
Abstract
The objective of the study was to explore parental experiences of being offered participation in a previous neonatal research study involving venepuncture. The method employed was a questionnaire-based exploration of parents' attitudes in those approached to participate in a study of term and preterm immunization responses (Preterm Immunisation Study [PREMIS]). We explored experience of the initial approach, knowledge of study, venepuncture and views on research ‘in general’. In all, 59% of families responded. Highest response rates were for those participating in PREMIS (87% term/69% preterm) and lowest in decliners (34% and 35%). Responding parents participating in PREMIS were well informed, positive about research and did not find the venepuncture problematic. Sixty percent of responding parents who declined PREMIS attributed their declining to the need for venepuncture. In conclusion, parents participating or declining a neonatal study involving venepuncture are different, but participating parents were well informed and seemed able to judge that participation was right for them such that in consenting families venepuncture itself is not problematic.
Introduction
The Royal College of Paediatrics and Child Health (RCPCH) of the UK has categorized the risks of research-related procedures for infant or child research participants as ‘minimal’, ‘low’ or ‘high’. 1 Procedures such as lavage (washing out of the airway in ventilated infants to obtain samples) and venepuncture (taking a blood sample from a vein), which are invasive and involve some risk, are according to the RCPCH definitions low risk. Research that exposes infants or children to more than a minimal risk requires ‘serious ethical consideration’ if they might expect ‘only slight, uncertain or no benefit to themselves’. Despite this call for reflection, studies assessing how parents experience their involvement with research, and its impact upon their children, are limited. Some data are available describing parental views of high-risk, invasive, research-related interventions in critical or serious situations. 2,3
A small body of evidence on parents' views of research-related venepuncture exists; most studies consider the impact of the procedure, assessing intensity and duration of upset, with varying results. 4–7 They generally do not consider the broader range of issues that might be associated with research-related venepuncture, such as whether the purpose of a blood test is clear, whether parents feel that the aims of the study warrant venepuncture or how acceptable it is in healthy children with little chance of benefit to themselves.
This lack of information may itself have a direct impact on research if, for instance, concerns around such acceptability prove to be an obstacle to research ethics committee (REC) approval or to parental consent for the inclusion of their child in a study.
In order to address some of the shortfall in relevant data in this area, the views of parents who were offered participation in research involving venepuncture were sought and explored via a questionnaire study, referred to throughout this paper as PAREX (a study of PARental EXperiences). All parents who were eligible for this questionnaire study had previously been asked to consider enrolling their baby in a study that included venepuncture – the Preterm Immunisation Study (PREMIS). 8 Fifty-seven percent had agreed to participate in this study and 43% had declined.
Methods
PREMIS and the development of the questionnaire
PREMIS was designed to assess antibody levels to routine immunization in babies <32 weeks gestation 8 by two blood tests, one before (at 8 weeks of age) and one after (at around 24 weeks of age) completion of the routine childhood immunization schedule. Preterm infants may respond suboptimally to these immunizations and then remain at risk of a significant childhood illness. 9–12 For methodological reasons PREMIS required a term control group, but these individual term infants were not at the time considered to be at extra risk of immunization ‘failure’, and were simply acting as controls for the preterm group. All study infants (term and preterm) received their primary immunizations as per standard UK practice, had antibody levels measured in blood taken before and after completion of the primary series and, if necessary (based on antibody levels achieved), were offered a booster dose of vaccine (with an optional further blood test thereafter). The timing and number of blood tests required was explicit in the parent information leaflet.
At the time of application for ethical approval for the PREMIS study, REC representatives suggested that the use of venepuncture in healthy term babies was problematic since these infants had little chance of personal benefit, and after REC consultation the term comparison group was restricted to 50 infants.
This concern by REC over the use of venepuncture, the experience of recruiting infants into the PREMIS study and the experience of carrying out their venepunctures led to the development of a questionnaire to allow parental feedback on their experiences.
