
Abstract
The aim of the present study was to describe and explore the perception of ethical guidelines and their role in ethical competence-building among Swedish physicians and research nurses. Twelve informants were interviewed in depth. The results demonstrated that the informants had a critical attitude towards ethical guidelines and claimed to make little use of them in practical moral judgements. Ethical competence was seen primarily as character-building, related to virtues such as being empathic, honest and loyal to patients. Ethical competence was assumed to be learned through good examples, role models and practical experience, while ethical guidelines were not perceived as valuable in this process. In order to improve the staff's familiarity with and the usability of ethical guidelines, the workplace needs to provide opportunities for ethical dialogues. In such discussions, argumentation can improve, virtues can be developed and guidelines can be usefully invoked.
Introduction
The ethical demands on first-line health-care providers have increased in recent decades due to factors such as improved medical competence, new biomedical technology and scarce resources. Medical practice includes patient treatment and care as well as clinical research. Often, clinical studies are led by a physician as the principal investigator (PI), with a research nurse assisting with the investigation. Arguably, they experience ethical dilemmas in relation not only to patient encounters but also to the studies in which they are engaged. One way to respond to the increased ethical demands in health care and medical research has been to produce ethical guidelines. However, it is still unclear what function the recent vast production of ethical guidelines has had in practice. In the present study, the perception of ethical guidelines for clinical research among Swedish physicians and research nurses has been explored. Further, the perception of ethical competence as well as the role of guidelines in the development of such competence was investigated.
Background
A wide range of studies have reported on the experience of ethical dilemmas for nurses1–3 and physicians.4–6 Also topics such as ethical competence and experiences of moral distress for nurses7–9 and doctors10,11 have had an upswing in interest. Some studies have observed the fact that research nurses12,13 and physicians engaged in clinical trials14,15 experience ethical dilemmas in relation to the studies they are engaged in. In a previous study, 16 we found that research nurses experience severe ethical dilemmas in their daily work (e.g. role conflicts between being a nurse providing care and a research assistant striving to include patients in a study), but that they lack opportunities for ethical competence-building.
Ethical competence in health care has been described as consisting of three dimensions – namely moral perception, moral judgement and moral behaviour. 17 Zhang et al. 18 have argued that nursing competencies include ethical attributes such as traits, motives and attitudes, which are assumed to contribute to effective nursing performance. In a previous study, 19 we have argued that ethical competence must include aspects not only of being (personal character) and doing (acting according to judgements made based on rules and principles), but also of knowing (familiarity with moral traditions as well as laws and guidelines for one's work). In order to bring these aspects together, a communicative ethics model was suggested.
In the late 1990 s, Scanlon 20 argued that one central aspect of ethical competence in nursing is the nurses’ knowledge of and adapting to codes of ethics. Likewise, Commons and Baldwin 21 argued that nursing care can be performed either ethically or non-ethically depending on professional standards for nursing. Such standards are set through nurses’ incorporation of ethical codes for their profession. By this reasoning, ethical codes are supposed to create a barrier between personal values, which might otherwise hinder good care and professional values, which will instead secure ethical care.
Empirical research has revealed a somewhat more sceptical attitude to codes of ethics among nurses. A focus group study on Dutch nurses 22 displayed a common unfamiliarity with codes and also a rather implicit use of them. Further, negative attitudes were found to the growing volume of codes. Similar results were found in a comparative study 23 on the value of nurses’ codes of ethics carried out in six European countries (the UK, Finland, Greece, Poland, Italy and the Netherlands). Most participants had a poor understanding of codes of ethics and also believed that such codes had little practical value.
Concerning ethical guidelines in the practice of physicians, Day et al. 24 found that although the physicians studied were aware of relevant guidelines, only a few actually used them to solve ethical dilemmas or to influence their decision-making in ethically troubling situations. Instead, the informants reported that they relied on previous experience and peers’ opinions when making moral judgements.
