
Abstract
Clinical ethics committees (CECs) in the United Kingdom (UK) have developed significantly over the past 15 years. The issue of access to and participation in clinical ethics consultation by patients and family members has, however, gone largely unrecognized. There are various dimensions to this kind of contact, including patient notification, consent and participation. This study reports the first specific investigation of patient contact with UK CECs. A questionnaire study was carried out with representatives from UK CECs. Results suggest that patient participation in clinical ethics consultation is low and unlikely to change significantly in the near future. Attitudes towards patients having a role in clinical ethics consultation are mixed, with a variety of reasons put forward both for and against patient participation. These results are discussed in the light of common themes in the literature and the practical and political context of clinical ethics support in the UK.
Introduction
The establishment and function of clinical ethics committees (CECs) in the United Kingdom (UK) remains an evolving process. Although an early CEC was convened in 1983, the majority of the other 80 or so committees now registered with the UK Clinical Ethics Network have been founded over the past 15 years.1–3A committee structure is the most common mechanism for deliberating about clinical ethics issues, although there are individual ethics consultants at a few hospital sites. CECs have developed in response to a perceived need by motivated clinicians at individual hospitals rather than a national policy mandate. However, support for committee development has also been given by professional organizations such as the Royal College of Physicians. 4
As is the case elsewhere, there has been discussion and debate on how UK CECs function, including their role in the health-care system,5,6 criteria for evaluation, core competencies and who can access the committee. In spite of this, UK committees are actively undertaking a tripartite role comprising case deliberation (both prospective and retrospective), ethics education within health-care trusts and policy development on a local and national level.
The question of access has informed this paper, as anecdotal evidence suggests that to date UK CECs have tended to operate for health professionals only. The question arising is therefore: what degree of access to and participation in UK clinical ethics consultation do patients and their families have?
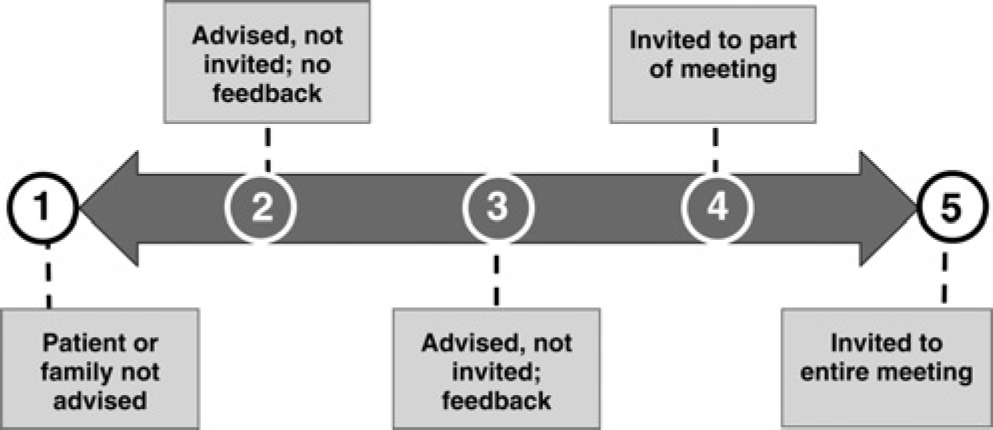
This issue of the patient's role and participation in clinical ethics consultation has been described as an important ‘second-generation challenge’ facing CECs. 7 It is a complex problem, not least because there are many possibilities for patients to either have access to or participate in ethical deliberations about the care they receive. Access in this context can be taken to mean being able to commission or refer an ethics consultation to a CEC, which gives rise to the question of exactly who should be able to commission a consultation. There is also a spectrum of potential participation, as Stidham et al. 8 have previously identified (Figure 1). When a need for ethics consultation arises, should the patient or a family member always be advised? Should they always be invited into the discussion and, if so, for what duration? At the end of the consultation, what should be reported, and to whom?
