
Abstract
Background
Self-expandable metallic stent placement is widely used to manage malignant gastroduodenal obstructions. However, there are difficulties in negotiating a guidewire (GW) and a stent delivery system (SDS).
Purpose
To investigate feasibility, usefulness, and safety of a guiding sheath for fluoroscopic stent placement in patients with malignant gastroduodenal obstructions.
Material and Methods
In July 2001 to August 2011, 726 patients with malignant gastroduodenal obstructions underwent stent placement. Guiding sheath was used in patients in whom a GW could not be passed through the obstruction and a SDS failed to reach the obstruction. Sheath usefulness was evaluated based on the ability of the sheath to successfully assist. The technical success rate and the most frequent reasons for the use of a sheath were evaluated.
Results
The guiding sheath was needed in 148 of 726 patients (20%). The overall technical success rate was 98% with the guiding sheath. In two of 148 patients, stent placement failed because, the GW could not be passed through the obstruction, in the other, the SDS could not be passed. A minority of patients reported mild discomfort. Patients with pancreatic cancer and duodenal obstruction were significantly more likely to require the use of guiding sheaths (P = 0.002, P < 0.001, respectively).
Conclusion
Using a guiding sheath for fluoroscopic stent placement appears to be feasible, useful and safe in patients with malignant gastroduodenal obstructions.
Keywords
Fluoroscopically guided peroral placement of gastroduodenal metallic stents is widely used to manage malignant gastroduodenal obstructions (1–3). Many authors have experienced difficulties in negotiating a guidewire (GW) and a stent delivery system (SDS) through strictures, especially due to GW buckling or the SDS forming a loop in the dilated stomach and gastroduodenal tract (3, 4). In order to facilitate GW and SDS introductions, the use of alternative methods such as the percutaneous approach and endoscopic guidance have been considered (5). Of these methods, endoscopy has often been referred in order to help movement of a GW through the working channel of the endoscope, eliminating the possibility that the GW becomes trapped in the gastroduodenal tract (6, 7). However, this method has some limitations, in particular the discomfort caused by the endoscopy and an inability of the currently available large diameter SDSs, which are designed for covered stents, to pass via the working channel (5, 8).
A previous study evaluated the efficacy with which two different types of specially designed guiding sheaths facilitate the placement of stents through gastroduodenal obstructions (7). However, further larger scale studies on the usefulness of the 60° J-shaped guiding sheath were lacking. Thus, the aim of this study was to retrospectively investigate the technical feasibility, clinical usefulness, and safety of a guiding sheath in fluoroscopic stent placement for patients with malignant gastroduodenal obstructions.
Material and Methods
Patient population
Informed consent was obtained from each patient and this retrospective cohort study was approved by our institutional review board. From July 2001 to August 2011, 726 consecutive patients with malignant gastroduodenal obstructions underwent fluoroscopic placement of a dual self-expandable metallic stent (S&G Biotech, Seongnam, Korea). The sites of obstruction were the stomach in 332 (46%) patients, the duodenum in 311 (43%) patients, and at anastomoses in 83 (11%) patients. The inclusion criteria for stent placement were as follows: (i) documented unresectable malignancy; (ii) obstruction of the stomach, the duodenum, or a surgical gastroenteric anastomotic site resulting in nausea, vomiting, and dysphagia; and (iii) patients whose life expectancy was >1 month. The exclusion criteria were: (i) mild symptomatic patients in whom an adult endoscope was capable of being passed through the malignant stricture; (ii) clinical evidence of perforation or peritonitis; and (iii) evidence of multiple small bowel obstructions. The characteristics of the patient population in this study are summarized in Table1.
Characteristics of the 726 consecutive patients in the study population

D1, first part of the duodenum; D2, second part of the duodenum; D3, third part of the duodenum; D4, fourth part of the duodenum
Guiding sheath construction
The guiding sheath used in this study was made from a polytetrafluoroethylene tube (Sang-A Flontec, Incheon, Korea). The tube was 5 and 6 mm (15 Fr and 18 Fr) in its inner and outer diameters, respectively, and its length ranged from 60 to 100 cm. The distal 3 cm of the sheath was curved in a J shape. This distal tip was positioned at an angle 608 to the axis in order to provide extra torque and the appropriate trajectory needed for a GW and an SDS to advance through gastroduodenal lumen (Fig. 1). A gold marker with a 12% polyurethane covering for surface smoothness was attached to the tip in order to facilitate easy detection during fluoroscopic guidance.
