
Abstract
The aim of this study was to investigate patients' experiences of not being treated well in medical health care in Stockholm County, Sweden. The study was conducted by implementing qualitative content analysis using categorization of empirical material for 2006 and 2007 provided by the Patients' Advisory Committee (Patientnämnden) in Stockholm. Complaints about not being treated well accounted for 13% of all complaints to the Patients' Advisory Committee. A sample of those who complained about their medical treatment shows that about 30% of these complaints also involved experiences of being badly received. Categorization of the complaints about being badly treated resulted in the following 11 categories: (1) rude, aggressive or arrogant behaviour; (2) being ignored; (3) being denied examinations or treatments; (4) lack of empathy among personnel; (5) lack of respect for personal integrity; (6) lack of time/waiting time; (7) personnel not separating private issues from their professional role; (8) injustice and discrimination; (9) sexual harassment; (10) coercion and violence and (11) unspecified bad treatment. In relation to the total number of patients, women were over-represented in all categories. In conclusion, what patients react most strongly against is when health-care personnel treat them disrespectfully by not abiding by established social norms. The results indicate that the combination of failure in medical treatment and not receiving an apology often leads patients to complain to the Patients' Advisory Committee.
Background
The aim of curing entails a considerable risk of harming the patient, as has been long recognized in the tradition of medical treatment. As early as around 1800–1750 BC, in ancient Babylonia, the renowned Code of Hammurabi stipulated that both citizens and slaves were entitled to obtain medical care, but also that the treatment should be successful. 1 The famous biblical proverb ‘An eye for an eye…’ is also found in the Hammurabi Code, whereby the physician could be punished physically if the operation was not successful.
Although quite a lot has been said throughout the history of medicine about requirements for adequate behaviour by physicians vis-à-vis patients, it was not stressed until the 19th century that the primary aim for physicians should be not to harm the patient – primum non nocere. 2 During this period medicine became more dangerous because of the increasing number of surgical operations, quite a few of which went wrong. Since that time primum non nocere has become a widely acknowledged axiom.
Following the shift towards democratic priorities of individuality in politics and society and a client-based health care in the 20th century, there has been increasing focus on patient autonomy and individual rights. 3,4 Not only is it required by public health care that patients be offered proper medical treatment, patients also insist on being treated with respect and kindness. Accordingly, we might ask whether the primum non nocere axiom has been replaced by another one: first of all do not act disrespectfully towards the patient – primum non offendere.
Every year, about 14 million medical encounters between health-care professionals and patients take place in Stockholm County. 5 The majority of them pass off smoothly and to the satisfaction of everyone involved, but now and then patients are dissatisfied. Most problems and complaints are probably dealt with immediately by those concerned and are not reported at all. But some patients take their complaint further and report to the Swedish authorities. Since 1981, citizens of the County of Stockholm have been able to report dissatisfaction to the Patients' Advisory Committee (Patientnämnden) in Stockholm, which is an independent organization assigned to listen, help and protect patients' rights in both publicly and privately financed health care. About 70% of all complaints concern physicians, but nurses, midwives and dentists as well as wards and receptionists are also reported. 6,7
Two components are crucial for patients' wellbeing: correct diagnosis and medical treatments and good treatment by health-care personnel. Apart from being unpleasant and a sign of disrespect, bad treatment can lead to miscommunication, which might lead to patients not getting adequate care, whereas kind treatment can improve communication, increase patients' trust and make them more amenable to medical treatment. 8–13
Medical research has mainly focused on aspects of medical treatment and experiences of living with diseases, while much less attention has been paid to attitudes and behaviour towards patients and their potential consequences for wellbeing. A number of recent studies concern patient complaints about health-care personnel behaving unprofessionally or communicating poorly, but systematic research and analysis still remains scarce. 14–20 The report Equal complaints 21 has used Swedish Patients' Advisory Committee statistics to investigate sex-related differences in treatment of patients, and an anthropological paper discusses the management of Swedish patient complaints, 22 but no general studies focusing on bad behaviour towards patients have been made in Sweden.
The present empirical study was conducted to investigate patients' experiences of not being treated well in medical health care in Stockholm County.
