
Abstract
Background
Both colon cancer and diverticular disease are common in the Western world. A challenge when patients present with clinical findings is that both diseases can present with symptoms that may mimic the other.
Purpose
To determine whether magnetic resonance imaging (MRI) could be helpful to differentiate between diverticulitis and cancer of the sigmoid colon compared to the differentiation offered by evaluation of multidetector computed tomography (CT) in a clinical situation.
Material and Methods
Thirty patients were consecutively included. Fifteen patients were under work-up for a recently diagnosed sigmoid cancer and 15 patients had recently been treated in hospital due to first-time acute sigmoid diverticulitis. All patients underwent CT, T2-weighted MRI and diffusion-weighted MRI. Anonymized examinations were retrospectively presented in random order to one experienced radiologist.
Results
With contrast-enhanced CT, the sensitivity and specificity for diagnosis of cancer and diverticulitis were 66.7% (10/15) and 93.3% (14/15), respectively. Using T2-weighted and diffusion-weighted MR images, the sensitivity and specificity for diagnosis of cancer and diverticulitis were 100% (14/14) and 100% (14/14), respectively.
Conclusion
MRI provides information that may contribute to improve the differentiation between sigmoid cancer and diverticulitis that is offered by CT. These encouraging results need to be confirmed in a larger study.
Keywords
Diverticular disease of the colon is common in the Western world, predominantly in the middle-aged and elderly population (1), annually 20–50 per 100,000 are admitted to hospital. Colon cancer is also a common disease, with an incidence of approximately 40 per 100,000/year in the United States, Australia, and Western Europe. The age group of patients affected by the diseases is similar (2).
When a patient presents with clinical findings consistent with acute diverticulitis, imaging is usually required to support the diagnosis and rule out other conditions with similar symptoms (3).
Today, the most widely used imaging modality for assessment of patients with suspected diverticulitis is computed tomography (CT). Historically, barium enema was the imaging technique of choice but has over the past decade been replaced by CT mainly because of its ability to visualize the entire colon independent of degree of stenosis, and to identify extra colonic extent of disease (4). A challenge when patients present with clinical symptoms and findings of diverticulitis is that colon cancer can present with symptoms that may mimic acute diverticulitis and vice versa. Furthermore, colon cancer may also develop in parts of the colon where there are diverticula that may obscure the presence of a tumor. If endoscopic biopsies are not conclusive or sometimes not obtainable and the patient is scheduled for follow-up investigations, the diagnosis and treatment may become delayed. An imaging modality that could differentiate cancer from diverticulitis in the sigmoid colon would therefore be of benefit to prevent delay, especially in cancer treatment.
Differentiation between diverticulitis and cancer is challenging because of considerable overlap in CT features (5, 6). Increased bowel wall thickness due to inflammation by diverticulitis may simulate thickening of the bowel wall caused by an annular cancer and vice versa. Free air, abscess formation, and specific target pattern of contrast enhancement on CT have all been proposed to support the diagnosis of diverticulitis but with low specificity (7) also locally advanced cancers can perforate.
A few studies have prospectively studied the value of MRI in diverticulitis using similar criteria for the diagnosis as on CT indicating that the diagnosis can be established without use of ionizing irradiation (8–10).
Diffusion-weighted MRI (DWI) is a technique where random microscopic motion of water protons contributes to image contrast (11). During the last few years, DWI has evolved as an important biomarker for evaluation of solid tumors. In a few observational studies, DWI has been described to be useful for diagnosis of colorectal cancer as well as for some inflammatory conditions in the abdomen (12, 13). Using DWI, tissue cellularity, organization, and volume of the extracellular space all contribute to the motion of water and thus to the signal intensity on DWI.
To the best of our knowledge, there is no previous study that retrospectively examined patients presenting with either left-sided diverticulitis with MRI including DWI or colon cancer in order to differentiate the conditions. The purpose of this pilot study was to compare CT and MRI with regard to differentiation between sigmoid cancer and diverticulitis. The study was approved by the local ethics committee of the Karolinska Institutet (KI 2008/474-31/4).
Material and Methods
Patients
An abdominal CT is often part of the work-up when a patient presents with abdominal symptoms that may be caused by either diverticulitis or sigmoid cancer. The pilot study prospectively included 30 consecutive patients after informed consent from May 2009 to September 2010. Half of these patients (of which six were women) were included because of a clinical diagnosis during a first-time admission for left-sided colonic diverticulitis confirmed by contrast-enhanced abdominal CT. This included pain in left or middle lower quadrant or local peritonitis, increased white blood cell count, C-reactive protein (CRP), and fever.
