
Abstract
Clinical ethics has developed significantly in Europe over the past 15 years and remains an evolving process. While sharing our experiences in different European settings, we were surprised to discover marked differences in our practice, especially regarding the position and role of patients. In this paper, we describe these differences, such as patient access to and participation or representation in ethics consults. We propose reasons to explain these differences, hypothesizing that they relate to the historic and sociocultural context of implementation of clinical ethics consultation services (Cecs), as well as the initial aims for which each structure was established. Then, we analyse those differences with common ethical arguments arising in patient involvement. We conclude that there is no unique model of best practice for patient involvement in clinical ethics, as far as Cecs reflect on how to deal with the challenging ethical issues raised by patient role and position.
Introduction
Following the International Conference on Clinical Ethics Consultation meeting in Basel in 2005, a group of European clinical ethicists founded the European Clinical Ethics Network to explore in detail how clinical ethics case consultations are carried out in practice in Europe. While sharing our experiences, we were surprised to discover marked differences in our practice, especially regarding the position and role of patients. We therefore wondered what reasons might explain such differences and what lessons we could draw from different models to stimulate discussion and improve our own practices in clinical ethics, but also to help others who would like to develop such activities in their context.
Little has been written on the role of patients in European clinical ethics consultation services (Cecs).1,2 This is probably due to the fact that clinical ethics is relatively new in Europe and that most existing Cecs were not directly accessible by patients and families until recently. Moreover, the role of patients can differ between two Cecs from the same country and is changing with time; an unsurprising observation given that clinical ethics remains a developing and evolving process in Europe.
In this paper, we explore and discuss the diversity of practices regarding the position of patients in five European Cecs. We also identify some of the ethical grounds that may underpin such differences and examine some of the arguments for and against different levels of patient involvement. The goal of this paper is not, however, to make normative recommendations as to the superiority of a particular model of patient participation. Rather, we aim to provide stimulus for further discussion and debate on European practice regarding patient participation in clinical ethics consultation.
The position of patients in five different European clinical ethics settings
The five European Cecs described here are settings in which we have personal involvement: the Centre d'éthique clinique, Hôpital Cochin in Paris, France (setting 1), Norway (setting 2) 3 , the Hannover Medical University in Germany (setting 3), the Royal United Hospital in Bath, UK (setting 4) and the General University Hospital in Padua, Italy (setting 5). This is therefore not an exhaustive review of all European Cecs models, and descriptions of each Cecs and its function have been published elsewhere.4–9
We focus in particular on three levels of patient, proxy or relative participation in clinical ethics consultation: (1) access; (2) participation; and (3) representation. For simplicity, in the remainder of this paper we will use the term ‘patient’ to describe patients and their proxies or relatives; and ‘clinician’ to denote any member of the health-care team.
Access
The key question for comparison here is: do patients have access to ethics consultation? If so, what is the mode of request or referral for an ethics consultation? If patients do have access, how are they informed of this right and how much do they actually use it?
Setting 1 (Paris, France): In this setting, patients can request an ethics consult by any means (such as by phone, email or personal visit). They are informed of their right to request a consult in the patient information booklet, by posters placed in different locations around the hospital, through press interviews or by visiting the Centre website. A lot of requests arise by ‘word of mouth’. Calls from patients represent one-third of ethics consults.
Setting 2 (Norway): A great majority of the 38 Cecs in Norway will accept case referrals from patients and relatives. However, this service is not well known to most hospital patients. Many Cecs have detailed information booklets as well as information online. It is the policy of Norwegian Cecs that the committee should not accept cases that are primarily patient complaints.
Setting 3 (Hannover, Germany): At Hannover Medical University, patients have access to ethics consultation services - a right explicitly protected by Clinical Ethics Committee Statutes. They are informed about the Cecs through flyers and via the Internet and they are also notified via a brochure of patients’ rights. In 2007, about 30% of requests for ethics consultation came from patients and relatives.