A spectrum of patient access to and participation in clinical ethics consultation. Points 1-3 deal with advising/ notification of patients; points 4-5 relate to involving patients in the ethics consultation
8
Of the limited current guidance governing clinical ethics and consultation in the UK, there is very little that explicitly addresses advising and participation of patients. The Royal College of Physicians has stated that patients’ input and values are important for the resolution of an ethical issue in health care and that CEC membership should include the patient perspective. 4,p.xi Yet they stopped short of recommending that CECs should always accept case referrals from patients or engage patients in an ethics discussion. In the context of critical care in fetal and neonatal medicine, the Nuffield Council on Bioethics has recommended that both parents and health professionals have equal access to CECs, but again there is no recommendation on the mechanisms through which this may be achieved. 9
In contrast, guidance in countries such as the United States has recommended that patients and families should have access to ethics consultation services (including the ability to commission consultations) and that patients should be notified about an ethics consultation where their involvement in decision-making is needed.10,11 There are also further issues about patient consent as opposed to patient notification to ethics consultation that are of interest, but fall beyond the scope of this paper.12,13
Several US studies have included an investigation of patient participation in CECs. For example, a 2001 survey of 1000 hospital ethics committees found that 94% allowed patients or families to request or commission consultations and 73% communicated directly with patients. 14 Of those patients who have been involved in consultation, one small study has indicated that a small majority (57%) found the consultation helpful, for reasons including clinical clarity, validation of a decision, moral awareness and empowerment. 15
The participation and role of patients in UK CECs has not yet been investigated. To this end, a short survey was designed to determine the degree to which UK CECs have contact with patients and, if so, in what ways. A secondary aim was to explore attitudes to the topic of patient involvement in clinical ethics support. The results and implications of this survey are discussed in this paper.
Methods
To investigate patient access to and participation in ethics consultation in UK CECs, an 11-item questionnaire was designed to reflect relevant themes in the literature (Appendix). The questionnaire contained a mix of closed and open-ended questions designed to establish the committee's activity in case consultation, contact with patients and attitudes to patient involvement in clinical ethics support. The questionnaire was piloted with the Chair of one UK CEC and shown to two other academics active in the field of clinical ethics. After some refinement, the survey was adapted for online implementation via the Bristol Online Survey (BOS) Tool. 16
An email announcing the study was circulated to one chair or administrator from each CEC registered with the UK Clinical Ethics Network in January 2008. The survey remained active for eight weeks, with a reminder sent to all chairs five weeks into the study period. Results were collected from the BOS system and quantitative data were collated using Microsoft Excel. Given the small sample size, analysis of all free-text data comprised categorization and matching of data with quantitative responses, before deducing key themes.
The survey was deemed service evaluation by the National Research Ethics Service and was deemed to not require hospital Research and Development approval. The Faculty of Medicine and Dentistry Committee for Ethics at the University of Bristol approved the study, reference: 070805. Completion of the survey was anonymous save for the geographic area of the committee, which itself was an optional question.
Results
Response rate and demographic information
Forty-five responses were received from a possible 75 committees, a response rate of 60%. All geographic regions of the UK were represented. Completers were predominantly CEC chairs (n = 28, 62%), with other respondents being deputy chairs (n = 6, 13%), CEC members (n = 4, 9%) or administrators (n = 3, 7%). The majority of respondents’ committees were located within acute health-care trusts (n = 28, 65%), with others located or integrated across more than one trust, in an ambulance trust, in primary care, in mental health, in palliative care or in paediatrics.
Participation of patients in committee work
Forty respondents (89%) sat on committees that provided ethics case consultation, either retrospective or prospective. Of these, just over half (n = 23, 58%) stated that they did not currently have any form of contact with patients, corresponding to number 1 in Figure 1. Seventeen respondents (43%) reported that they did have some form of contact with patients, although the majority of these (n = 12, 71%) stated that they estimated that less than 10% of their overall caseload included the active involvement of patients. Two respondents did, however, indicate that contact with patients occurred in more than 50% of their work. This contact is not always interactive; for example one respondent stated that their contact is mainly with incapacitated patients. A minority of committees (n = 4, 9%) had contact with patients in a capacity other than case consultation, for example policy development.
