake when compared with high-risk thymoma and thymic carcinoma, which are more likely to have homogeneous uptake. Presence of encasement of mediastinal structures, pleural thickening, or effusion generally indicates invasive nature of the tumor (Fig. 7). SUVmax has been shown to be an important factor for differentiating among various histo-pathological subtypes of thymic tumors on 18F-FDG PET-CT (19, 22, 24-26). On the contrary, Shibata et al. reported that 18F-FDG PET-CT cannot differentiate among histopathological subtypes of thymoma (8). In addition, the SUV cut-offs given by these studies show considerable overlap. Multitude of factors might have accounted for these variations. These factors include smaller sample size, variation in acquisition/processing protocols, variability in size of tumors along with factors that influences SUVmax (serum glucose, body weight, injection time, etc). In spite of these variations it is generally agreed that invasive thymomas show higher 18F-FDG uptake (SUVmax) as compared to non-invasive thymomas (25). Calcification is often seen in thymomas. Up to 5% of patients with invasive thymomas can present with distant metastasis and 18F-FDG PET-CT being a whole-body imaging method is useful in detection of same. In patients with myasthenia gravis, differentiation between thymoma and thymic hyperplasia may be difficult on the basis of anatomic imaging alone. 18F-FDG PET has been found to be useful in differentiating these two entities by El-Bawab et al. (27). In their study, the mean value of SUVs in patients with thymoma was significantly higher than that in patients with thymic hyperplasia (4.75 and 1.89, respectively). 11C-Acetate PET has also been shown to be useful in differentiating the histopathological grades of thymoma based on SUV (8).
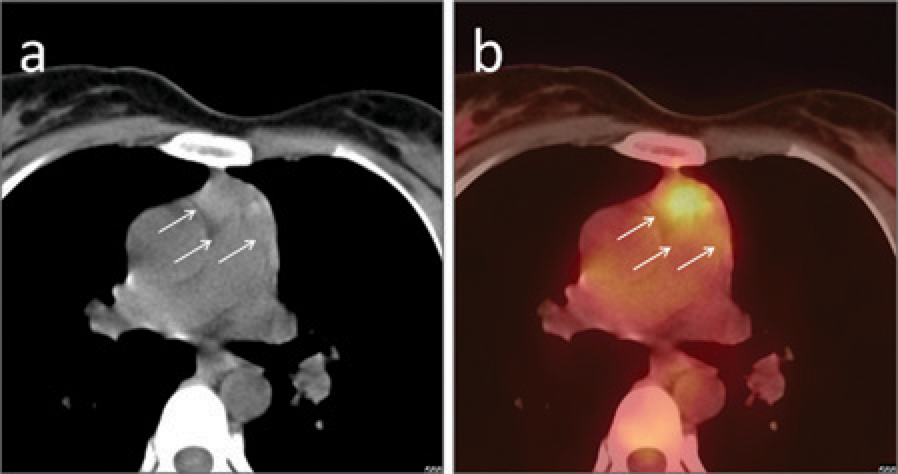
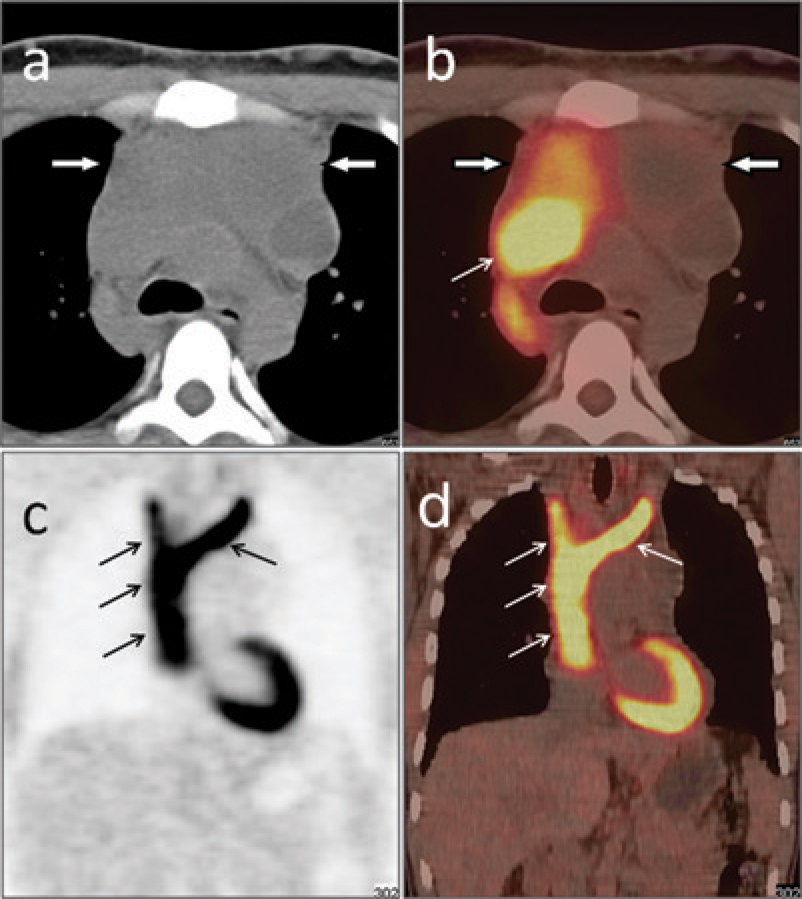
A 45-year-old female patient presented with myasthenia gravis. She underwent 18F-FDG PET-CT. (a) Non-contrast CT images revealed a 4 × 2.6 cm mass arising from the left thymic lobe (arrow) and abutting the left main pulmonary artery. No significant 18F-FDG uptake was seen in the mass on PET-CT images (b, arrow), with SUVmax of 1.9. A diagnosis of noninvasive thymoma was made on 18F-FDG PET-CT. Biopsy came out to be thymoma WHO subtype A A 25-year-old female patient presented with myasthenia gravis and an anterior mediastinal mass suspicious for thymoma. Preoperative 18F-FDG PET-CT was done. Non-contrast CT (a) of thorax showed an anterior mediastinal mass measuring 2.7 × 3.1 cm in size with fine calcification. The mass showed mildly increased 18F-FDG uptake on PET-CT (b) with SUVmax of 2.1. The fat planes between the mass and the great vessels was maintained (a, b, arrows). A diagnosis of non-invasive thymoma was made on 18F-FDG PET-CT. On histopathology the tumor came out to be thymoma, WHO subtype B1 A 75-year-old woman presented with pure red cell aplasia, secondary to a thymic tumor. 