Material and methods
Definition
The use of the term ‘treatment’ will here be restricted to the way patients are approached while in contact with health care, i.e. if the caregivers act in a friendly, empathic, attentive and caring way or if they are hostile, ignorant, patronizing or disrespectful. In this context ‘treatment’, then, should not be understood as medical treatment or other therapies (henceforth referred to as medical treatment).
Material and methods
Every year the Patients' Advisory Committee in the County of Stockholm receives approximately 4500–5000 complaints on different aspects of health care. 6,7 Until recently, the number of reported cases was steadily rising along with increased awareness of the existence of the Patients' Advisory Committee, 23 but during the past few years the number of complaints has remained stable. The most frequent complaints concerned consequences of medical treatment or the absence of medical treatment, but other topics were also reported, such as availability, information, administration and how individuals felt they were treated as a patient.
The complaints were lodged through emails, phone calls, letters and personal visits, and they were summarized and categorized by educated handling officers at the Patients' Advisory Committee. Normally, the complaints were registered in predefined categories, but in some cases the complaint was also given a supplementary registration when it contained more than one component of bad experiences. 6,7 The majority of these side complaints concerned how health-care personnel had behaved towards patients.
The study was conducted by implementing qualitative content analysis by categorization of empirical material provided by the Patients' Advisory Committee from 2006 and 2007. 24 Complaints about being wronged or badly treated represented the fourth commonest topic (preceded by [a] medical treatment, [b] counselling and [c] availability) and accounted for 13% of all complaints during the years 2006 and 2007 (2006: n = 659/5062; 2007: n = 589/4633). To examine this phenomenon, a systematic review of complaints concerning perceived bad treatment was carried out. The material was carefully worked through until potential categories were identified, tried and rejected, and a stable set of qualitatively distinct and substantial categories was established. The classification ‘medical treatment’ was also investigated to find out if any cases of bad treatment were prevalent also in that group, but they were not included in the analysis. Differences between men and women were taken into consideration. The Ethical Review Board in Stockholm approved the study.
Results
Categories of treatment complaints
Ten subordinate categories of complaints were found through our analysis among complaints categorized by the Patients' Advisory Committee under the label ‘treatment’. An additional category comprised complaints that had been reduced to such short summaries in the reports that no reliable conclusions about the art of bad treatment could be drawn. The complaints regarding treatment were categorized as shown in Table 1.
Categories of complaints about treatment to the Patients' Advisory Committee in Stockholm, Sweden, during 2006 and 2007
(1)
The most frequent objection about treatment was when the caregiver acted unprofessionally by behaving arrogantly, rudely or even aggressively. This complaint was, for instance, characterized by staff being sarcastic, verbally humiliating the patient or administering undeserved reprimands. The following quotes are examples from the Patients' Advisory Committee reports: ‘A 90-year-old woman complained about the way she was treated during an operation. The spleen was removed without forewarning. When the woman questioned this she was told: “At your age, what kind of life do you have to come home to anyway?’' ‘A man called his doctor to get a renewed prescription. He suffered from migraine and whiplash and had used the same medication for 20 years. He got to talk to a doctor who shouted at him and treated him like a drug abuser. He was denied a new prescription.’
Some patients had, for example, been accused of being fat, substance abusers, poor, uneducated or stupid. Some had experienced personnel getting angry, yelling and threatening them, or staff who had simply hung up on them in the middle of a conversation on the telephone.
(2)
The second most frequently reported topic concerned patients who reported physicians ignoring them, being unwilling to help, uninterested or not listening to their experiences. Some patients felt distrusted – as if the doctor thought that they were making up stories or were just whingeing. ‘Man, was calling about his partner who was depressed and did not have the strength to do anything at all. She turned to her family doctor but didn't get any help. The doctor was nonchalant, did not listen, and seemed to have no interest in helping her.’ ‘Woman, stated that she was not listened to when she presented her problems with a crown of a tooth. Eventually it had to be extracted but some problems remain.’
These complaints were often connected to dissatisfaction with medical treatment.