An investigation performed by Eriksson et al. 25 identified three major problems related to ethical guidelines – namely the interpretation problem, meaning that there is always a gap between the rule and the practice, which implies that ethical competence is needed for those who are to implement the guidelines; the multiplicity problem, meaning that the great number of codes, declarations and laws might pull in different directions, which may confuse the health-care providers who are to follow them; and the legalization problem, meaning that ethical concerns may take on a legal form, whereby ethical reflection is replaced by a procedure of legal interpretations.
In sum, previous research has shown a common unfamiliarity with ethical guidelines among health-care practitioners, as well as a rather scarce use of them. Furthermore, several theoretical problems with ethical guidelines have been identified. There is, however, a lack of studies on the practical relevance of guidelines and laws that regulate clinical research. How do research nurses and physicians working in clinical studies regard such guidelines? Do they use them in their daily work? And do they apprehend them as useful in the development of ethical competence?
Aim
The aim of the present study was to describe and explore the perception of ethical guidelines among Swedish physicians and research nurses working in clinical studies. Further, the perception of ethical competence as well as the role of guidelines in the development of such competence was investigated.
Methodology
A qualitative methodology with in-depth interviews was chosen. An inductive approach, with no predetermined categories, was used.
Participants
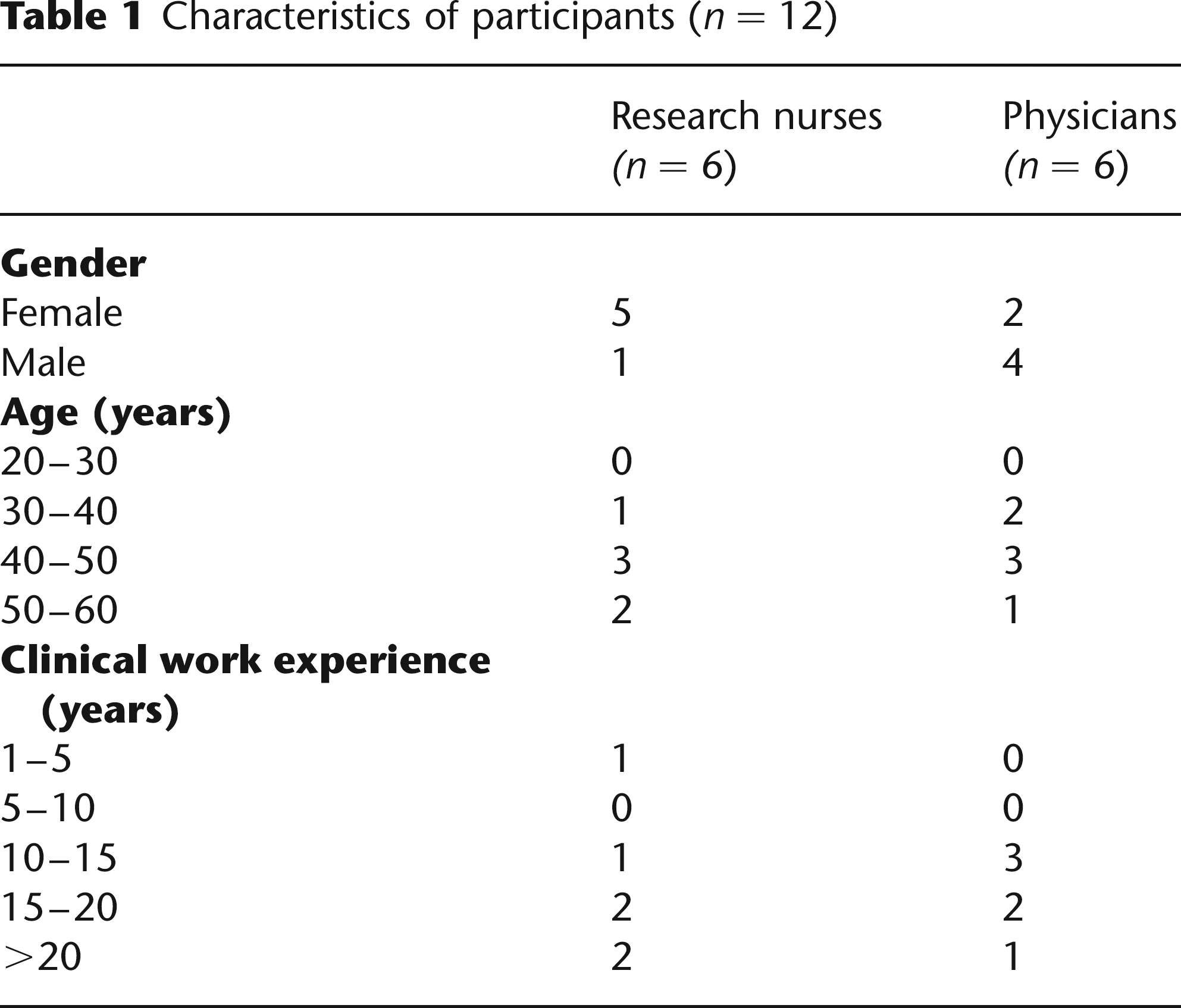
A purposeful sample 26 of 12 informants, consisting of six research nurses and six physicians from five wards of differing disciplines in four Swedish hospitals, was recruited for the study. As the aim was to investigate the informants’ perception of ethical guidelines for clinical research, inclusion criteria were that the informants should be engaged in clinical studies. Therefore, research nurses and physicians involved in clinical research were judged as suitable for the study and were asked to participate. Recruitment was terminated when saturation was reached, i.e., when the last interviews in each category did not add significant, new information to the study. 27