The other group of patients (of which nine were women) were under work-up for a newly diagnosed biopsy verified (during colonoscopy) as adenocarcinoma of the sigmoid colon patients without distant metastases on contrast-enhanced CT. To ensure that the cancer did not involve the rectum (>15 cm from the anal verge) all cancer patients underwent rigid recto-sigmoidoscopy. These patients were included when performing CT for metastasis staging.
The median age of patients with sigmoid cancer was 76 years (range, 57–82 years) and for patients with diverticulitis was 55 years (range, 39–75 years).
Patients with sigmoid cancer were then examined with MRI of the lower abdomen within a median of 10.7 days (range, 1–25 days) from CT. MRI of the lower abdomen in patients with diverticulitis was performed with the same imaging protocol as patients in sigmoid cancer group and with a median of 16.9 days (range, 1–43 days) from CT. All patients with sigmoid diverticulitis were subsequently examined with colonoscopy 4–6 weeks after the acute admission (reference standard) that confirmed the diagnosis of diverticular disease and ruled out colon cancer or polyps in the sigmoid colon.
Exclusion criteria were MRI contraindications, such as a cardiac pacemaker or metallic implants, pregnancy, claustrophobia or indication of emergency surgery, distant metastatic disease at presentation, and patients aged <18 years.
CT and MR examinations
MR examinations of the lower abdomen were performed on a 1.5 T System (SignaHDxt; GE Healthcare, Milwaukee, WI, USA) using a body phased array coil. The examination included T2-weighted fast spin-echo sequences in at least three planes, one plane perpendicular to the affected bowel segment (4140-12857/83- 107 ms TR/TE, voxel size 3-5 × 1.4-1.7 × 0.6-0.8 mm). Diffusion-weighted images were performed using transaxial free-breathing T2-weighted echo planar imaging sequence (10000/67 ms TR/TE) with b-values of 0 and 800 s/mm2.
CT examinations included the whole abdomen and were performed on one of two multidetector (4- and 16-row) scanners (LightSpeed, GE Healthcare, Milwaukee, WI, USA). The examinations were performed after oral and intravenous contrast administration. Images were reconstructed with 5 mm sections in a transaxial, sagittal, and coronal planes. The same protocol was used for both patient groups, as well in CT and MRI examinations.
Retrospective image evaluation
All MR and CT examinations were blinded to patients' clinical data and other clinical findings. The images were then retrospectively assessed visually exam by exam in random order by one experienced abdominal radiologist with 20 years of experience in abdominal CT and MR examinations (LB). The radiologist (LB) had not been involved in the initial evaluation of the CT or MRI examinations of patients included in the study.
First, the overall image quality was assessed. Presence of diverticular disease and/or presence of annular or exofytic tumor was documented if present. In case of diverticulae, stranding and possible complications such as fistulae, abscesses, or free air was further noted.
For MR examinations, a diagnosis was first established based on T2-weighted images. After evaluation of T2-weighted images, in addition evaluation of diffusion-weighted images was performed with the hypothesis that tumors would show decreased diffusion displayed as high signal intensity and that inflammatory process within diverticulitis would not show decreased diffusion compared to adjacent bowel loops (Fig. 1) (14).
A 64-year-old woman. Coronal and transaxial CT (a, b) and MR images (c–e). At blinded retrospective assessment of the CT examination, the diagnosis on CT was diverticulitis influenced by the presence of diverticular in the sigmoid colon. When independently assessing MR images, the tumor could be identified due to the difference in signal intensity between the propria muscle layer of the bowel and the lesion on coronal (c) and transaxial (d) T2-weighted images as well as focal increase in signal intensity on diffusion-weighted MR images with high b-value (e)
Results
MR investigations could not be evaluated in one of the 15 patients each in the cancer and in diverticulitis group due to reduced imaging quality caused by motion artifacts.
Among the sigmoid colon cancer patients (n = 15) all but one patient underwent left-sided hemicolectomy. One patient was not operated with resection due to concomitant disease including clinically locally advanced or metastatic colon cancer. The tumor stage according to histopathological analysis of the resected specimen was distributed according to Table1.