(3)
Patients also relatively frequently complained to the Patients' Advisory Committee about having been denied what they requested – a meeting, examination, medical treatment, referral or prescription. This phenomenon was often associated with complaints of unempathic and rude behaviour or not being listened to; this group was rather small yet featured frequently as a ‘by-category’ to other classifications. ‘Young woman (…) was refused treatment after questioning the medication. The doctor said that she ‘does not want to treat the patient since she obviously does not believe in it’ even though the patient had several times insisted that she wanted the treatment anyway.' ‘Older woman, sought acute care for chest pain. Examinations were carried out and at 00.30 the woman was asked to go home, and then return for operation at 09.00 in the morning. The woman was very ill during the night and during transportation from and to hospital. She wanted to know why she was not allowed to stay over at the hospital.’
(4–5)
Other complaints concerned lack of empathy for suffering patients and disrespect of personal integrity. Common examples were personnel perceived as insensitive or indifferent to the patient's needs and who ignored pain or dysfunctions, or weak patients who were sent home from hospital without being offered or helped to arrange adequate transportation. Patients also complained of insulting and offensive treatment, for example by having their naked bodies exposed, by having their diagnosis discussed in front of other patients or by feeling accused of being hypochondriac, being bad parents or leading ‘immoral lives’. ‘Woman, called the emergency duty repeatedly because of strong anxiety. The answering ward responded by saying “So what is it this time?” This conversation made the woman so sad that she took an overdose of her medicine.' ‘Woman with breast cancer, received a brochure about wigs by mail in a handwritten envelope from the county council. There were no other words or even a greeting. The woman felt offended.’ ‘Young man, felt very offended by a doctor who discussed his diagnoses in front of other patients. When the patient asked him to lower his voice, the doctor asked him to leave the ward.’
(6)
Another kind of complaint concerned waiting time and not being given enough time with the physician to discuss symptoms or a condition. Some patients were also denied information, examination or tests because of lack of time, and many complained about stressed doctors who would not take the time to listen to them even when they were scheduled. ‘Woman, who was unsatisfied with her visit to the health-care centre. When she wanted to ask more questions, the doctor told her she had to book a new appointment for that.’ ‘Woman, who reported that a doctor had blurted out that her cancer had spread to the liver and to the kidneys. The doctor then said that she was very stressed, did not have time to talk to the woman, and just told her to book an operation.’
(7)
This is a small but distinct category, containing examples of staff moaning to patients about their own situation, about workload or other personal problems, and thus behaving unprofessionally. ‘A woman had an appointment for prolonging her sick-leave (but) the doctor acted strangely and was talking about herself being worn out with hard work and about her private life. She yelled at the patient and projected her own problems on her (i.e. on the patient).’
(8)
Injustice and discrimination is another small category containing examples of patients experiencing that other patients with less acute symptoms at the emergency clinic were being prioritized. There were also situations where people had suffered discrimination due to sex, ethnic background, sexual preferences, physical or psychological dysfunctions, or age. ‘Man, sought help for somatic reasons. The doctor informed him, without examination, that he could not help him and referred him instead to psychiatry. The man felt insulted and that he was getting poorer treatment because he had a history of psychiatric illness.’ ‘Man, 67-year-old, had a car accident. He was then referred from orthopaedics to rehabilitation at the same hospital because of his whiplash injury. The man called the clinic to see when he would be treated but was told that they did not want to treat old-age pensioners.’
Age-discrimination accounted for a rather large proportion of the complaints and was in most cases reported by relatives of the aggrieved party.
(9–10)
A few cases of violence, threats, coercion and sexual harassment were also registered, for example experiences of being forced to eat, medicate or walk although in pain, or being denied help unless a certain treatment was accepted. Some patients reported violence in the shape of having experienced avoidable suffering, brutal handling by the assistant nurses, being pushed or being hit and a few cases concerned bad treatment in the final stage of life. A few examples of sexual harassment were also reported, and some patients reported physicians being unnecessarily intrusive during examination. ‘Man, was asked to perform a sexual favour for the doctor.’ ‘Mother of a 15-year-old girl called to complain about the behaviour of the GP. Her daughter had sought care for asthma and cold symptoms but instead was told that she was overweight. Moreover, the doctor touched her breasts to show her the location of the heart. The visit had demolished the girl's trust in health care.’ ‘Woman, was upset that she, while being treated at a psychiatric clinic, was not asked before the staff brutally pulled off her pants to see whether she was wearing a diaper.’