Ways in which patients have contact with CECs
Respondents who had contact with patients were asked to select any of a range of non-mutually-exclusive mechanisms by which patients initially become involved with the committee, or to specify any other ways in which patients become involved. The most popular method was when a member of the CEC had direct contact with a patient (40% of responses). Another mechanism was when the health professional who requested the ethics consultation invited the patient to be part of the discussion (23% of responses). One respondent reported the use of posters to advertise their service in the hospital.
Respondents were also asked about the ways in which patients are then involved in the ethics consultation process, again by selecting from a range of non-mutually-exclusive options. The most popular way to involve patients was to advise them of the consultation (27% of responses), corresponding to number 2 in Figure 1. The second most popular method of involving patients was to provide them with feedback following the consultation (20% of responses; number 3 in Figure 1), via either the committee or the referring health professional. Less popular methods involved asking patients for consent before their case was discussed (15% of responses) or inviting patients to attend either the CEC meeting or a separate meeting (12% of responses; numbers 4-5 in Figure 1). Another respondent indicated that if the patient or a family member was not advised of the consultation (against their standard practice) then the case would only be discussed in an anonymized form.
Likelihood of having patients participate in future
Respondents’ attitudes to the likelihood of involving patients in their CECs in the future were mixed. The most popular response, chosen by 19 responders (43%), was that it was ‘not at all likely’ that they would have contact with patients in the next 12 months. A further eight respondents (18%) did, however, indicate that having contact with patients was ‘extremely likely’, while seven (16%) remained uncertain. As Figure 2 illustrates, those committees who do not currently have contact with patients are less likely to have contact with patients in the future than those committees who do already have contact with patients. Responders from CECs who already have contact showed a more even spread of likelihood of future contact.
A comparison of the likelihood of patient contact in next 12 months between respondents who already have contact with patients and respondents who do not have such contact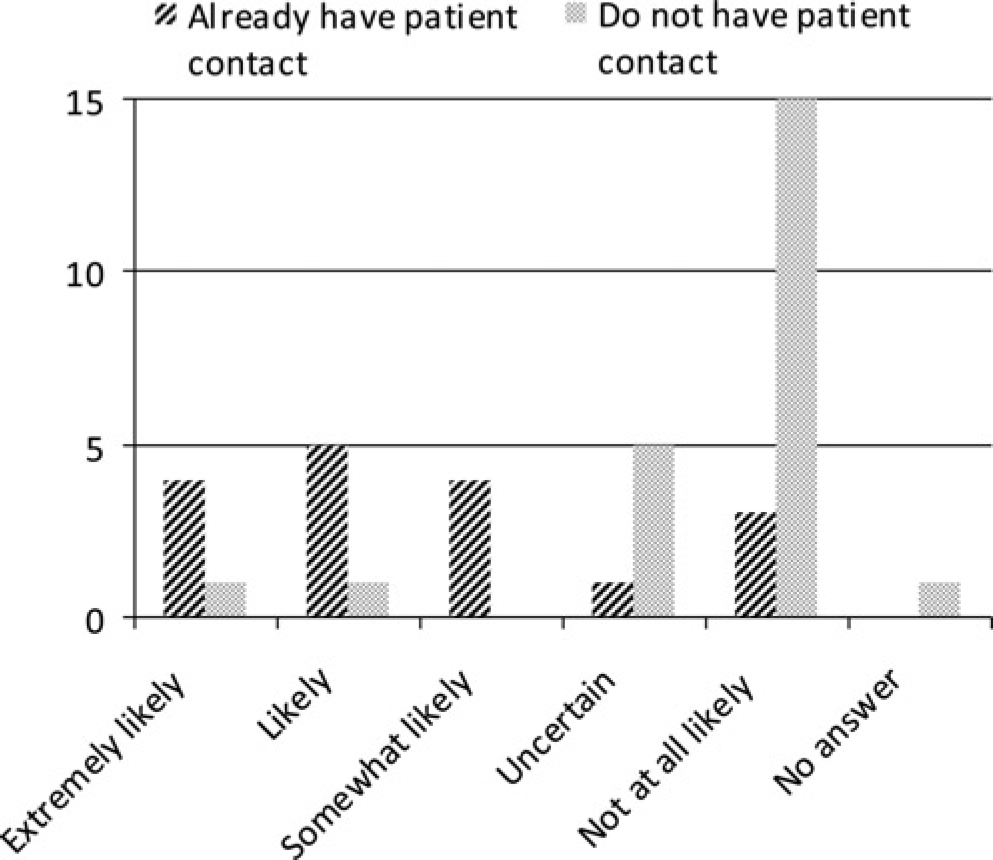
Attitudes to patient participation in CECs
Responders were also asked, in a personal capacity, to express their opinion as to whether UK CECs should have contact with patients. The response was mixed, with 19 responders (43%) indicating that they agreed that CECs should have contact with patients. Eleven respondents (25%) said ‘no’, while 14 (32%) were unsure. Participants were also given a free text field in which to elaborate on their answer. These responses were classified according to the response and common themes were identified. These themes are shown in Table 1.