The participants’ ages ranged from 39 to 58 years. Both groups consisted of both women and men. Among the research nurses, five were women and one man. Among the physicians, two were women and four were men. The clinical background of the informants varied from three to 32 years. Characteristics of the participating nurses and physicians are shown in Table 1.
Characteristics of participants (n = 12)
Data collection
Data were collected during 2006 and 2007. All but one of the interviews was conducted by Author 1 (ATH); one informant was interviewed by Author 2 (SE). One interview was, at the informants’ request, conducted with two nurses at the same time (Nurses 5 and 6). The interviews were carried out in a spare room at the informants’ workplaces, and lasted about one to one and a half hours.
A semi-structured manual was used during the interviews. The informants were asked whether they were familiar with some ethical guidelines or laws for their work; how they viewed such regulations; whether they used guidelines in their ethical decision-making; how they understood ethical competence and how such competence was developed. Through asking for concrete examples and situations, the focus was maintained in the interviews. The participants’ answers were often followed up with additional questions by the interviewer.
Analysis
The interviews were tape-recorded, transcribed verbatim and processed as text. The transcribed interviews were sent to the informants for approval. The text was analysed through a stepwise categorization method as outlined by Malterud. 28 The first step was to read through each interview several times in order to grasp the whole of the content. The second step was to identify meaning units. The third step was to code the identified meaning units, and in the fourth and final step the content of these abstracts was condensed and grouped into themes. The analysis process is described in Table 2.
Description of the analysis process through a thematic stepwise method

The analysis of the interviews was conducted primarily by ATH, while the two other authors acted as co-readers.
Ethical considerations
According to current Swedish legislation, formal approval of the Regional Ethics Committee was not required for this study. Throughout the project, the ethics of scientific work as outlined in the Declaration of Helsinki were followed. The participants were included after informed consent; verbal and written information on the study was given; all information has been treated confidentially; and all personal identifiers have been removed so that the personnel and their workplaces cannot be identified in the published results.