Baseline characteristics of patients with sigmoid cancer and diverticular disease
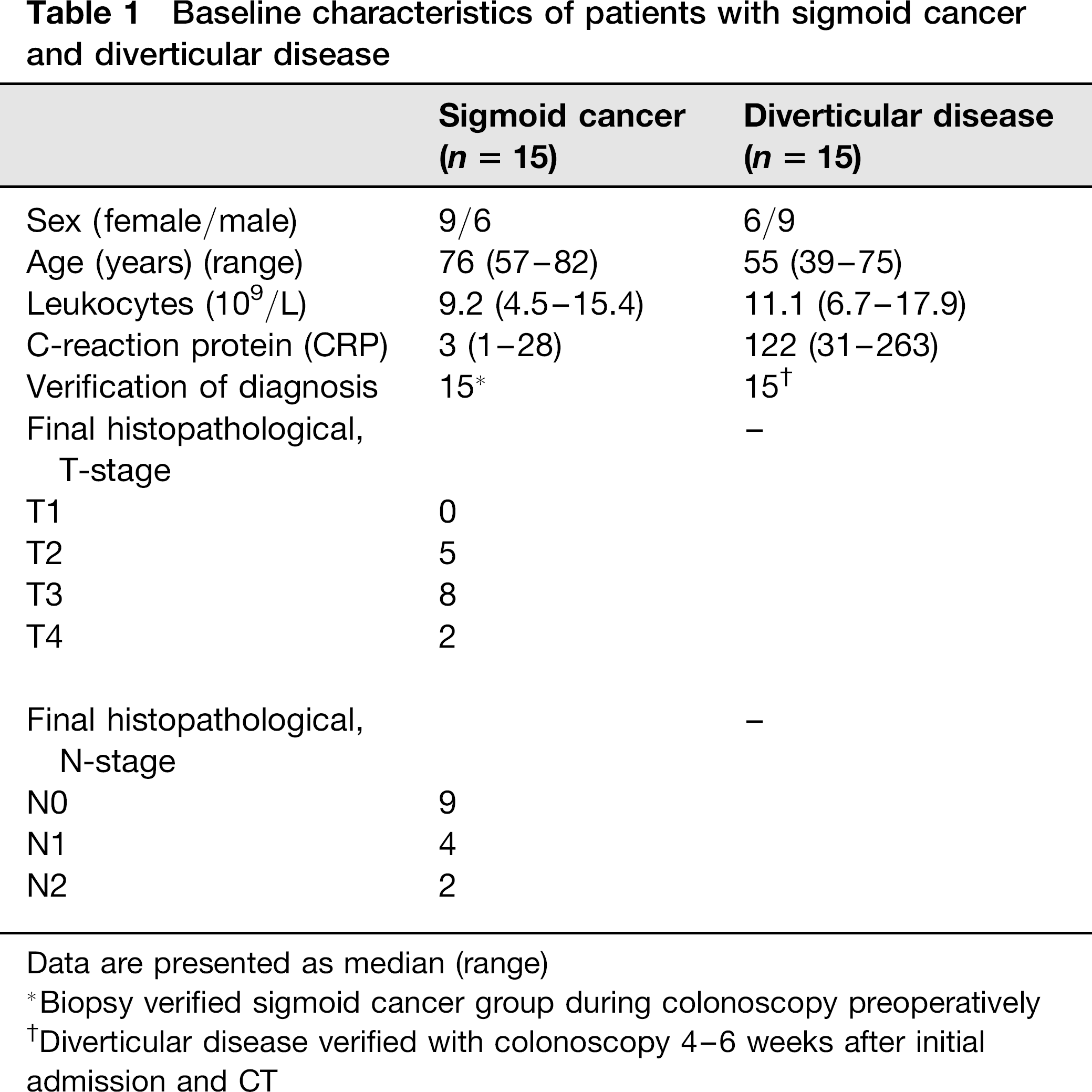
Data are presented as median (range)
Biopsy verified sigmoid cancer group during colonoscopy preoperatively
Diverticular disease verified with colonoscopy 4-6 weeks after initial admission and CT
In patients with sigmoid diverticulitis, none were primarily operated. Five were treated with fasting and antibiotics and 10 patients with fasting only according to a local treatment protocol.