Common free-text reasons arising in responses to the question ‘Do you personally believe that clinical ethics committees should have contact with patients?’ arranged by how the question was answered
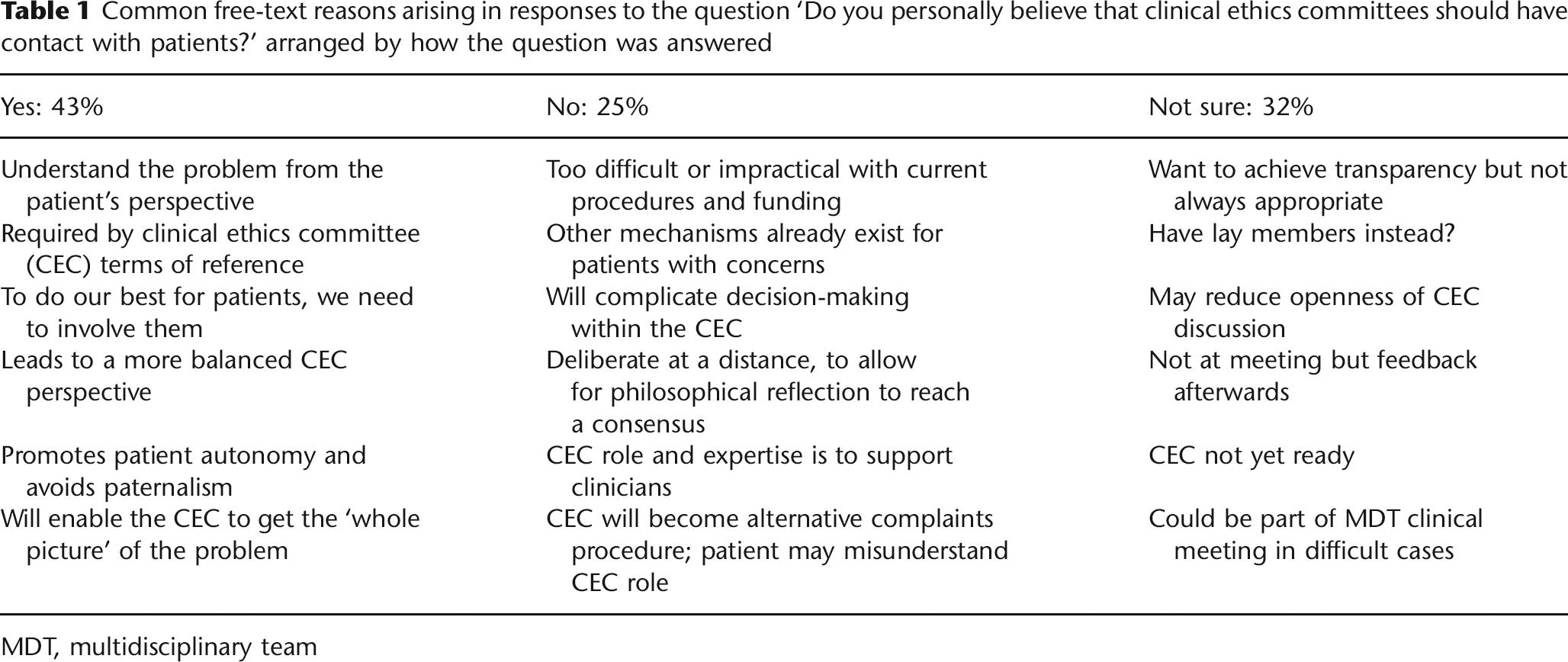
MDT, multidisciplinary team
Some respondents provided qualifications in their answers. For example, one respondent who clicked ‘yes’ to contact with patients provided a further qualification in their response:
‘Only in limited circumstances… The decision-making power of the CEC should also be made very clear to the patient so that s/he has appropriately modest expectations of what powers the CEC will exert. There can be no doubt that the powers continue to reside with the patient and their [clinical] MDT [multidisciplinary team]’ (Response 01).