Photograph shows a type B guiding sheath, consisting of a polytetrafluoroethylene tube with a distal J-shaped tip. The distal 3 cm section of the sheath is positioned at an angle of 60° to the axis
Stent placement technique and usage of the guiding sheath
Dual-design expandable metallic stents (S&G Biotech, Seongnam, Korea), which consist of an outer partially covered stent and an inner bare nitinol stent, were used. The dual self-expandable metallic stent with its standard placement technique has previously been described in detail (9). Briefly, a hydrophilic exchange GW of 260 cm in length and 0.035 inch in diameter (Radifocus M; Terumo, Tokyo, Japan) was introduced with the help of a multifunctional coil catheter (Song-Lim catheter; S&G Biotech, Seongnam, Korea) through the mouth and across the obstruction into the duodenum or proximal jejunum to measure the length of the obstruction. The hydrophilic GW was then replaced with a super stiff GW (Medi-tech/ Boston Scientific, Watertown, MA, USA). After removing the coil catheter with the super stiff wire still left in place, a 3.8 mm (12 Fr) diameter SDS was passed over the super stiff GW through the obstruction in order to place the stent. The 60° J-shaped guiding sheath was inserted into the stomach to help a GW or an SDS pass through the gastric pyloric portion in cases where negotiation of a GW or an SDS through the obstruction failed due to GW/SDS buckling in the enlarged stomach (Figure 2).