18F-FDG PET-CT was done for preoperative grading of the thymic tumor. Transaxial PET-CT images (a) showed a large anterior mediastinal mass measuring 10.3 × 12.7 cm in size and showing areas of calcification. Increased 18F-FDG uptake was seen in the mass (SUVmax 3.4). The fat planes between the mass and the pericardium were lost (b, arrow). A diagnosis of invasive thymoma was made on 18F-FDG PET-CT. Histopathology came out to be thymoma, WHO subtype B2 A 45-year-old male patient presented with myasthenia gravis. On further evaluation an anterior mediastinal mass was seen. The patient underwent 18F-FDG PET-CT. Maximum intensity projection (MIP) PET images (a) revealed a mediastinal focus of increased 18F-FDG uptake (arrow). Non-contrast CT image (b) showed an anterior mediastinal mass (arrow) measuring 3.8 × 4.1 cm in size. The fat plane between the mass and adjacent structures was maintained and findings were suggestive of non-invasive thymoma. However, on 18F-FDG PET-CT (c) the mass showed increased 18F-FDG uptake with SUVmax of 5.2. A diagnosis of invasive thymoma was made on 18F-FDG PET-CT. The final diagnosis histopathological diagnosis was thymoma, WHO subtype B2. Hence, while minimal invasion can be missed on CT, 18F-FDG uptake is a more reliable indicator of histological grade A 27-year-old male patient presented with progressively increasing facial puffiness and engorgement of neck and facial veins. Chest X-ray revealed an anterior mediastinal mass. He underwent preoperative 18F-FDG PET-CT. A large multilobulated anterior mediastinal mass (bold arrows) was seen on non-contrast CT (a) which showed areas of necrosis and heterogeneous 18F-FDG uptake on PET-CT (b), SUVmax 3.7. The mass was encasing the vessels and invading the superior vena cava (SVC) forming an 18F-FDG avid tumor thrombus (b–d, arrows) in the SVC and brachiocephalic veins. A diagnosis of invasive thymoma was made on 18F-FDG PET-CT. On histopathology the tumor was thymoma, WHO subtype B3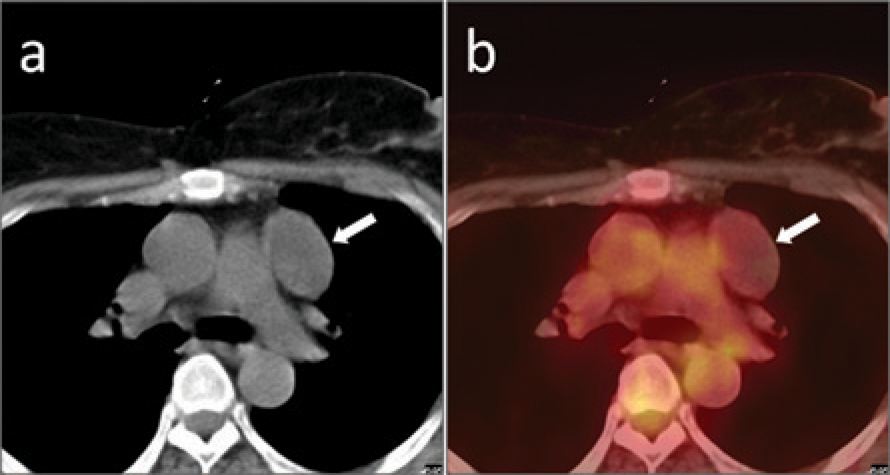


Thymic carcinoma