A further respondent suggested that being in favour of patient participation was only the first part of the challenge, in that ‘The main problem is getting this information to …[patients and their families]’ (Response 08). A respondent who said ‘no’ to patient contact stated: ‘I do feel however that representatives from the CEC should have contact with patients on request as part of a multidisciplinary [clinical] meeting in difficult cases’ (Response 25).
Respondents who indicated that they were ‘not sure’ about patients having contact with CECs highlighted the tension in ethics support between the committee and consultant model. Patients may experience difficulty in appearing before a committee as opposed to having a discussion with an individual consultant. There were also concerns about whether the committee structure actually exists to support professionals, while an individual consultant could better support patients. For example, one respondent stated:
‘We need to be clear on referral mechanisms and pathways and we feel this needs more work. There are those who feel that direct access of patients and parents to CEC, as opposed to ethicists, does somehow compromise clinical care and undermines professionals…'(Response 45).
Attitudes towards patient involvement also showed a degree of correlation with future intentions towards patient involvement. For example, of the 19 respondents who answered ‘yes’ to the question as to whether patients should have contact with CECs, 42% (n = 8) answered that their committee would be likely or extremely likely to have contact with patients in the coming 12 months. In contrast, only three (27%) of the 11 respondents who answered ‘no’ to the same question considered that their committee would see patients in the coming year. Likewise, seven ‘no’ respondents (64%) stated that it was ‘not likely’ that they would have contact with patients in the coming 12 months, compared with five (26%) of those who considered that patients should be involved.
Discussion
Role of patients in UK clinical ethics support
The results of this small study provide a snapshot of the current role and participation of patients in UK CECs. The status quo appears to be one in which less than half of those committees who provide case consultation have some form of contact with patients, and for those that do see patients this forms a small component of their overall caseload. Some respondents indicated that they were likely to have contact with patients in the coming year.
It therefore appears that patient notification, participation and reporting are currently low. It is, however, interesting to observe that despite the relatively low involvement of patients in clinical ethics consultation and deliberation, respondents appeared to have a sound knowledge of the possibilities of patient involvement and the nuances of the debate over this.
Mapping attitudes to the existing debate
Unsurprisingly, the mixed response to involving patients in clinical ethics support observed in this study reflects the broader debate surrounding patient participation in clinical ethics support. A body of literature covering these debates has been published over the past two decades, most of it from North American scholars. Most of the reasons advanced in this literature for and against the participation of patients in clinical ethics support have been reflected in the responses to this questionnaire.
Reasons given by respondents to this survey that have been canvassed in the literature include the following: involving patients in clinical ethics support will respect their autonomy and right to self-determination with full information; facilitate better clinical decision-making; and reflect multidisciplinary care and ensure all perspectives are represented.7,8,17–19 One reason not identified by the small group of participants in this survey is that involving patients can actually protect their confidentiality. 20 Another reason is that involving patients will uphold mutuality - the idea of ‘patients as partners’.
Respondents who articulated some of the reasons against involving patients in clinical ethics support also picked up on existing themes in the literature, such as the CEC becoming a complaints forum or a surrogate patient advocate; that good alternatives already exist to help patients; that a patient's presence may inhibit discussion; and that ‘arm's length’ deliberation to reach a consensus might be threatened (thus reducing the objectivity of the CEC). One respondent also picked up on the fact that as patients’ cases are often discussed in multidisciplinary clinical teams, why should an ethical aspect be treated any differently from a clinical aspect?7,14,21 There may also be those ethics consultations that are, by virtue of the specific dilemma, inappropriate for patient participation. 13
Practicalities of patient participation in UK clinical ethics support
A key question arising from these results is what implications, if any, this debate should have for the practice of clinical ethics in the UK. In addition to addressing the normative force of empirical evidence, addressing this issue will necessitate consideration of the practicalities of the UK clinical ethics framework and the publicly funded health-care system in which it is situated.