Setting 4 (Bath, UK): At Royal United Hospital, patients are not routinely informed about the availability of Cecs. No consultation has ever been commissioned directly by a patient. The Cecs is considering making itself available to patients in the future.
Setting 5 (Padua, Italy): At Padua Hospital, patients have access to ethics consultation directly (contacting the Bioethics Service) or through the Hospital Public Relations Service. They are informed about the right to request a consultation through flyers, the hospital website, associations of patients and volunteers. Only around 10% of requests are made by patients.
Participation
To describe the way in which patients who are the subject of an ethics consult themselves actively participate in Cecs, we will use an adaptation of the spectrum originally proposed by Stidham et al. 10 The questions that underpin this analysis are: do they participate as much as clinicians and is there any difference in this participation depending on who commissions the consultation?
As per Stidham et al., we have categorized four increasing levels of patients’ participation:
Patient not advised of clinical ethics meeting; Patient advised but not invited to meeting and no feedback; Patient advised, not invited to meeting but feedback provided; Patient invited to the clinical ethics meeting.
As shown in Table 1, our adapted spectrum also includes:
Whether or not the patient is met before the ethics meeting; Whether or not there is follow-up by the Cecs after the ethics meeting; To what extent lay people or patient representatives are part of the whole process of Cecs.
Spectrum of patient participation in five European clinical settings
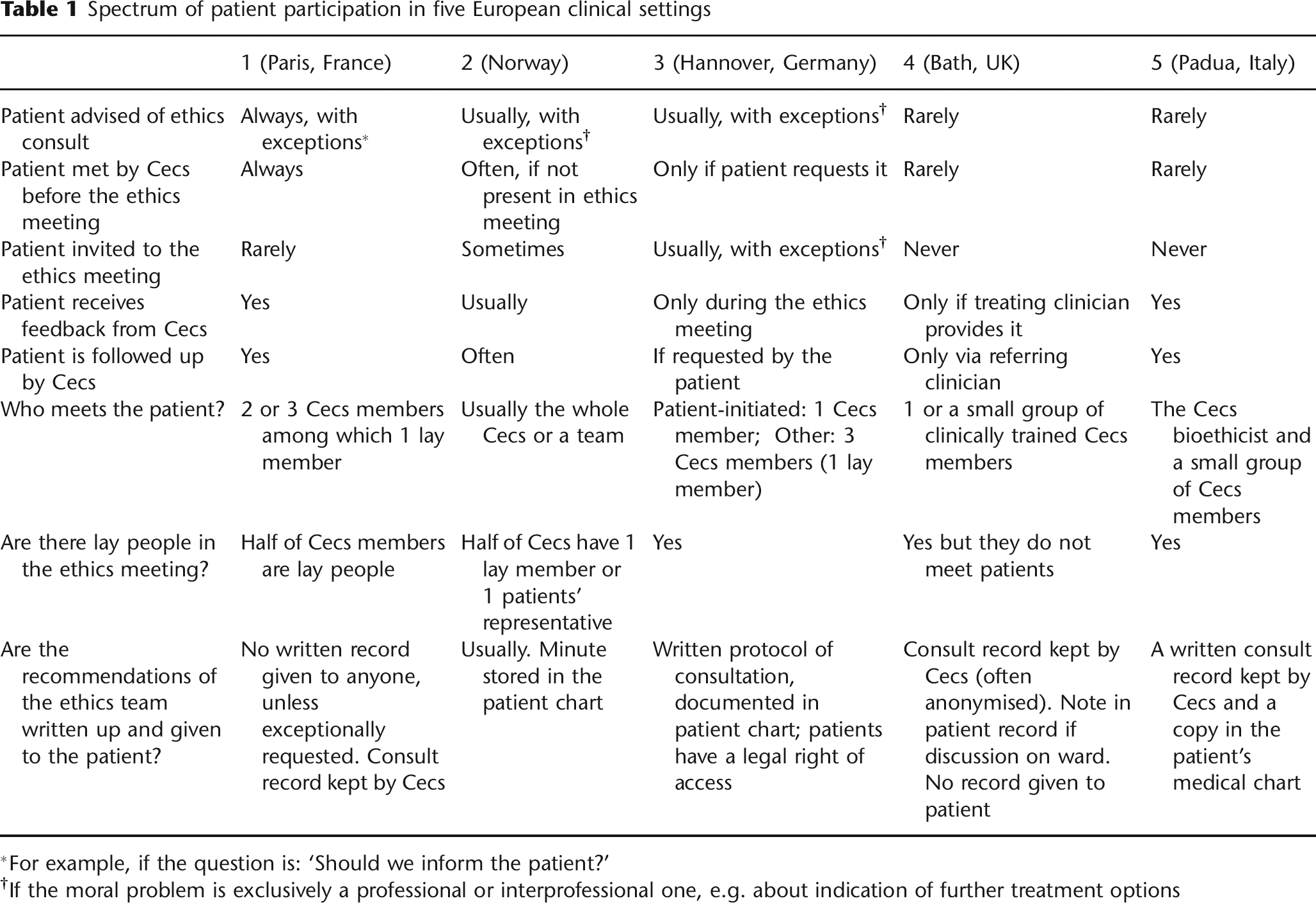
For example, if the question is: ‘Should we inform the patient?’
lf the moral problem is exclusively a professional or interprofessional one, e.g. about indication of further treatment options
To provide a little more information regarding each of the five settings:
Setting 1 (Paris, France): There is no difference in participation regardless of who commissions the consult. Clinicians and patients are both met before the ethics meeting in order to ensure a comprehensive understanding of every stakeholder's position. However, patients are not usually invited to attend ethics meetings, whereas doctors are. This is because their positions are not considered to be equal in terms of personal consequences. This will also help protect patients from experiencing a potentially adversarial environment, particularly one where the patient will encounter a group of 15-20 previously unknown people. Additionally, members of the ethics group have expressed feeling of unease and impediment from full discussion of the issues at stake when the patient is present. The decision to provide no written record at the end of the consultation has been made to respect the decider's freedom. 11