Results
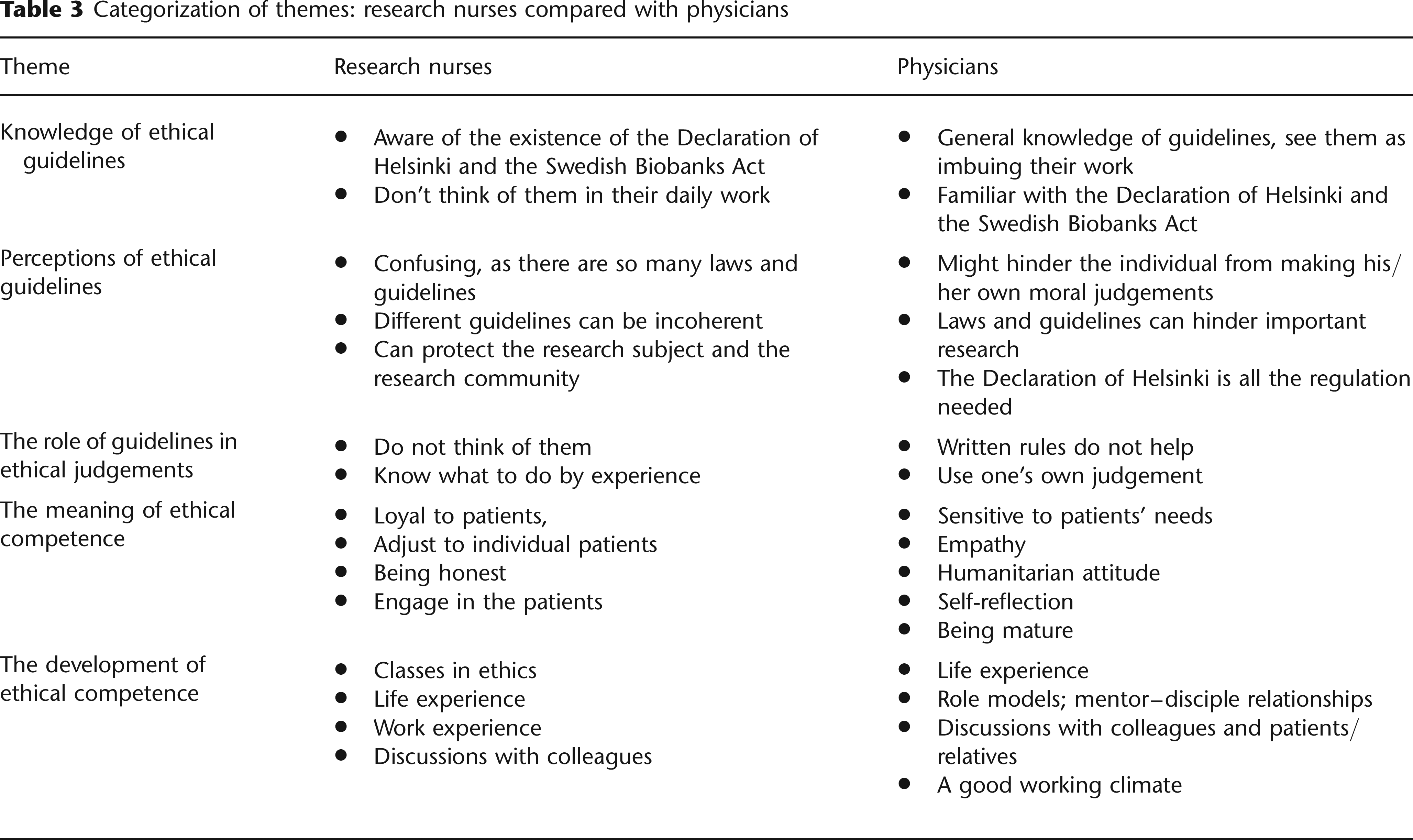
Through the analysis of the interviews five themes emerged, namely:
Knowledge of ethical guidelines; Perceptions of ethical guidelines; The role of guidelines in ethical judgements; The meaning of ethical competence; and The development of ethical competence.
An overview of the themes, with a comparison of research nurses’ and physicians’ perceptions, is presented in Table 3. In the following, each theme will be illustrated by quotes.