In order to contextualize the results of the questionnaire study, an understanding of the PREMIS study is necessary. Full details are available in the initial publication of the antibody data; 8 however, a summary is given below for ease of understanding the following information. Although study interventions were not different between term and preterm groups, the parent information leaflets and approach to parents were different due to their different circumstances and differing roles in the study. Parents of preterm babies (all <32 weeks gestation at birth) were approached while their babies were still inpatients approximately four to six weeks after delivery and invited to participate. Parents had until just before the eight-week immunization to make their decision. Parents of term babies were approached on the postnatal wards prior to discharge, usually one or two days after delivery. Their time to deliberate their decision was 24–48 hours to fit with patterns of discharge and to minimize loss to the study. Oral and written information was given (written information available from the corresponding author if required).
Blood samples were taken in the neonatal intensive care unit or at home, with parent(s) present if they wished. For most preterm infants, their preimmunization sample was taken while they were still in the neonatal unit, and if possible (and for most preterm preimmunization samples) this was taken alongside other routine tests. All term preimmunization samples (except one that coincided with the need for a haemoglobin check) were taken specifically for the study. All postimmunization samples (preterm and term) were specifically taken for the study. Anaesthetic cream was used where appropriate (as per licensing, in infants over 1 month of age and at parental request), and parents were told verbally of its possible use at the time of consenting to (or declining) the study. At the time of the study, sucrose administration for analgesia during venepuncture was not routine. All study samples were taken using the same venepuncture method: none was taken by heel prick. For all infants, if the antibody levels to one specific antigen (Haemophilus influenzae type b [Hib]) were low, a Hib booster was offered. Such efficacy data for individuals are not ordinarily available, and was a potential perceived parental benefit for all babies who joined the study, but one which might have been more expected by the parents of a preterm study infant since at the time of the PREMIS study there was no concern about term babies' immunization responses, in contrast to the preterm population. 10–12
A total of 384 families were approached for participation in PREMIS – term infants were approached and recruited between March and July 2002, and preterm infants between February 2001 and July 2002. Overall 220 families consented and 164 declined, giving an overall consent rate of 57%. This rate differed significantly between parents of the preterm and term babies (Figure 1) (χ 2 = 141, P < 0.001) – we approached proportionately many more parents of term than preterm babies. The questionnaire study provided the opportunity to explore the issues involved.