Setting 2 (Norway): Half of the Cecs in Norway are open to the inclusion of the patient during case discussion in prospective cases. The majority of cases are discussed in a committee setting; no Cecs employs an ethics consultant to provide individual ethics counselling. Some Cecs meet the patient before the meeting, and then discuss the case; some include the patient in parts of the ethics meeting; and some have the patient present during the whole committee discussion.
Setting 3 (Hannover, Germany): The Cecs operates in a strictly client-oriented manner. If patients ask for counselling, this is dealt with confidentially. Only if the requester wishes to open up the consultation to other people involved in the case will this occur. Nevertheless, in the majority of cases a ‘grand consultation round’ consisting of the patient, physicians, nurses and Cecs members will occur. 12 If the consultation has arisen because clinicians are uncertain whether a hazardous operation is medically indicated, the consultation will usually take place without the patient. This is to protect the patient from potential harm arising from a detailed yet speculative discussion. If the consult concerns matters of autonomy, the patient's presence is considered morally mandatory.
Setting 4 (Bath, UK): Patient participation in Cecs is rare in Bath, as it is in the United Kingdom as a whole. 13 Patients may be advised of an ethics consultation, but this may be after the discussion has taken place. However, some inpatients may be visited by an individual clinically trained Cecs member or a small group of members - often to ensure clinical information is accurate and/or to speak to the wider treatment team following a consult request. Patients do not presently attend quarterly Cecs meetings, for practical and policy-based reasons. If a patient or staff member is consulted on the ward a note may be made in the patient's record. Cases are written up using a proforma document, but these are usually anonymized and are not provided to patients. Patients may receive feedback if the clinician involved provides it. The Cecs often approaches commissioning clinicians after a consultation to determine the outcome and impact of the deliberation.