Images obtained from a 57-year-old man with duodenal obstruction at the fourth portion of the duodenum caused by a pancreatic tail cancer. (a) Passage of an SDS through the obstruction failed due to loop formation (arrows and arrowheads). (b) Through the use of a guiding sheath (curved arrow), passage of the SDS through the stricture was successful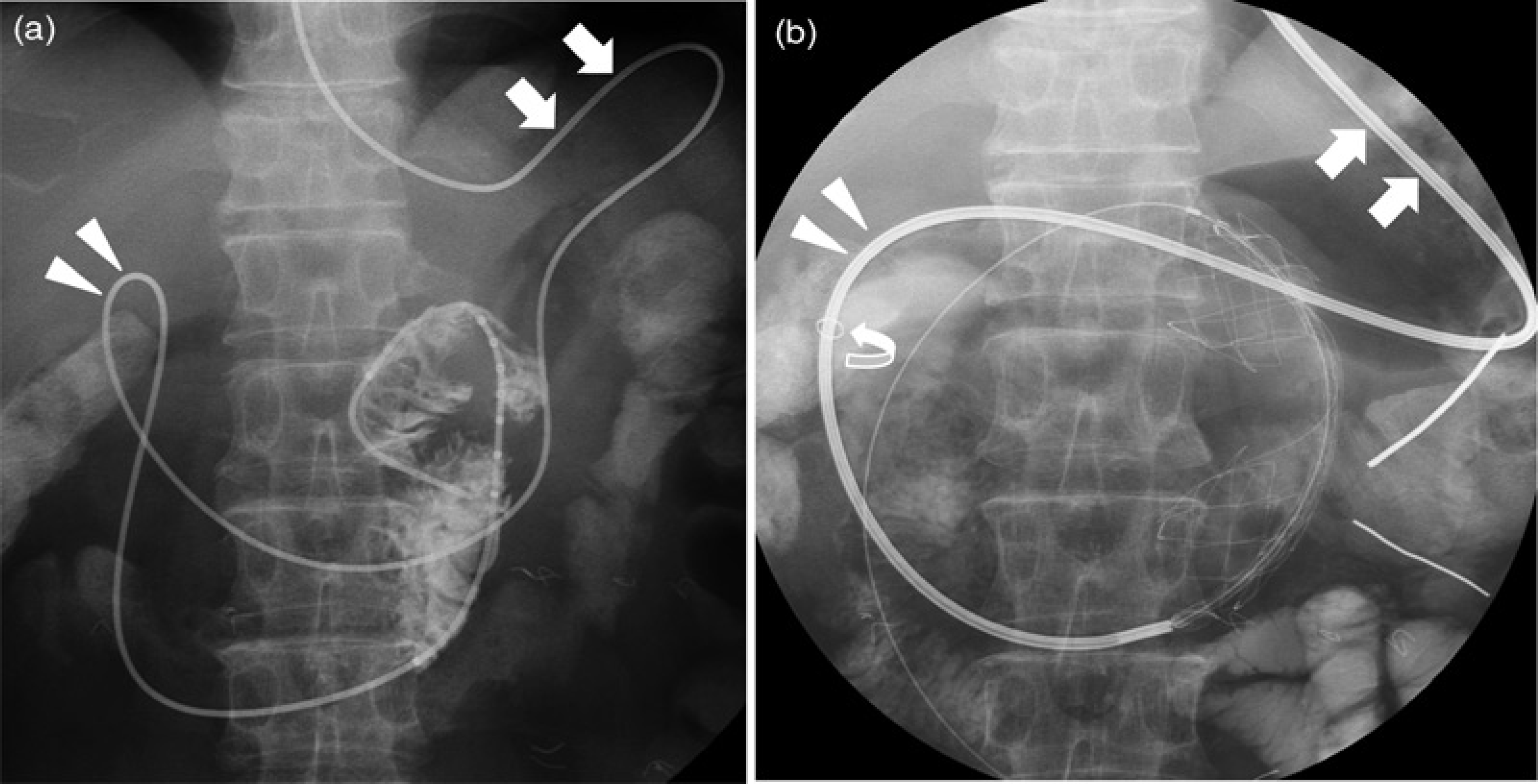
Definition and analysis of data
The technical success rates, the causes of technical failure, and procedure-related complications were analyzed. Technical success was defined as the successful negotiation of a GW and SDS.
The Fisher's exact test was used to evaluate the relationship between the use of guiding sheaths and the source of obstruction. We also evaluated the relationship between the use of guiding sheaths and location of obstruction. SPSS version 18.0 software (SPSS, Chicago, IL, USA) was used for all analyses. A two-sided P value of <0.05 was considered statistically significant.
Results
Usage of the guiding sheath
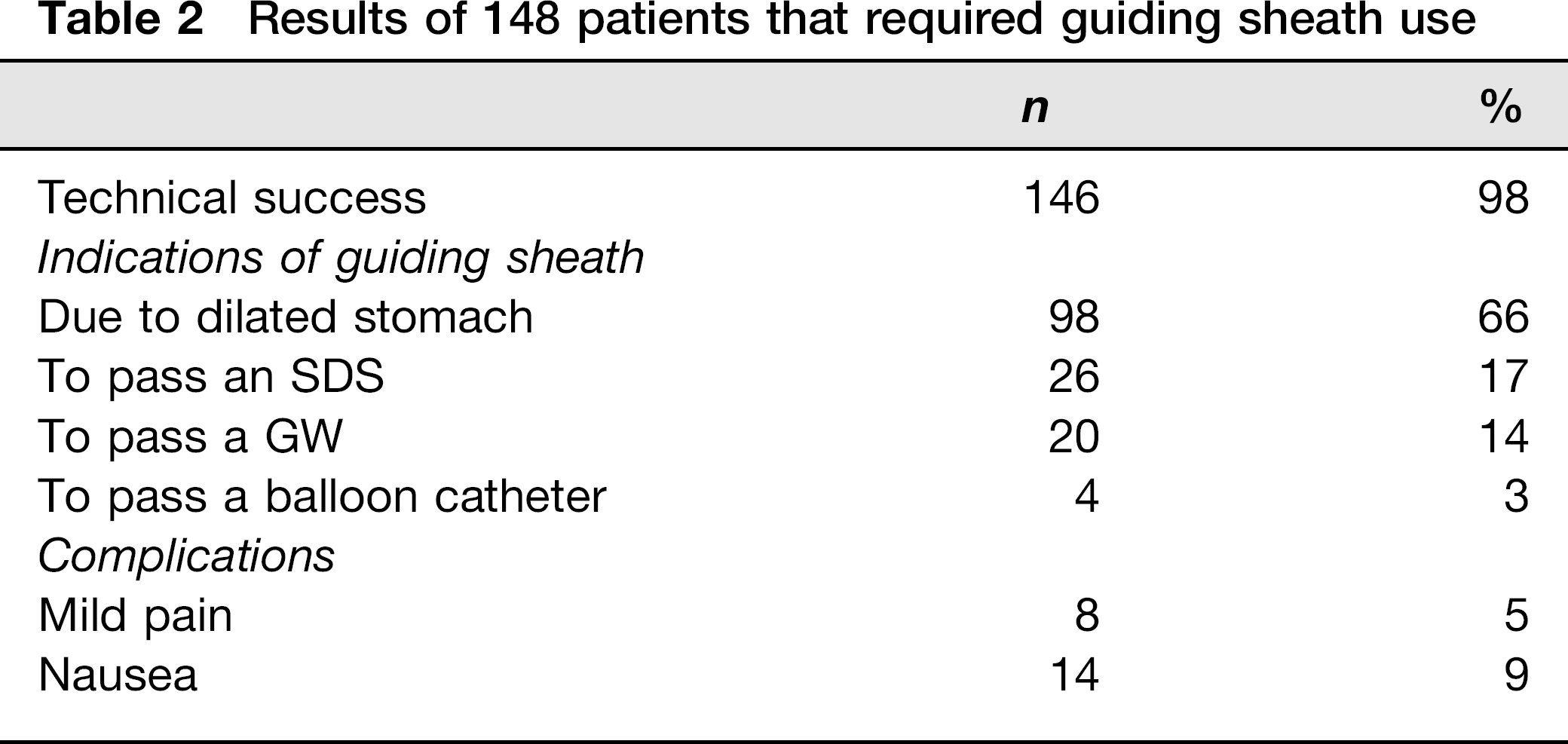
The guiding sheath was required in 148 of 726 patients (20%). The technical success rate was 98% (146/148) with the guiding sheath. With regard to the remaining two patients, the GW could not pass through the tight stricture in the fourth part of the duodenum in one patient while in the other patient, although it was possible to deploy the first graft stent into the stricture in the third part of the duodenum, deployment of the second bare stent was not possible. Endoscopic guidance was also used in the latter patient to resolve the problem but it was unsuccessful.
The reasons for using the guiding sheath were evaluated and four main reasons were identified, the most common, at 66%, being a dilated stomach (Table2). None of the 148 patients suffered major life-threatening sheath-related complications (such as bleeding and bowel perforation) during stent placement. A minority of patients reported mild discomfort (pain, 5% and nausea, 9%) during insertion of the sheath into the stomach.
Results of 148 patients that required guiding sheath use
Comparison between groups with and without use of guiding sheath
Patients with pancreatic cancer were significantly more likely to require the use of a guiding sheath than not (P = 0.002) (Table3). Conversely, patients with gastric cancer were significantly less likely to require guiding sheath use (P = 0.001). In addition, patients with duodenal obstruction were significantly more likely to require guiding sheath use (P < 0.001), especially, when the obstruction was found in the third part of the duodenum (P <0.001). In contrast, patients with gastric outlet obstruction were significantly less likely to need the use of a guiding sheath (P = 0.013). Moreover, patients with recurrent malignant obstructions at anastomosis sites such as the gastro-jejunostomy and gastroduodenostomy were significantly less likely to require the use of guiding sheaths (P = 0.020).