Categorization of themes: research nurses compared with physicians
Knowledge of ethical guidelines
One theme that emerged from the interviews concerned the informant's familiarity with and knowledge of ethical guidelines for clinical research. In this case, knowledge was defined as knowing the guideline by name and being able to give a brief account of its content. An ethical guideline almost all informants were familiar with was the Declaration of Helsinki:
‘Already in nursing school the Declaration of Helsinki was presented, together with the law book. So we have had that to lean back upon’. (Nurse 3)
‘I have read the Declaration of Helsinki and tried to understand it. And I see it as directly applicable to research and research ethics’. (Physician 6)
Also, the Swedish Biobanks Act, adopted in 2003, was a regulation almost all informants mentioned in the interviews:
‘One could say that the Biobanks Act is very present in our work. There is definitely a good knowledge of it among the doctors’. (Physician 5)
‘But also the law that regulates biobanking … We know that we need documented consent when we take tissue samples and so on’. (Nurse 3)
A rather common response among the nurses was that they knew that many guidelines existed, but that they were not actively using them in their practice:
‘But, of course, we know that there are rules and guidelines, absolutely. […] But we don't think of them in our daily work’. (Nurse 5)
Among the physicians, it was mentioned that ethical guidelines influenced their daily practice indirectly:
‘There are a number of such rules, which I don't read every day, but they imbue the work, so to say, but not in every detail, of course’. (Physician 4)
Perceptions of ethical guidelines
Concerning how they regarded ethical guidelines, primarily the interviewed physicians expressed a critical attitude. One informant argued that ethical rules might stop the individual from making his/her own judgements:
‘I think it's good that you formulate it and write it down, but there are several risks, too. For example, you risk making the doctor passive in his own judgements. Someone else has thought for me, so to say […] And another risk is that you say: But that's what the principle says … I just followed the principle […] We must teach our co-workers to think for themselves. To think ahead: what would be the consequence if I acted like this? […] You cannot always follow a principle’. (Physician 2)
Furthermore, the problem of how to use and interpret a law or guideline was mentioned:
‘There is a risk that you commit yourself to a particular judgement because ‘this is what the law or some guideline says, so we have to do that’. But, I mean, it is a dynamic process, no situation is exactly the same as another, so you have to adjust to the situation to make the best judgements and decisions’. (Physician 6)
Likewise, some of the interviewed physicians expressed the view that some laws and guidelines could have a negative impact upon their work in research projects; they could sometimes even hinder important research from being performed:
‘In the end some colleagues seem to give up their research, because a lot of good studies cannot be done, as there are new laws and regulations all the time that hinder them. Today you also have to pay quite a lot for an ethical approval, which I think is totally absurd’. (Physician 2)
The great number of guidelines, and the fact that new ethical challenges are often met by the construction of a new guideline, was commented on by a physician:
‘If you don't read and follow the Declaration of Helsinki, it's no use making a new convention, and so on’. (Physician 1)
Also among the research nurses, criticism was expressed regarding the great number of ethical guidelines:
‘It can be very confusing. Where do these guidelines come from? Who says what? I took a class in research ethics and I think I had a whole bunch of laws and guidelines collected from that class!’ (Nurse 3)
Likewise, the fact that different laws and guidelines were not always compatible or coherent with one another was mentioned:
‘Sometimes you feel some kind of tension. The Medical Products Agency says one thing about medical records, but the pharmaceutical industry says something else’. (Nurse 4)
The fact that laws and guidelines could be interpreted in several ways was also mentioned as a problem among the research nurses:
‘And a law … I mean, that's words! You can interpret it in different ways’. (Nurse 2)
However, some positive attitudes to ethical guidelines and laws were identified by the informants. Among the physicians, it was declared that ethical guidelines can function as some sort of checklist in medical research:
‘The Declaration of Helsinki, for example, is good and you should read it before you start a research project. That's what you need to know. It's like a checklist’. (Physician 1)
‘You need to know about certain documents, such as the Declaration of Helsinki, the UN Declaration on Human Rights and the Swedish Medical Association's Ethics Code. In these documents you get your responsibility described quite clearly’. (Physician 6)
Further, two research nurses expressed that guidelines can function as a type of protection, for both the research subjects and the research community:
‘Most of all, it works as a protection of the patients and that's really good’. (Nurse 6)
‘And if someone does something wrong you can use the rules to argue against that person’. (Nurse 5)
The role of guidelines in ethical judgements
Having found that the informants were quite aware of the existence of the Declaration of Helsinki, one can proceed by asking whether they use such a document in their daily work. Do ethical guidelines impact their judgements and decisions? One physician argued that ethical guidelines could have practical value:
‘I think rules and guidelines can improve ethical awareness’. (Physician 3)
But the majority of the informants, among both physicians and research nurses, indicated that they did not use ethical guidelines in an active way in their daily work:
‘I don't feel that written rules can help me so much. Mostly, I use my own judgement’. (Physician 1)
‘You don't think of them [laws and guidelines], you just know what to do’. (Nurse 1)
The meaning of ethical competence
When asked what might be most important in order to perform their work ethically, a majority of the informants, both physicians and research nurses, did not mention familiarity with ethical guidelines or laws regulating clinical research but rather aspects of personal character:
‘You need to be sensitive to your patients’ needs … and you must have a humanitarian attitude … and empathy. As a doctor I must be engaged, but not too personal’. (Physician 5)
‘It's about being loyal to the patients. And I think many nurses have a strong sense of duty. We engage in the patients’. (Nurse 1)
Another important aspect of ethical competence mentioned by some of the interviewed physicians concerned the importance of being a mature and self-reflecting person:
‘You need a high degree of self-reflection’. (Physician 2)
‘I think it is a question of being a mature person’. (Physician 6)
Among the research nurses, it was expressed that personal characteristics that might contribute to ethical care-giving were sensitivity, honesty and respect:
‘You try to be sensitive and adjust to different people. And to be honest! Always tell the truth’. (Nurse 1)
‘It's all inside you. You must act in a way that you would like other people to act towards you’. (Nurse 6)
Some of the physicians mentioned that ethical competence is not just an individual responsibility for the staff, but also a collective or structural skill, and as such a question for the management level:
‘Ethical competence is improved by a good working climate; an open atmosphere between colleagues and staff groups. If we dare to open up and listen to each other and have good communication, these questions will come up’. (Physician 6)
The development of ethical competence
Having stated that both physicians and research nurses in the study saw ethical competence first and foremost as a question of personal character, one can proceed by asking how such competence can be learned and developed. Two of the research nurses mentioned classes in ethics as a source for the development of ethical competence:
‘I have taken a GCP (Good Clinical Practice) course and in that there was a lot of focus upon ethics’. (Nurse 5)
‘I took a class, because I felt that my knowledge was limited, both of ethics and of the rules for medical research’. (Nurse 4)
The most common response to questions on this theme, though, was that ethical competence is developed throughout your entire life. This was mentioned by both physicians and nurses:
‘You learn it during your childhood and your adolescence; to tell right from wrong, and so on’. (Nurse 6)
‘In principle, you are shaped morally from when you are a child’. (Physician 4)
Further, ethics was described by both groups as knowledge you learn from practical work experience:
‘We had one lecture on ethics in medical school … But you don't face the big and difficult questions until after a couple of years’ work. […] I mean, a class might be helpful, but [ethics] is learned practically’. (Physician 2)
‘You learn [ethics] from the studies you work with’. (Nurse 1)
Several of the interviewed physicians also mentioned that you learn from good examples and role models in your work:
‘You learn from role models and through discussions with colleagues, patients and their relatives’. (Physician 1)
‘I think it is as an old-fashioned mentor – disciple education. You can't learn it from a book. You need experience’. (Physician 3)
Concerning the question of whether organized ethical discussions, e.g. in the form of interprofessional ethics rounds,11,29 could be a means to improve ethical competence, most informants described that they lacked such opportunities:
‘We don't have regular meetings. But spontaneously, when something comes up, we discuss with the doctors’. (Nurse 5)
‘It's not formalised; we don't have meetings now and then, so it's up to us ourselves. Sometimes we call our colleagues to an ethics discussion, and on our regular morning meetings it happens that someone addresses an ethical question and discusses it with their colleagues’. (Physician 1)
Discussion
The aim of our study was to investigate how Swedish physicians and research nurses regard ethical guidelines for clinical research. Further, the role of guidelines in the development of ethical competence was investigated. The results demonstrated that a majority of respondents, both physicians and research nurses, knew about the Declaration of Helsinki and the Swedish Biobanks Act; the latter had been enacted quite recently when the interviews took place and is relevant to all biomedical research in which biological samples are collected and analysed. Thus, some ethical guidelines and laws regulating clinical research were acknowledged. Some advantages of ethical guidelines were also pointed out. The physicians stressed that ethical guidelines can increase ethical awareness, by functioning as a checklist. Among the research nurses, primarily the fact that laws and guidelines could contribute to protecting the interests of research subjects was emphasized as a positive aspect.