Thymic carcinomas are aggressive tumors with high tendency for distant metastasis and accounts for 20% of thymic epithelial tumors (13). They frequently cause pressure symptoms but rarely cause immunological paraneoplastic syndromes. On 18F-FDG PET-CT they usually present as large multilobulated masses with areas of necrosis and calcification and increased 18F-FDG uptake. SUVmax can be used to differentiate thymic carcinoma from thymoma, with the former usually having a SUVmax of ∼7 or more (22, 28). In addition, presence of mediastinal lymphadenopathy and distant metastasis on 18F-FDG PET-CT suggest thymic carcinoma (Fig. 8). Apart from its ability to differentiate between the various histological subtypes, 18F-FDG PET-CT can also detect residual or recurrent disease after treatment in patients with thymoma and thymic carcinoma (Fig. 9) and is superior to CT for this purpose (27). Because of its ability to detect metabolic changes it can distinguish post-therapy changes from residual/recurrent disease. Preliminary data suggest that 18F-FDG PET-CT is useful in monitoring and predicting response and outcome after treatment in unre-sectable thymic epithelial tumors. The metabolic response criteria based on 18F-FDG PET-CT seem to be more sensitive and accurate for response monitoring of such tumors (22).
A 56-year-old man presented with progressive respiratory difficulty and anterior mediastinal mass on chest X-ray. Fine needle aspiration cytology from the mass was inconclusive. He underwent 18F-FDG PET-CT imaging with a suspicion of primary thymic tumor. (a) Maximum intensity projection (MIP) PET images revealed a large area of irregular 18F-FDG uptake in the mediastinum. Transaxial PET-CT images (b) revealed a large mediastinal mass with areas of necrosis and 18F-FDG uptake in solid non-necrotic parts (SUVmax 8). The mass was invading the mediastinum and causing superior vena cava syndrome by encasing the SVC. Dilated collaterals (arrows) are seen in the chest wall. Also noted were 18F-FDG avid enlarged posterior mediastinal nodes (bold arrows) and left pleural effusion (asterix). Diagnosis of thymic carcinoma with nodal metastasis was made and confirmed at biopsy. The pleural effusion was also malignant on cytology A 50-year-old female patient underwent surgery followed by radiotherapy for a WHO subtype B3 thymoma. She presented 17 months later with cough and chest pain. The treating physician requested 18F-FDG PET-CT to rule out recurrent or metastatic disease. (a) Maximum intensity projection (MIP) PET images revealed a large focus of 18F-FDG uptake in the thorax (arrow). PET-CT images (b) revealed a large pleural based soft tissue mass in the left costophrenic angle (arrow) with increased 18F-FDG uptake (SUVmax 6.9). Apart from postoperative changes no other abnormality was noted at the primary site (c). A diagnosis of distant recurrence was made and confirmed on CT-guided biopsy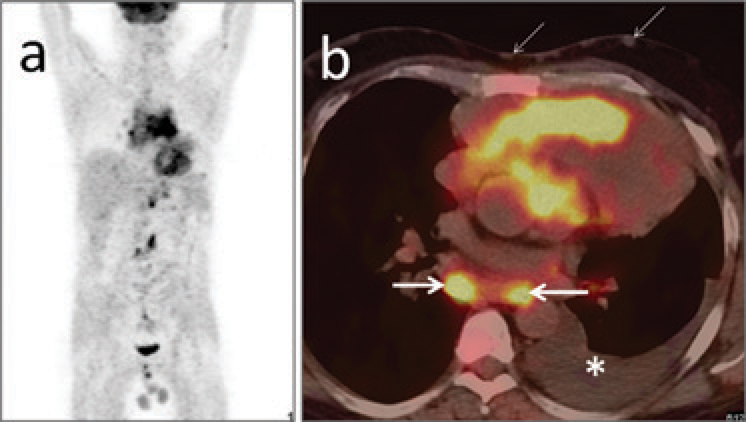