Setting 5 (Padua, Italy): If a request is made by the treating clinician, the patient is usually not involved. A written record of the consultation is kept by the Cecs and a copy is included in the patient's medical record. Family may be involved if appropriate to the specific context of the case. The Cecs always approaches the treating clinician after a consultation to determine the impact of the deliberation and the case follow-up. When the request comes from the patient, the Cecs members meet her personally as well as her family if she asks for it; the treating clinician may be part of this meeting if the patient wishes.
In addition to active patient participation, there is also the broader question of patient representation within Cecs. The question here is: what is the place or role of lay people in Cecs? Who are they? How are they chosen? What proportion of the Cecs membership do they represent? Are they part of the consultation team, or the ethics meeting?
Setting 1 (Paris, France): The ethics group comprises equal proportions of clinically trained staff and a diverse group of members of patients’ associations, journalists, philosophers, jurists, sociologists and psychologists. This membership is as representative as possible of society's (and therefore patients’) diversity. At least two people are involved in each ethics consult, one doctor and one layperson. Thus, lay people have exactly the same role and place in the whole Cecs process as clinical members.
Setting 2 (Norway): On average each Cecs has 10-12 members. Most members are hospital health-care employees. Half of the committees have a lay person or patient's representative as members. These are often public officials or people working in patient organizations (such as a patient ombudsman). In addition, many Cecs have an external ethics member, member with legal training or member from primary health care.
Setting 3 (Hannover, Germany): Five out of 18 Cecs members are lay people. One is a judge, one a hospital chaplain. The other three represent different patient perspectives: two are from regional self-help groups and one represents the health-related interests of ethnic minorities and migrants.
Setting 4 (Bath, UK): The Cecs currently comprises 12 members, of whom five are non-clinical. These members are a psychologist, a member of the complaints department, an academic ethicist, a legally trained lay person and a hospital chaplain. All members of the group actively participate in case discussions, either by email (using de-identified information) or at meetings. For reasons of convenience, it is usually only the on-site clinically trained members who consult with patients.
Setting 5 (Padua, Italy): The Cecs has 17 members, seven of whom are lay people: a jurist, a philosopher, a psychologist, a patient organization representative, a chaplain, a sociologist and a journalist. All lay members are external to the hospital and are designated by the director of the hospital. All Cecs members participate in case discussions.
Having now described these divergent methods of functioning as Cecs, we will explore the reasons that may explain such differences and their ethical basis.
Possible reasons for these observed differences in patient participation
Our thesis is that there are at least three main reasons that could explain the above differences: (i) the specific background surrounding how the Cecs was established; (ii) the aims of the Cecs; and (iii) the historical and cultural context of the specific country and health service. This is consistent with Agich and Youngner's 14 analysis of the variations of patient involvement in hospital ethics committee functioning, in which they suggested that this reflects ‘the political and sociological realities of the institutional setting, as well as its conception of and commitment to ideals of patient care and professional responsibilities’.
The specific background surrounding how the Cecs was established
Setting 1 (Paris, France): The Cecs was established in 2002, soon after the first French law relative to patients’ rights was adopted. This law gave a greater voice to the patient and promoted shared medical decision-making. Hence, the creation of the Cecs corresponded to the political context of facilitating the transition towards a less paternalistic doctor-patient relationship. Therefore, it appeared essential to give equal emphasis to patients’ and doctors’ voices in the Cecs process.
Setting 2 (Norway): The first committees were established in 1996 as an initiative from clinicians, the Norwegian medical association and ethicists. In addition, the work has received substantial support from politicians from all political parties.
Setting 3 (Hannover, Germany): The Cecs was founded in 2000 after almost a year of internal negotiation and preparation. 15 The first proposal for a Cecs was made by an academic medical ethicist from the Medical University. This was supported by the director of the University Hospital and the Research Ethics Committee (IRB). The goal was to complement the board dealing with research ethics with another responsible for clinical ethics.
Setting 4 (Bath, UK): The Bath Cecs was established in 2000. Like many ethics committees in the UK, 16 it developed from the enthusiasm of a group of clinicians as opposed to an external policy or legal development. The Cecs remains a relatively informal group and does not formally report to any other hospital committee or management structure, although it does produce an annual report and is involved in hospital policy-making activities.