However, most respondents expressed a somewhat sceptical attitude towards ethical guidelines. Thereby, our study supports earlier findings on this matter.22,23 The informants pointed out a number of potential and real difficulties. First, both groups of professionals mentioned that every law or guideline has to be interpreted and related to the specific situation at hand. This indicates that knowledge of ethical guidelines cannot replace individual ethical competence. Among the physicians, it was also expressed that there is a risk that people commit themselves to a particular judgement because a guideline ‘says so’. In other words, guidelines might prevent healthcare practitioners from relying on their own ethical reflection. This can lead to a replacement of responsibility (‘I did it because the rule said so’), which is even more regrettable since the stated rules might produce the wrong answer to the situation at hand. The coexistence of many legal regulations and ethical guidelines covering the same area further complicates the situation, according to the informants, since one might get incompatible directives from different sources regarding what to do.
This criticism supports several of the ideas of potential disadvantages of ethical guidelines identified by Eriksson et al. 25 The empirical results found in this investigation display examples of all categories suggested as problematic for ethical guidelines, namely, the interpretation problem (a guideline has to be interpreted, hence practitioners need some sort of ethical competence), the multiplicity problem (different guidelines and laws might pull in different directions) and the legalization problem (ethical concerns may take on a legal form, whereby ethical reflection is replaced by non-reflective rule-following).
An additional disadvantage pointed out by some of the interviewed physicians was that legal regulations might hinder important research by making it too difficult to fulfil requirements, too expensive, or too time-consuming to fill in the required forms. Some of these experienced difficulties can perhaps be explained by the relative novelty of and unfamiliarity with the requirements of a new Ethical Review Act in place in Sweden in 2004, in addition to the recent Biobanks Act. However, the fact that extensive regulations can threaten research, for instance by making some research more difficult to perform and by risking decreasing research quality, has been pointed out previously.30–32
These primarily negative attitudes are also mirrored in the fact that ethical guidelines were of limited relevance to the informants in their actual ethical judgements and decision-making. Instead, they stated that they acted out of experience or moral intuition in ethically troubling situations. This supports previous international findings.23,24
For ethical guidelines to be of any practical value, they need to find their way into practice; thus health-care practitioners must know about them. Apparently, many guidelines were unknown to the physicians and research nurses in our study. The overall message in the interviews seemed to be that there are some advantages in ethical guidelines, but they do not solve the ethical problems or take away the responsibility from the research staff who handle them. Ethical competence is still badly needed, and the questions concerning what this is and how it is achieved still remain.
Almost all informants in our study described ethical competence with reference to personal character. Among the physicians, several personal characteristics were mentioned when ethical competence was to be described. First, being a mature person with a high degree of self-reflection was emphasized. Second, having a humanitarian attitude and being engaged and empathic were put forward. Finally, being a good listener and being sensitive to patients’ needs were mentioned as characteristics of ethical competence in medical practice and research.