Usage of sheath with regard to location and source of obstruction
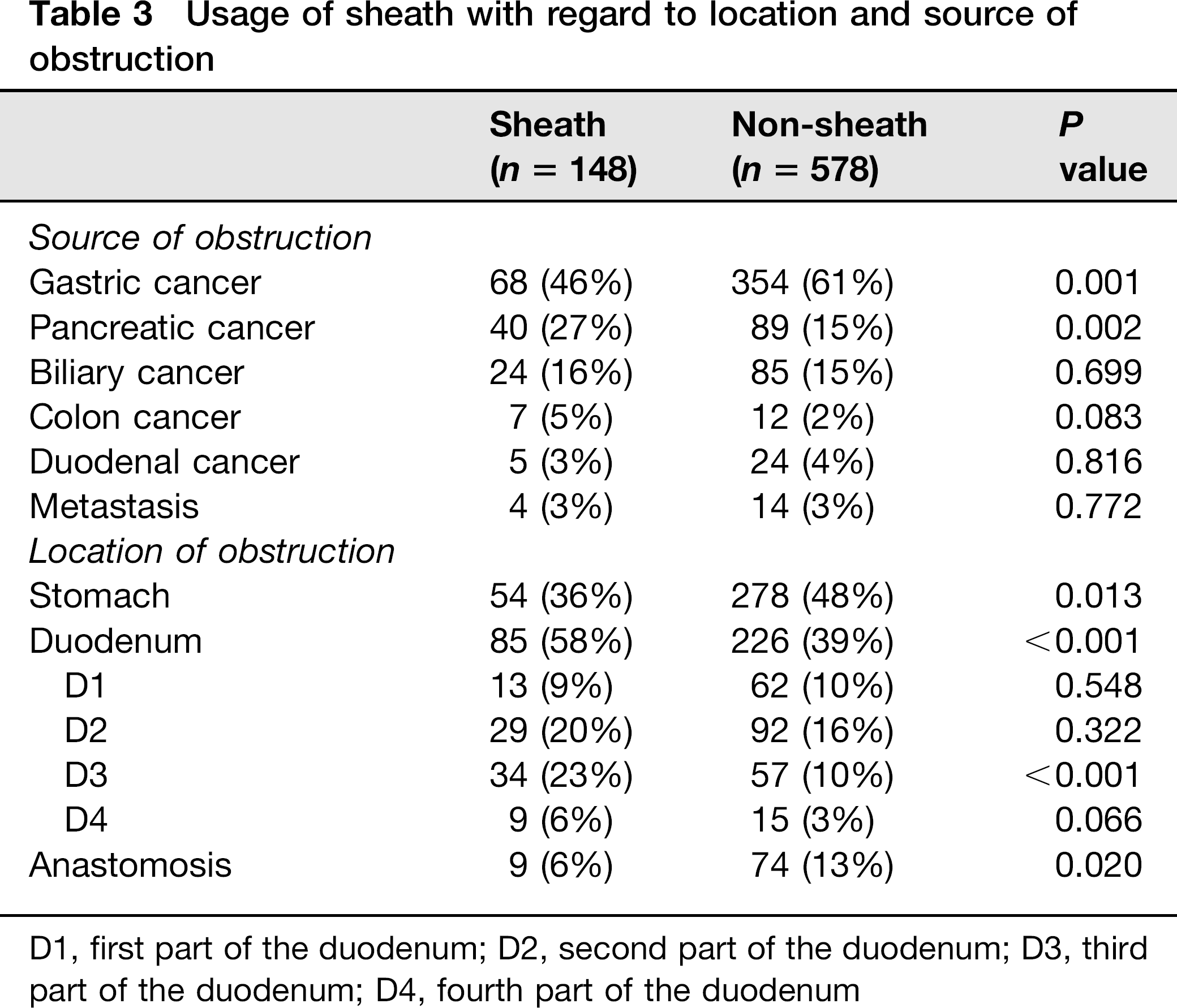
D1, first part of the duodenum; D2, second part of the duodenum; D3, third part of the duodenum; D4, fourth part of the duodenum
Discussion
In this study, the use of 60° J-shaped guiding sheaths in a relatively large patient population showed a high success rate (98%, 146 of 148 patients) in preventing GWs and SDSs from becoming trapped in the gastroduodenal tract during the deployment of gastroduodenal stents. The most frequent reason for using a 60° J-shaped guiding sheath was to overcome the angulated route from the stomach fundus to the gastric outlet during GW advance (65.5%, 98 of 148 patients). The guiding sheaths were most frequently applied for treating malignant obstructions due to pancreatic cancer and used as a supportive treatment option for patients whose strictures were located at duodenal portions. In other words, the longer from the mouth the duodenal strictures were, the more the guiding sheaths had to be adapted.