Setting 5 (Padua, Italy): The Hospital (Clinical) Ethics Committee (HEC) in Padua was established in 1996 by the General Hospital Board, in cooperation with an independent catholic Center of Studies in Bioethics (Fondazione Lanza). There was a specific goal of implementing clinical ethics consultation and continuing education in bioethics for the hospital settings through a bioethicist consultant and a small team including clinicians and lay people.
The aims of the Cecs
Setting 1 (Paris, France): The main aim is to help medical decision-making when an ethical dilemma arises, as opposed to promoting moral deliberation 17 or continuing education in ethics for health-care professionals. The second aim is to identify the emerging changes in the collective social values that are mobilized in bioethics. Because of its very diverse composition, the ethics group can play a role in better enlightening these values and can facilitate the readjustment of interactivity between medicine and society.
Setting 2 (Norway): Cecs were initially seen as helping with decision-making for the health-care team. However, politicians also supported the initiative in order to strengthen value issues in health care. Since the Patient Rights Act was passed in 2001, Cecs have been seen as one way to increase the voice of patients and relatives in difficult and controversial medical decisions. Discussion of difficult or controversial cases in a Cecs is also recommended in the recently launched national guidelines for foregoing life-prolonging treatment. 18 The committees’ conclusion is, however, only advisory. The decision stays with the doctor in charge of the patient.
Setting 3 (Hannover, Germany): The preamble of the Statutes of the Cecs states that its main purpose is to support responsibility, autonomy, (mutual) trust, respect and empathy as lived moral values both in clinical decision-making and in relationships among doctors, nurses, patients and relatives. It aims to achieve a status quo in which patients are satisfied with their care and professional staff are satisfied with their working conditions. The four main tasks of the HEC are as follows: (1) sensitization of staff for matters of medical ethics; (2) staff ethics education; (3) moral case deliberation or ethics counselling; and (4) developing ethics guidelines.
Setting 4 (Bath, UK): In the absence of national clinical ethics policy (see below), committees like the Bath Cecs have largely set their own agendas - although members of committees regularly meet at conferences of the UK Clinical Ethics Network. The primary role of the Bath Cecs is to advise on clinical ethical problems. Its terms of reference stipulate that issues of clinical competence, professional discipline or resource allocation fall outside its remit. The Cecs also has roles in medical ethics education in the hospital and advises on local and national policies that have an ethical dimension.
Setting 5 (Padua, Italy): Following Regional Law and Cecs statutes, the main goal is to help medical decision-making when clinical staff or patients face ethical dilemmas or conflicts. A second goal is to develop ethics guidelines concerning several problems present in the hospital, with a particular focus on organizational ethics. The third goal is to promote public discussion between hospital professionals and civilian society on relevant issues in bioethics and clinical ethics, and to provide continuing education for professionals on these issues.
The social and cultural context of the country
Setting 1 (Paris, France): France is traditionally a ‘jacobine’ centralized and paternalistic country, in addition to being quite innovative in the domain of democracy. Currently, there are no legal requirements concerning Cecs and they remain controversial nationwide because of the perceived power they may give to patients. But there is also an increasing trend towards more importance being accorded to patients’ rights and autonomy. Consequently, the Parisian Cecs has had to compromise between these divergent trends. The group has had to determine how to balance respect for the authority and power of doctors (who according to law remain responsible for medical decisions) with promoting a better interaction between medicine and society. 19
Setting 2 (Norway): Patient rights are becoming increasingly important in Norway. But it is widely agreed that doctors must make the final decision, based on the best possible medical knowledge, but after an open decision-making process in which all important values and interests have been taken seriously. Transparency considerations necessitate that written minutes are made following the case discussion.