Bad treatment as a ‘by-category’
A random sample of remaining classifications in the Patients' Advisory Committee reports indicated that bad treatment seemed to occur more often than it was reported. A systematic review of the classification ‘medical treatment’ showed that more than a third of the complaints (2006: n = 511/1553; 2007: n = 413/1366) also concerned how the patients were received. Most commonly, they were denied certain forms of medical treatment in a rude or unpleasant way or were not listened to.
Women complained more frequently than men about being badly treated
Investigating the sex ratio, women were found to be in the majority as complainants in the reports to the Patients' Advisory Committee. In both 2006 and 2007, 63% of the complaints originated from women and 37% from men. In 2007, 14% of all women (n = 406) complaining to the Patients' Advisory Committee complained about not being well treated as against 10% of the men (n = 161) and in 2006 the balance of the sexes was 15% women (n = 473) versus 10% men (n = 185). 6,7 The gap between the sexes in patients experiencing bad treatment was found in all categories and in all areas of health care.
Discussion
Adequacy and relevance
The categories we identified turned out to constitute a stable basis for managing the large amount of material of reported complaints regarding treatment to the Patients' Advisory Committee in Stockholm in 2006 and 2007. They are also sufficiently distinct to facilitate categorization of new cases into existing categories and, furthermore, they cover all cases of bad treatment. We therefore believe our categorization to be both fruitful and relevant. However, the adequacy of a set of categories arrived at in qualitative research can always be questioned – how fine-grained the categories should be ultimately depends on their intended use.
When a complaint is reported to the Patients' Advisory Committee, it is generally classified and filed by an administrator as initially stated by the patient, regardless of whether there are also other aspects of the event that the patient might consider to be more important. Complaint interpretations made by the administrator which the aggrieved patients would not necessarily agree with can also affect classifications. These are therefore two sources of possible misclassification. The potential classification errors might also affect the reliability of the quantitative measures of incoming complaints, for example, concerning proportions between complaints regarding treatment and medical treatment. However, all cases categorized by the Patients' Advisory Committee as ‘treatment’ complaints were categorized by us according to their main content, which corrects misclassifications within this main category as far as the information in the filed reports permit. No cases were assigned to more than one category.
Main reasons for complaints about treatment
The largest category of treatment complaints (22%) concerned rude, arrogant or aggressive behaviour, or a disrespectful attitude. In other words, complaints that health-care personnel failed to show a minimum of respectful behaviour. The second largest category (19%) contained complaints about being ignored or not being taken sufficiently seriously as patients – complaints more specifically relating to expectations concerning health-care personnel. The third largest category (9%), being denied something requested such as a certain examination or specific medicine, arguably related to unmet expectations concerning Swedish public health care. Together with the following three categories of complaints – lack of empathy (6%), lack of respect for personal integrity (5%) and complaints related to time (5%) – these categories cover most of the specified treatment complaints, although there were complaints also concerning personnel failing to separate private and professional life, injustice and discrimination, sexual harassment, and coercion and violence.
Other studies – from Australia, Sweden and USA – also point to experiences of being disrespected as a major reason for patients' complaints about treatment. 14,15,17–19 Some of the examples given included being ignored or not being taken seriously, lack of empathy, personnel being ‘rude and condescending’, arrogant or having ‘no bedside manner whatsoever with adults’. 19 However, it is difficult to compare in any detail different studies of how patients are treated in a health-care setting since different categorizations were used. There are many similarities, but also important differences. For instance, ‘communication’ is given as a category in several papers. This category can cover improper information routines as well as incorrect behaviour by personnel giving the information.
The proportion of women reporting bad treatment to the Patients' Advisory Committee was larger than that of men. This remains so after correction for overall consumption of health care, where women accounted for about 60% (which can partly be explained by their enrolment in maternal care). 5 Other studies, from Sweden and Australia, show similar results regarding patient complaints. 17,18,23 Our study provided no indication of why this is so. Thus, we do not know if women were more inclined to report complaints or if women were treated worse than men. The latter has been hinted at in a previous study based on material from the Patients' Advisory Committee. 11
Experienced and actual bad treatment
The complaints to the Patients' Advisory Committee in Stockholm revealed that quite a few patients experienced something that they perceived as bad treatment in their contacts with health care. But they did not tell us with any certainty what really happened or whether the patients' indignation was justified. We can only make an educated guess that in some cases it was and in some cases it was not, which is also the conclusion drawn in studies that have looked into the estimated validity of patient complaints. 20,25 There are a number of uncertainties: (1) did it happen (as perceived) or not? (2) If it did, is the behaviour correctly labelled as bad treatment? (3) If the patient indeed was treated badly at some time, who or what should be blamed – the doctor, the nurse, the patient or something else?