Lymphoma
Lymphoma is the most common cause of anterior mediastinal mass in children and second most common cause in adults. Thymic involvement in lymphoma can occur in the setting of widespread disease or as isolated involvement. It is more common in Hodgkin's lymphoma than Non-Hodgkin's lymphoma (14). When involved, the thymus is enlarged, sharply demarcated, occasionally enclosed within a thick capsule, and shows intense 18F-FDG uptake (Fig. 10). This 18F-FDG uptake is mainly dependent on the histopathological subtype of lymphoma (29). It can be difficult to differentiate thymic lymphomas from thymomas on 18F-FDG PET-CT, but the former tend to occur in younger populations, is more aggressive, and responds better to therapy. More problematic is distinguishing between rebound hyperplasia after chemotherapy and residual/recurrent lymphoma of thymus. SUVmax on 18F-FDG PET-CT has been shown to be useful in differentiating rebound hyperplasia from lymphoma involving the thymus (15). Nodular, asymmetrical enlargement of thymus with SUVmax ≥3.4 in a symptomatic child usually indicates lymphoma while symmetrical, smooth, non lobulated enlargement with SUVmax <3.4 in an asymptomatic child usually indicates rebound hyperplasia (15). However, overlap might occur and clinical data should be taken into consideration when making a diagnosis.
A 13-year-old girl with mediastinal Hodgkin's lymphoma. She underwent staging 18F-FDG PET-CT. Non-contrast CT images (a) showed a large anterior mediastinal mass, but the fat plane with the mediastinal structures is maintained. 18F-FDG PET-CT images (b) showed intense 18F-FDG uptake in the mass, with SUVmax of 15.6. A diagnosis of thymic lymphoma was made. After six cycles of chemotherapy she was in complete remission. A large anterior mediastinal mass with intense 18F-FDG uptake in a young patient generally favors lymphoma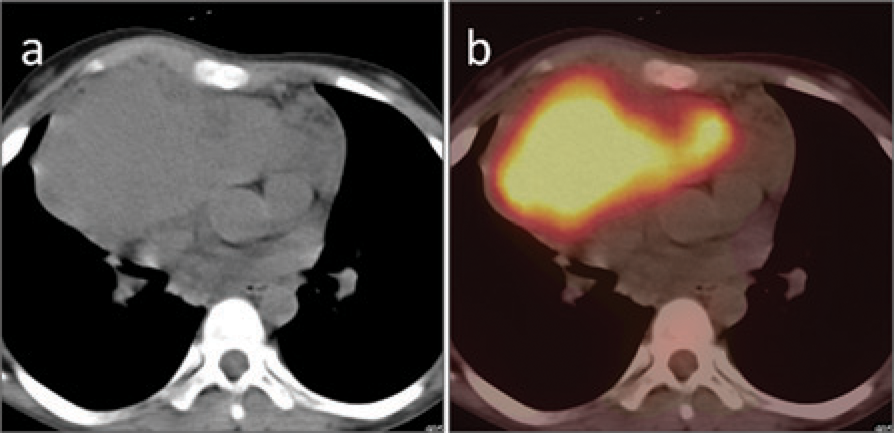
Thymic carcinoid
Thymic carcinoids are rare well differentiated neuro-endocrine tumors, more commonly seen in men. Patients can present with endocrine syndromes (Cushing's syndrome, multiple endocrine neoplasia). About 50% are invasive at time of diagnosis and frequently show hemorrhage and necrosis. In contrast to bronchial carcinoids which are usually not 18F-FDG avid, thymic carcinoids are usually 18F-FDG avid (30) (Fig. 11). 18F-FDG PET-CT can demonstrate the primary tumor, metastasis, or recurrent disease. Somatostatin receptor PET-CT with 68Ga-labelled peptides can be useful in selection of patients for peptide receptor radionuclide therapy in recurrent and metastatic cases, but is rarely positive (31).