Setting 3 (Hannover): There are no legal requirements regarding Cecs in Germany. Public awareness of patients’ rights and patient autonomy has been growing since the 1970s, particularly in the fields of informed consent, end-of-life decision-making and living wills. The first proposal for clinical ethics consultation was made in 1997 by the Catholic and Protestant hospital associations, who recommended that Christian hospitals should implement some kind of ethics consultation service. 20 The growing ‘scene’ of ethics committees was encouraged and supported by German hospital accreditation organizations and the German Medical Association. Nevertheless, only a minority of German hospitals currently offer Cecs. 21
Setting 4 (Bath, UK): To date there has been little political recognition of or support for Cecs in the UK, although professional organizations such as the Royal College of Physicians have stated that ‘ethics support is needed everywhere healthcare is provided’. 22 The UK Clinical Ethics Network is also very active in promoting engagement and is taking the lead on issues such as core competencies for ethics consultation. 23 There has been some academic research and reflection to document Cecs activity,24,25 but a more critical approach to the goals of UK ethics committees is still emerging. 26 The context of the National Health Service is increasingly emphasizing patient choice.
Setting 5 (Padua, Italy): In Italy there is no legal requirement regarding Cecs activities, and in most parts of the country there is one hospital ethics committee, which assumes the functions of clinical trial review (as a research ethics committee), Cecs and public discussion on bioethics. In 2004, the Veneto Region (where Padua is located) issued a law that identified two different local ethics committees: a Research Ethics Committee and an HEC. The law defined the composition and functions of both of them. The experience has been very positive, despite resistance from some doctors. There have also been encouraging experiences of such structures preventing legal action, promoting dialogue among and between clinicians and patients, and increasing bioethical debate in the clinical setting.
Discussion
The descriptions of these five settings indicate that there are often differences within Europe as to how and when patients participate in Cecs. We will now reflect on these differences with respect to some of the ethical arguments for and against varying levels of patients’ involvement in Cecs.
Drawing on relevant literature,
14
we consider four main ethical issues that have been identified as potentially problematic to the position of patients in Cecs:
The role of patient autonomy; Pursuing theoretical ethical discussion rather than patient engagement; Not respecting confidentiality; Responsibility.
The practice of ethics consultation can be seen as a balancing exercise. It is important to provide enough, but not too much, weight to respecting patient autonomy and to act without bias or partiality to a particular stakeholder. Arguably, the more important the role of patients becomes in the Cecs process, the bigger the emphasis on respect for her autonomy. As Reiter-Theil 2 has argued: ‘there is no “natural neutrality” in the role of the clinical ethics consultant’, especially if he or she is supposed to provide the ‘confidential and empathic support needed by the patient’. But Reiter-Theil 2 also underlines how important it is to ‘differentiate between (a) adopting the content of the wishes […] and (b) taking them seriously into consideration’ and also to develop a ‘so-called multidirectional partiality’ to balance competing interests.
Strategies can be developed to resist the risk of overemphasizing patient's autonomy over another's. For example, involving several consultants to work on a case, having external members as ethics consultants or being systematically reviewed by an ethics committee very diversely composed are some of the tools that can be used. Having patients present during committee discussion can be helpful in making them realize that their wish for a certain solution may be based on unrealistic expectations or false information.
We should not forget that the most common risk in Cecs is not to over-emphasize the patients’ autonomy but the doctor's position, in particular in committees where the majority of members are health-care workers at the same institution. This can give rise to authoritative doctors who ‘own’ the medical facts, leading to difficulties for the committee to formulate an independent opinion. 27
Pursuing theoretical ethics rather than patient engagement
This problem can arise when the patient is not involved enough in the consultation process, typically when the ethics team do not meet the patient and moral deliberation is mainly conducted away from the ‘real life’ of those involved in the specific case. Not meeting patients at all in ethics consultation may mean that only half of the problem is effectively deliberated, yet for some this may be entirely acceptable if the provision of clinical ethics support is only meant to help clinicians in their work -a narrower focus adopted by some committees in the UK. 13
At the very least, this problem suggests that if a broader approach can be justified, then training and education needs will arise for ethics consultants. That is, ethics consultation should not only involve the weighing of moral principles. It should rather be seen as a process of counselling and deliberation, in which the contingent moral positions, attitudes and convictions of all stakeholders play a part - not merely abstract principles or moral rules. Morality lies in the process of the ethics consult and training programmes should acknowledge this 28 . Ethics consultation should not perform abstract moral judgement as an end in itself, but act as a support for context-sensitive, patient-oriented decisions.