First of all, there is a difference between, on the one hand, experiencing or being under the impression that something has happened, and on the other hand that something has actually happened. There are such things as delusions and misunderstandings. We also know that our moods and feelings can strongly taint our experiences at times. Since the patient can perceive being badly treated or not as well as be badly treated or not, there are four possible outcomes of medical encounters in this regard, as illustrated in Figure 1.
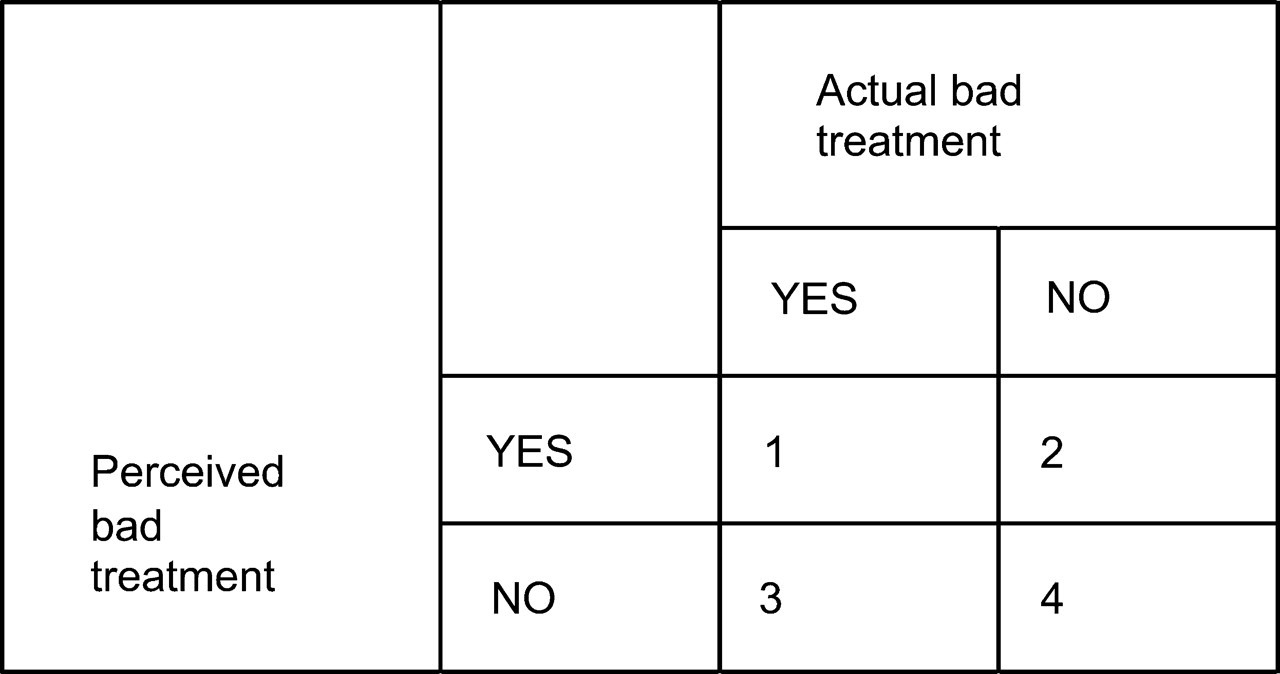
Possible relationship between perceived and actual bad treatment
Most medical encounters do not contain any element of bad treatment and are not experienced as negative. The vast majority of patients' encounters with health care in Stockholm County therefore represented field 4 and thus are not presented in any Patients' Advisory Committee report. Another conceivable set of cases that would not show up in the Patients' Advisory Committee reports is that of patients being exposed to bad treatment without recognizing it (field 3). One example would be if patients were treated unjustly without their knowing it. Patients being ignored or not being treated sufficiently seriously, but believing such behaviour to be normal and therefore acceptable, would be another example. Research regarding homeless people in Stockholm County indicates that this set is not empty. 26
It is obvious that those who do contact the Patients' Advisory Committee truly feel disappointed, wronged, maltreated or offended. It requires time and effort to go through with a report and most people would not do it unless they were upset. However, what is considered offensive differs significantly between individuals. Most likely some patients occasionally complain to the Patients' Advisory Committee about things that a neutral observer would not consider as bad treatment (field 2).