A 32-year-old male patient presented with diarrhoea and flushing. Biochemical evaluation revealed elevated serum chromogranin A and urinary 5 hydroxyindoleacetic acid. Contrast-enhanced CT of thorax revealed a large enhancing anterior mediastinal mass, suspicious for thymic carcinoid (not shown). The patient underwent whole-body 18F-FDG PET-CT. (a) Non-contrast CT and PET-CT images (b) showed a large anterior mediastinal mass invading the mediastinum. Fat plane between the mass and great vessels was lost. The mass showed areas of necrosis (arrows) and 18F-FDG uptake in non-necrotic parts (SUVmax 2.3). In the given clinical scenario diagnosis of thymic carcinoid was made on 18F-FDG PET-CT and confirmed on biopsy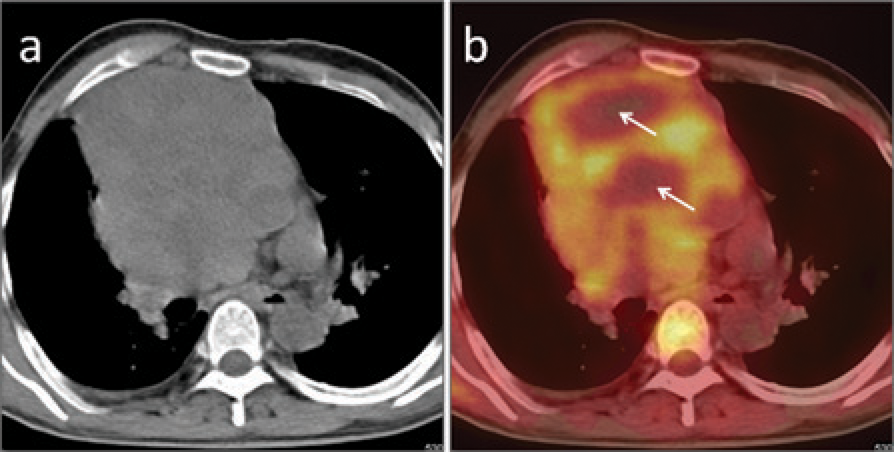
Miscellaneous tumors
Thymolipomas are rare, benign thymic neoplasms and usually present as asymptomatic large masses. CT appearance is diagnostic and shows large tumor connected to thymus with fatty attenuation, interspersed with fibrous septa and normal thymic tissue. 18F-FDG PET-CT has no additional role for such tumors. Anterior mediastinum is the commonest site for extragonadal germ cell tumors, which are usually benign, the commonest being teratoma (32). They usually present as large, round, lobulated masses with fat, fluid, calcification, bone, or teeth on PET-CT with variable 18F-FDG uptake, depending on grade of tumor (33). In addition 18F-FDG PET-CT can also be used for detecting recurrence and predicting survival for such tumors (34). Thymic sarcomas are rare aggressive neoplasms with poor outcome. They present as large heterogeneous masses on PET-CT with increased 18F-FDG uptake (33). Metastasis to thymus is rare and can occur in wide variety of tumors (lung, breast, head and neck, etc.). It can occur via lymphatic pathway or via the hematogeneous route. As for other metastatic tumors 18F-FDG PET-CT can demonstrate this rare site of metastasis (35).
Discussion
Thymic tumors represent a broad spectrum of neoplastic pathologies with variable overlap in clinical and imaging presentation. Conventional imaging with CT is useful but not sufficient alone for thymic oncologic imaging. This is mainly because of overlap between imaging appearances of thymic tumors, especially epithelial neoplasms (20). Various studies have shown that 18F-FDG PET is superior to CT for imaging thymic neoplasms (14, 16). A combination of PET and CT in the form of PET-CT is superior to either modality alone by combining anatomical and metabolic information (36). MRI, especially chemical shift MRI has also been found to be useful for differentiating thymic hyperplasia from thymic tumors (37).
The knowledge of the dynamic nature of thymus is essential when interpreting 18F-FDG PET-CT studies. There is change in shape, size, and 18F-FDG uptake of thymus with age and this should be kept in mind when evaluating PET-CT studies (12). In addition, thymic hyperplasia, especially rebound thymic hyperplasia, can mimic thymic malignancies and should be recognized. SUV on 18F-FDG PET-CT is useful in differentiating thymic hyperplasia from neoplasms, especially thymoma and lymphoma (15). One of the major utilities of 18F-FDG PET-CT is in preoperative histological classification of thymoma. This is based mainly on the level of 18F-FDG uptake, with increase in SUV seen with increasing grade (22). However, some degree of overlap is seen. CT features, when included in this algorithm improve the diagnostic accuracy. Apart from histological differentiation, 18F-FDG PET-CT can demonstrate metastasis, recurrence, and response to treatment in unresectable cases.