Not respecting confidentiality
A potential challenge to increased patient participation in Cecs is that the more the patient is included in the Cecs process, the more members of the ethics team he or she will meet. This will include Cecs members who are external to the health-care institution, such as lay people. Private details and circumstances will become known by everyone and discussed during the ethics meeting, which may undermine confidentiality. As Neitzke 29 has suggested: ‘ethics consultation has become a relatively new challenge to confidentiality and privacy in the hospital’, for at least four reasons: (i) how to guarantee confidentiality of the ethics consult to those involved; (ii) how to guarantee respect for confidentiality by the members of the ethics committee, especially the lay members; (iii) how to ensure the clinicians will not disclose details irrelevant to the ethical issue under discussion; and (iv) how to discriminate between elements that can be disclosed to the patient concerning the doctor (and vice versa) gathered during the Cecs process. 29 For Neitzke, patient informed consent to disclosure of private information and an explicit written commitment to confidentiality by Cecs members are some of the tools that can help resolve confidentiality challenges to clinical ethics consultation. It is interesting to note that here patient's participation becomes per se an ethical guarantee in the way that the more he or she is present, the more confidentiality and transparency may be respected. However, it is important that the patient knows the character and goal of the consultation and is informed about the type of medical and private information that must be disclosed, to whom.
Responsibility
Responsibility is important to ethics deliberation: who is responsible for what and whom? Does the involvement of patients in Cecs redistribute such responsibilities? As Agich and Youngner 14 point out, clinical ethics consultation contains a risk of ‘diffusion of responsibility’. However, it seems that whereas legal responsibility remains with the clinician in charge, the intervention of Cecs means that moral responsibility will become increasingly shared between the patient, his or her clinician and the wider health-care team. This ‘shared responsibility’ is a new and favourable paradigm in medicine.
Balancing risks and benefits of patient participation
Figure 1 illustrates how the main ethical issues discussed here may manifest differently when deliberating greater or lesser patient involvement in the Cecs process. We suggest that the more a patient is involved in Cecs, the greater the risk of over-emphasizing his or her autonomy over other important ethical considerations - leading to partiality towards the patient. But on the other hand, if patient participation is too low, there is an increased risk that the pursuit of theoretical ethics will override the patient's best interests. Ideally, a system of patient participation should be developed to maximize the outcomes in the middle of the lower half of Figure 1: that is maintaining confidentiality, showing appropriate partiality, ensuring responsibility and balancing autonomy and best interests.