The guidance failure of GWs and SDSs due to an inability to pass through the gastric antrum and tight stricture has long been a major obstacle for the deployment of gastroduodenal metallic stents (3, 10). In order to prevent these problems, some guidance has been performed. Strecker et al. (11) used combined multiple GWs when tracking the stent through the strictures to overcome the angulated duodenal C-loop. Lee et al. (8) also used a 0.035-inch metal GW to prevent looping in the distended stomach. The use of those wires was not considered as an alternative in this study due to the increased risk of ulceration and minor bleeding in the gastroduodenal tract due to the wires being pushed hard against very tight strictures (12). Endoscopic assistance has also often been performed to overcome this technical problem during the procedure (5, 7).
In this study, the use of a 60° J-shaped guiding sheath was taken into consideration on the basis of the study by Bae et al. (7), which reported that the 60° J-shaped guiding sheaths improved the technical success rates of passing a GW and an SDS through a malignant gastroduodenal obstruction. The current study further confirmed the effectiveness of the 608 J-shaped guiding sheaths used by Bae et al. (7) but in a larger patient population (n = 148). There were some advantages in the use of the guiding sheath. First of all, the sheath could be introduced close to tight strictures at the third and forth duodenal portions without causing discomfort to most patients. The ability to pass a large-sized balloon catheter through the sheath is also one of the advantages in using the sheath. According to previous studies, an SDS with a large diameter for covered stents (>6 mm) cannot currently be passed through the working channel of endoscopes whose size are 4.2 mm (12 Fr) (8, 12). Even though the diameter of the SDSs in this study were 3.8 mm, the passage of a balloon catheter through the sheath means that if a similar J-shaped guiding sheath with a larger diameter were designed, it could easily facilitate the large-sized SDSs that are designed for other covered or newly designed stents.
The retrospective comparison between the groups of procedures with and without the use of the 60° J-shaped guiding sheaths suggests that the primary source of obstruction significantly affected the need for the guiding sheath. Compared to the non-sheath-aided patients, significantly more patients with pancreatic cancer needed the guiding sheath, while the reverse was true for gastric cancer patients. The difference in the preferences for guiding sheaths might be explained by the findings of Kim et al. (13), which revealed that more challenges were observed with stent placement in 60 patients with pancreatic malignant carcinoma than in 147 patients with gastric carcinoma. Similarly, in patients with pancreatic cancer, we often failed to pass GWs and SDSs using only a single GW through the distended stomach and the curved configuration of the duodenal C-loop. The 60° J-shaped guiding sheaths proved their effectiveness in the placement of stents at duodenal portions. In particular the long and tortuous path from the mouth to distant locations of the duodenum made it difficult to deliver the stent to the obstruction.
Reduced usage of guiding sheaths in fluoroscopic stent placement was shown for patients with recurrent malignant obstructions at anastomosis sites that were formed by reconstruction methods after surgical procedures. This may reflect the fact that most patients had their stomach resected partially or totally and then had new gastroduodenal routes constructed. This means that the passage from the mouth to the stricture was straighter and shorter than in other patients, which facilitated the easy passage of GWs and SDSs through the surgically altered gastroduodenal lumen to the stricture.
The principal limitation of this study is its retrospective design, but it is believed that these results will support the viability of future prospective investigations into developing guiding sheaths to aid GW and SDS passage through strictures.
In conclusion, in a larger population of patients, a 60° J-shaped guiding sheath was shown to be an effective technical modality for facilitating the introduction of a GW and an SDS through tight strictures when a GW buckles and an SDS loops in the gastroduodenal tract. Using a 60° J-shaped guiding sheath appears to be feasible, useful, and safe in fluoroscopic stent placement for patients with malignant gastroduodenal obstructions.