The research nurses underlined characteristics such as being loyal to patients, having a strong sense of duty and being honest and telling the truth. Likewise, being good at building a confidential relationship with the patient as well as being good at communicating was mentioned. From a theoretical point of view, the informants seem to express views and aspects common in the virtue ethics tradition. Thereby our results support the findings of Smith and Godfrey, 33 who examined nurses’ perceptions of what it means to be a ‘good’ nurse and found that to a great deal the informants’ understanding of good nursing was consistent with virtue ethics, in that they emphasized personal attributes of the good nurse, such as putting the patient in the centre, and being compassionate, respectful and caring.
Some of the physicians also pointed to the need for a good working climate with an open atmosphere where different problems can be discussed, without leaving people feeling insecure. This means that some of the informants’ answers can be interpreted as their seeing competence as both an individual and a collective skill. This supports previous research, arguing for the management level's responsibility for the development of ethical competence among their staff.8,11
So far we can state that the informants saw ethical competence primarily as character-building, which can be analysed as being in line with a virtue ethics perspective. As in all virtue ethics, the question then arises how such competence and personal character can be learned and trained. 34 According to the results of this study, classes in ethics were of limited value. Instead, the informants pointed out factors such as being raised properly, getting practical experience, having good role models and learning from discussions with colleagues. This means that the respondents in this study saw the development of ethical competence as a continuous process that goes hand-in-hand with learning how to be a (good) human being.
Striking findings in our study are the informants’ criticism of ethical guidelines and the fact that they did not perceive guidelines as valuable in the process of ethical competence-building. The overall impression from the responses is that ethical guidelines in practice are of limited relevance to decisional competence regarding ethical issues. Thereby, ethical guidelines also seemed to play a limited role in the development of a professional ethical attitude towards research subjects. Arguably, the fact that the informants were unaware of the content of many codes and guidelines might impact this position; if they knew more about the guidelines they might use them more. On the other hand, some informants were aware of, and had experienced the problems and limitations of, ethical guidelines and thus seemed to dismiss them based on that experience.
Finally, our interviews displayed that the informants lacked extensive experience of ethical discussions in their workplaces. Discussions did occur, at coffee breaks and sometimes at meetings, but more structured meetings on ethical issues were rare. We argue that this indicates a need for the workplace to create opportunities for this kind of meeting, for example in the form of ethics rounds.11,29 In such discussions, the experience of co-workers and the possibility to see problems from different perspectives could be developed. Ethical guidelines could also be invoked and could be of help in giving structure to the discussions and providing arguments, thereby deepening the practitioners’ knowledge and understanding of them and making guidelines more present in ethical judgements.
Limitations and strengths
Our study was qualitative and we have evidence only of our subjects’ reported experiences and perceptions. As in other qualitative studies with a purposeful sample of informants, there was a risk that informants in our study were selected on the basis of their interest in the topic studied – thereby representing only a subset of the views held by people in their respective groups. Further, the number of informants was low, only 12 persons altogether and six of each category (physicians and research nurses). However, we did include until we experienced that saturation had been reached, and hence we do believe that our investigation has captured significant aspects of practitioners’ perceptions of ethical guidelines and their role in ethical competence-building. In order to confirm the frequency of the reported assumptions, quantitative studies are required.
Conclusion
The research nurses and physicians interviewed had a critical attitude towards ethical guidelines and claimed to make little use of them in practical ethical judgements. Our conclusion is that the production of new such guidelines may be of limited use to ethical decision-making and competence-building among health-care staff working in clinical studies. Instead, the development of ethical competence might be stimulated by letting ethics teachers, employers and producers of various guidelines and position documents focus more on virtues and character, which would tie in with thought patterns already present among professionals. To further ethical competence among medical research staff, the workplace needs to provide opportunities for ethical dialogues. In such discussions, argumentation can improve, virtues can be developed and guidelines can be usefully invoked.
Footnotes
Acknowledgements
We are indebted to the research nurses and doctors who participated in the study and willingly shared their experiences with us. Funding for the study was received from the Bank of Sweden Tercentenary Foundation (Riksbankens Jubileumsfond).