According to evaluation of contrast-enhanced CT, a correct diagnosis of cancer was established in 10/15 patients. Five patients with cancer were diagnosed as diverticulitis, of which one patient had both diverticula and cancer in the colon. In patients with diverticulitis, one was diagnosed as having cancer of the sigmoid colon. The sensitivity for diagnosis of cancer on CT was 66.7% (10/15). The specificity of diverticulitis on CT was 93.3% (14/15).
Evaluation of T2-weighted and diffusion-weighted MR images, respectively, resulted in a correct diagnosis of cancer in 14/14 patients. In the diverticulitis group, the evaluation resulted in correct diagnosis in 14/14 patients. The sensitivity for diagnosis of cancer was 100% (14/14) and specificity for diverticulitis was 100% (14/14). The diagnosis was not changed with the addition DWI.
Discussion
Our results in this small study indicate a high sensitivity and specificity (100%) with MRI in the differentiation between diverticulitis and sigmoid cancer. The obtained results with CT resulted in a lower sensitivity and specificity for diagnosis of cancer and diverticulitis (66.7% and 93.3%).
Previously, CT perfusion measurements of the bowel wall have shown better discrimination of the entities than using morphologic criteria alone (15) but this technique is not generally used in clinical praxis and not used in our study.
Buckely et al. reported that it is easier to differentiate diverticulitis from cancer on MRI than CT due to the fact that MRI has excellent contrast resolution that allows a clear visualization of the thickened inflamed bowel and features typical for cancer as focal thickening with abrupt transition between normal colon and thickened colon. The advantage with MRI is the higher soft tissue contrast resolution enabling distinction of the muscularis propria layer of the colon from tumor and inflammation, particularly on T2-weighted sequences (16). This technique is routinely used for rectal cancer staging where the tumor typically has higher signal intensity than the propria muscle layer of the rectum and the outer border of the tumor and its relation to the mesorectal borders can be assessed (15, 17). It also provides functional capabilities such as diffusion-weighted imaging (8–10). The current study corroborates an earlier report on diverticulitis with MRI, where two blinded observers investigated a patient population of 55 patients with clinically suspected acute diverticulitis prospectively, the results showed sensitivities >94%, specificities of 88% (8). Other studies reported a sensitivity of 97% and specificity of 100% in a patient group with appendicitis (18).
Several reports have shown DWI as a possibility to identify neoplasms and a useful tool in detection of colorectal malignancy (13, 19). To our knowledge, there are no previous reports exploring the findings of DWI to sigmoid diverticulitis from cancer. Taken together, the present study showed no significant differences in the results between the MRI with or without and diffusion-weighted MRI. Larger studies are needed to investigate the value of DWI to differentiate diverticulitis from colon cancer. A challenging clinical problem is patients with chronic diverticulitis investigation with CT as well with colonoscopy may have difficulties to exclude colon cancer, and these patients therefore may even have to undergo colonic resection for final diagnosis. Therefore, MRI with the above results may facilitate the differential diagnosis being of considerable value in the daily clinical work.
The limitations of this study have to be mentioned. First of all, the radiologist that performed the retrospective evaluation of images was aware of that each group consisted of each 15 patients with the above mentioned diagnoses. When planning the study, our hypothesis was that restricted diffusion would appear in cancer and not in diverticulitis. Although we were not able to document this consecutively our impression was that restricted diffusion also was present to some extent in diverticulitis which has to be studied further to confirm and explore. Interestingly, decreased diffusion has previously also been shown in Crohn's ileitis (20) but to our knowledge not reported in sigmoid diverticulitis.
In this context, we were not able to make measurements of the apparent diffusion coefficient (ADC) values for cancer and diverticulitis which may have provided further information.
The MRI availability in our hospital also made the mean time between CT and MRI median 16 days (range, 1–43 days) which may also have affected the results in the analysis of the diverticulitis group. Some of the acute inflammation may have resolved during these 2.5 weeks between CT and MRI in this patient group, although there were still clear signs of the inflammation on the MRI images. Finally the sample size of the study is small, and our results should be confirmed and further explored in a larger study.
In conclusion, sigmoid diverticulitis can be diagnosed with CT although the differentiation from cancer is difficult in some patients. MRI using T2-weighted images provides information that may contribute to better differentiation between sigmoid diverticulitis and cancer.
Footnotes
Acknowledgements
This work was supported by Sigurd and Elsa Goljes foundation and the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County Council, and Karolinska Institutet.