For other thymic tumors, the role of 18F-FDG PET-CT is less well-defined. 18F-FDG PET-CT can demonstrate and be used for response monitoring of thymic lymphoma and thymic metastasis (29, 35). Thymic carcinoids are generally 18F-FDG avid and PET-CT can be used to demonstrate invasion of adjacent structures, metastasis, and recurrence (30). Same is true for thymic sarcomas. Germ cell tumors on the other hand show variable 18F-FDG uptake depending of tumor grade. The main indication of 18F-FDG PET-CT for such tumors appears to be for detecting metastasis and recurrence (34). A brief overview of clinical findings and 18F-FDG PET-CT imaging findings for various thymic tumors is presented in the Table 1.
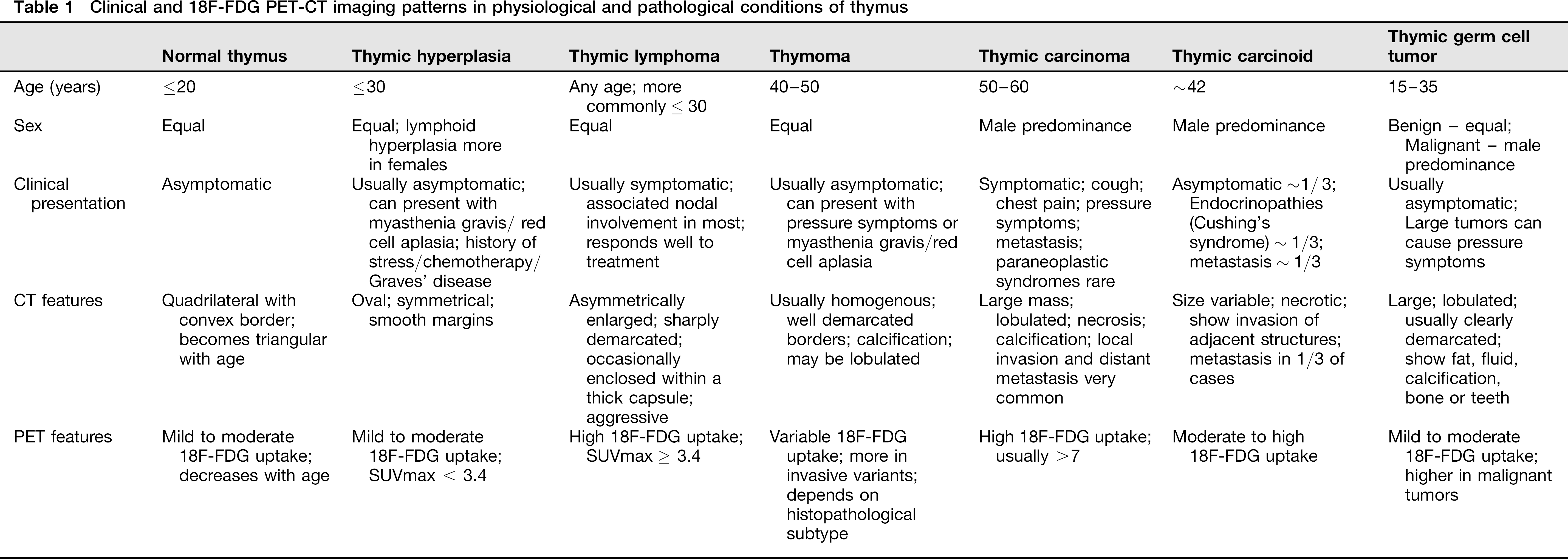
Clinical and 18F-FDG PET-CT imaging patterns in physiological and pathological conditions of thymus
In conclusion, 18F-FDG PET-CT is very helpful in imaging the various types of thymic tumors. Familiarity with thymic physiology and patterns of various thymic tumors is essential for correct interpretation of 18F-FDG PET-CT done for such tumors. The role of 18F-FDG PET-CT in comparison to newer MRI techniques like dynamic study with first gradient-echo 2D or 3D sequences, chemical shift images, and diffusion-weighted imaging needs to be evaluated. Additionally, recently introduced hybrid PET-MRI technology will combine them and further improve the imaging of thymic tumors.