The ‘ethical landscape’ of patient participation in Cecs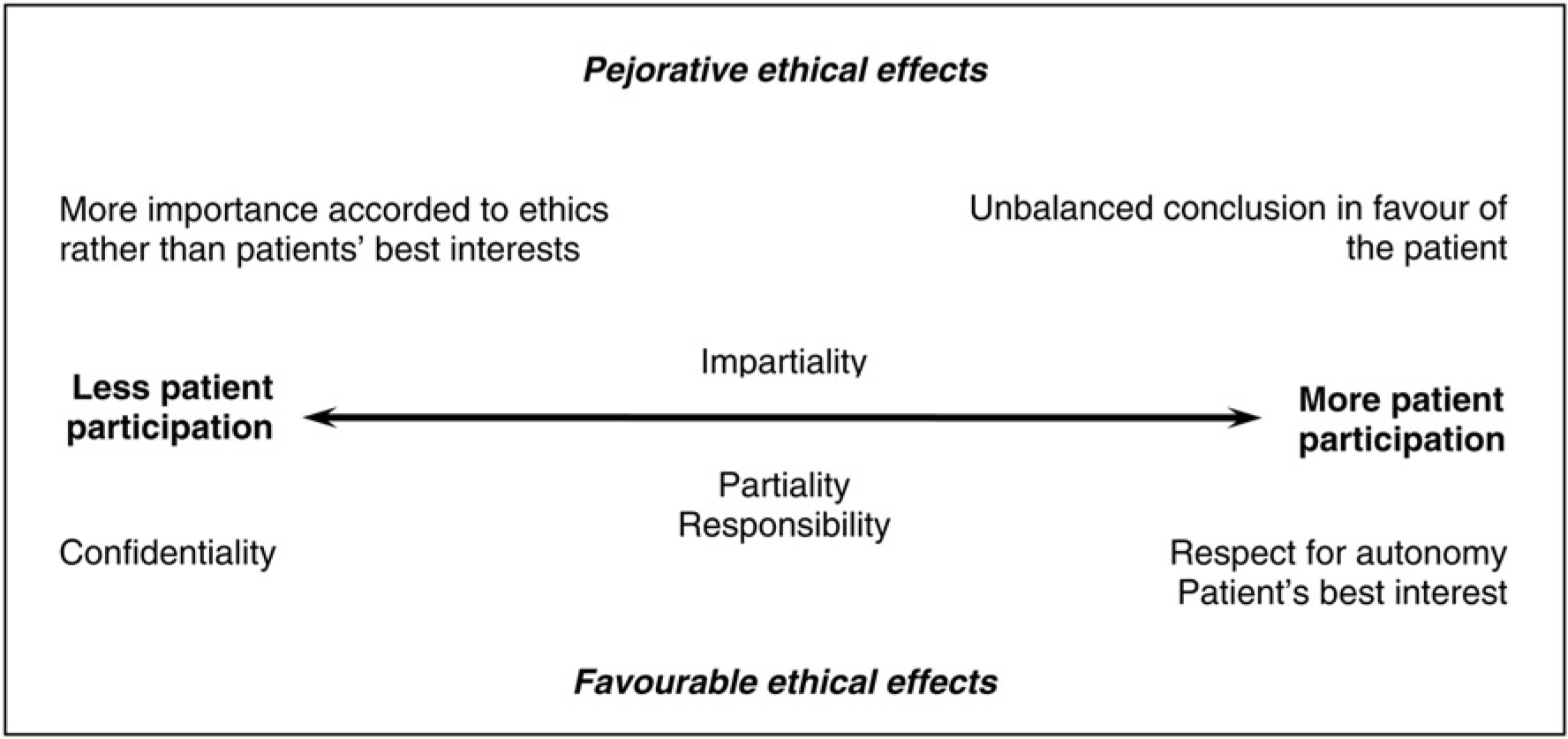
Current policy and practice in each of the settings described here weighs these factors differently, leading to a different position on this spectrum. But all of them have a common objective: that is to maximize the favourable effects and to minimize the pejorative ones, considering the specific context in which they have to work. Further, they all are motivated to continually reflect on their various practices in Cecs and the ethical validity of the processes they have adopted.
Conclusion
In comparing the five different European Cecs settings that we are involved in, important differences have been observed with regards to the position and role of patients. Our hypothesis is that these differences are linked to the historic and sociocultural context of implementation of these clinical ethics support services, as well as with the initial aims under which each structure was established. Yet even if the position and role of patients in Cecs is very different from one setting to another, in each model the same ethical questions about procedures seem to be confronted and treated with similar ethical concern.
Our conclusion is that what is important is that each Cecs finds its own way to deal with these challenging issues. There is no unique model of best practice, but we have suggested a form of equilibrium in which different Cecs can find what will work best for their context. This leads to the idea that if there is something universal in ethics, it is more in the approach than in the result.
Another conclusion is that there seems to be a certain trend in Europe towards greater patient participation in clinical ethics consultations. Nonetheless, much work is still needed to better determine whether and how patients should become more involved (or not), while avoiding an unproductive systematization, insensitive to the cultural, political and contextual differences that define Europe as a whole.