Some of the cases in the Patients' Advisory Committee reports emerge as apparent examples of bad treatment (field 1), not least those where health-care personnel have acted in a way that would not be accepted in other social contexts, such as intentionally hurting or humiliating the patient. Here we also find complaints about staff who do not apologize when something goes wrong. This seems to make it much worse from the patient's perspective (there are many examples of this in the Patients' Advisory Committee reports). We find it feasible to assume that apologies can prevent major discontent and that many complaints to the Patients' Advisory Committee could have been avoided if the person responsible for the mistake had only behaved empathically and friendly and had apologized and explained the mistake. There is some support for this view in the literature. 27–29
Other reported cases are less obvious. For instance, what some perceive as normal communication between doctor and patient, others might perceive as patronizing. It is part of the professional role of doctors, nurses and other hospital staff to behave in a friendly, attentive and understanding way in their encounters with patients. If they do, then complaints about their behaviour usually have little moral weight.
Justified or unjustified expectations?
When there is no disagreement regarding who did what, there might still be disagreement regarding the reasonableness of what was done. While rude, arrogant behaviour is not acceptable in any health-care situation, denying patients examinations or medical treatments that they request certainly might be, not least in publicly financed health care. There are quite a few complaints of the latter kind. Both kinds of behaviour might be perceived by patients as equally upsetting, while prioritizing in accordance with established and reasonable health-care policies is what physicians should do. In other words, what is experienced by the patient as bad behaviour may actually be commendable behaviour.
Individual or organizational flaws?
Some complaints concerned cases where patients were deeply disappointed and where they arguably were not treated well, but where the blame could not (fully) be put on individual physicians or nurses. Instead, structural or organizational limitations and official priority setting affect how the patient is treated. 29 Complaints regarding access to health care, too little time when seeing the doctor and stressed personnel concern such organizational aspects. Refusal of examinations or medical treatments requested is normally due to planned restrictions – restrictions that, in principle, could be immoral but which doctors and nurses are required to follow. Regardless of the reason why patients are displeased with a decision, the message should always be delivered in a friendly and respectful way.
What can be done to improve the situation?
Most meetings in the health-care setting do not result in bad recollections for the patient, but unpleasant experiences tend to be remembered. This could affect trust, even if the majority of remaining experiences are positive. Some of the complaints to the Patients' Advisory Committee may not have much substance, but a reasonable and responsible approach to the cases is that they point at a number of flaws in the behaviour of health-care personnel towards patients. Stressing the importance of these encounters in professional training is important. Perhaps this needs to be done to a greater extent than it is done today.
Respectful and kind behaviour towards patients is important not only for the immediate wellbeing and self-respect of patients. It might also affect patients' health and safety in the longer run by generating greater trust and better communications in both directions: doctors are likely to be better informed about the patient's status and the patient is likely to become better at and more interested in following the doctor's recommendations. 11–13,30 Better communication might also lead to a better understanding of the limited resources of health care and lead to an adjustment of sometimes unrealistically high expectations.
Conclusion
The reports to the Patients' Advisory Committee contained a wide range of experiences of bad treatment in health care, including that patients have been insulted or yelled at, that their personal integrity has not been respected, or that they have not been properly listened to or cared for. Among the most upsetting experiences were those where health-care personnel did not respect well-established social norms of decent behaviour. Experiences of bad treatment were quite often associated with discontent with medical treatments or other therapies and then seemed to reinforce the dissatisfaction.
It is likely that not all complaints were based on events where someone had actually wronged the patient. Patients might at times experience situations very differently from the way a neutral observer would. They might also have unrealistic expectations on publicly financed health care. This study indicates that respectful behaviour towards patients might prevent some of the complaints made by patients.
Footnotes
Acknowledgements
Financial support from the National Board of Health and Welfare is gratefully acknowledged.