UK CECs have tended to be established by a core group of motivated clinicians and most operate with a minimal budget. Members are volunteers (with the exception of a few professional ethics consultants) and many work outside the campus where the committee is located. These factors will influence the ability of a committee as a whole to handle patient participation in a consistent manner and to deliberate when it may be appropriate to notify or involve a patient, or to receive a consultation request. Most CEC chairs are clinicians and so are used to engaging with patients as part of their daily work. However, treating a patient clinically and entering into an ethics deliberation are arguably different and so will require a different set of skills. Some respondents to this survey indicated that they would begin to involve patients when they were better established. Others may argue, however, that if this is important, then it should be built into procedures from the outset.
There are no overarching goals for CECs in the UK, although most committees have their own terms of reference. It is interesting to consider the responses from those ‘not sure’ about patient participation, which highlighted whether UK ethics support is for clinicians or for everyone. Patient participation could be viewed as inherent to success in clinical ethics consultation. But the patient is not currently at the heart of the CEC system. If or when an ethics consultant model gains popularity, this status quo may change.
Any committee considering patient participation will also have to consider questions such as advertising, response times and financial implications, and sound policies will need to be in place.7,18,22 It might be argued that to fulfil the ambitions of clinical ethics consultation and maximize its benefit for the health-care site as a whole, patients should have the same right of access to consultation as the clinicians who treat them. But in a healthcare system reliant on rationing, this may be difficult to justify given the resource implications it will give rise to.
Limitations of this study
The questionnaire used in this study did give rise to some responses that took ‘patient contact’ to mean patient or patient-liaison membership on a CEC, or CEC members having contact with patients in their professional capacity, rather than involving those patients whose circumstances give rise to an ethical problem. Future studies will make the scope of the questions clearer. Further work could additionally explore whether any UK CECs have yet developed or implemented any policies on the role of patients in clinical ethics deliberation.
The methods by which patients are notified of or participate in an ethics consultation cannot be weighted as they were not ranked in the questionnaire. However given the exploratory nature of this study, the goal was to identify the range of methods used rather than stipulate the most popular.
Conclusion
Since CECs in the UK have been increasing in number for over 15 years, the time is now appropriate for them to consider a role for and participation of those patients whose clinical circumstances give rise to a request for ethics advice. As CECs continue to develop in the UK National Health Service, there will be more consultations taking place and this question will become more acute.
This preliminary study provides some insight as to why patient involvement in UK clinical ethics consultation is not yet as common as we may expect. Results suggest that the UK currently lags behind North America and Europe when it comes to patient participation. But before condemning the UK approach, there needs to be a greater discussion of the value of patient involvement. This should include factors such as the ambit and objective of ethics consultation (is it just for National Health Service professionals or patients too?), procedures for notification and reporting (including recording the consultation in patient notes or file) and whether patients can request a consultation.
Consideration should also be given to patient attendance at consultations, other than ‘bedside’ consultations, where the patient is automatically included. How might this impact on clinical staff and CEC members’ ability to have an unconstrained deliberation of often complex and nuanced issues? Not all conflicts will involve patients, suggesting that patients should not always be involved. But in many cases there is good scope for patients to participate in at least some of the ethical deliberation arising from their care.
Footnotes
Acknowledgements
Thanks to Mr Andy Cooper and Dr Anne Slowther of the UK Clinical Ethics Network for facilitating the distribution of the questionnaire to chairs of UK Clinical Ethics Committees and for their feedback throughout the period of research. Thanks too to attendees at the 3rd International Conference on Clinical Ethics Consultation (Toronto, 2007) and to members of the European Clinical Ethics Network (particularly the working group on the role of the patient) for valuable feedback on earlier versions of this paper.
Appendix: Survey questions
Possible answers are given in