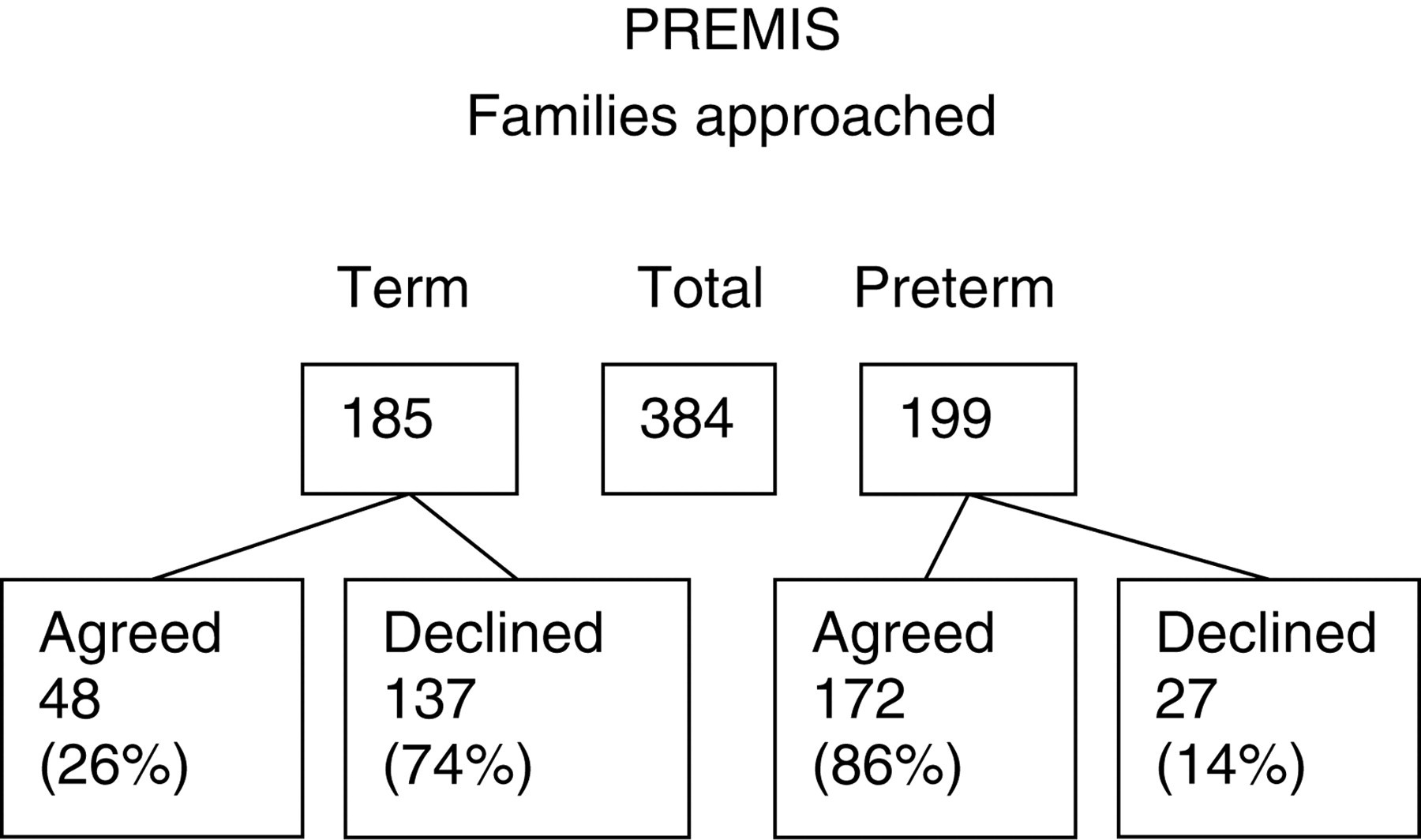
Families approached for PREMIS study. PREMIS = Preterm Immunisation Study
Questionnaire study methodology
All 384 families approached for PREMIS were eligible for the questionnaire. Permission to contact families was sought from their general practitioner (GP), as a requirement by REC for approaching families who are currently not in contact with the research group. In 80 cases, contact was not possible either because the GP declined, the family was not known to the GP or no response was obtained from the GP; the remaining 304 families (159 preterm, 145 term) were sent a letter explaining the questionnaire study and the self-administered questionnaire. A full copy of the questionnaire is available from the corresponding author. The same questionnaire was sent to all – term and preterm and participants and decliners of the PREMIS study, but some questions were clearly not appropriate to be answered by decliners (such as those focusing on the experience of having a blood test as part of a study). The questionnaire included structured questions, modified Likert scales and open questions to elicit parents' views, and recollection of: immunization, the aims, methods and recruitment processes of the PREMIS study, the use and impact of the venepuncture, and general views on research in babies. Both parents received their own copy of the questionnaire (but an assumption was made that both parents resided at the same address). They could reply separately or together, and were asked to indicate whether the response represented individual or joint views. Replies were via enclosed stamped addressed envelopes, anonymous, but coded by secretarial staff to allow a single reminder to be sent to non-responders. The initial approach to parents with the postal questionnaire was in February 2003 to all parents.
Statistics
Statistical analyses presented below are on all responding to the PAREX questionnaire and involve two main explanatory categorical and non-exclusive variables: whether a baby was born preterm or at term, and whether PREMIS was accepted or declined. Statistical analyses used the χ 2 test, with Yates' correction or Fisher's exact test where appropriate.
Ethical approval
PAREX was approved by the Northern and Yorkshire MREC in September 2002.
Results
Response rates
In 151 cases one parent returned the PAREX questionnaire, and in 28 cases questionnaires were returned by both parents, resulting in 207 questionnaires for 179 cases, an overall family response rate of 59% (Table 1). There were clear patterns in the response rates to the questionnaire: those who participated in PREMIS were much more likely to respond (Figure 2). Among questionnaire respondents, significantly more of the parents of term than preterm babies (48% versus 22%), and more of those who had declined to participate in PREMIS than had consented (47% versus 29%), had received education beyond the age of 18 (χ 2 14.6, P < 0.001; χ 2 4.78, P < 0.05). These two facts are not independent however: it is well recognized that level of education and risk of preterm delivery are associated, and most declining parents represented in the questionnaire study were of term infants.
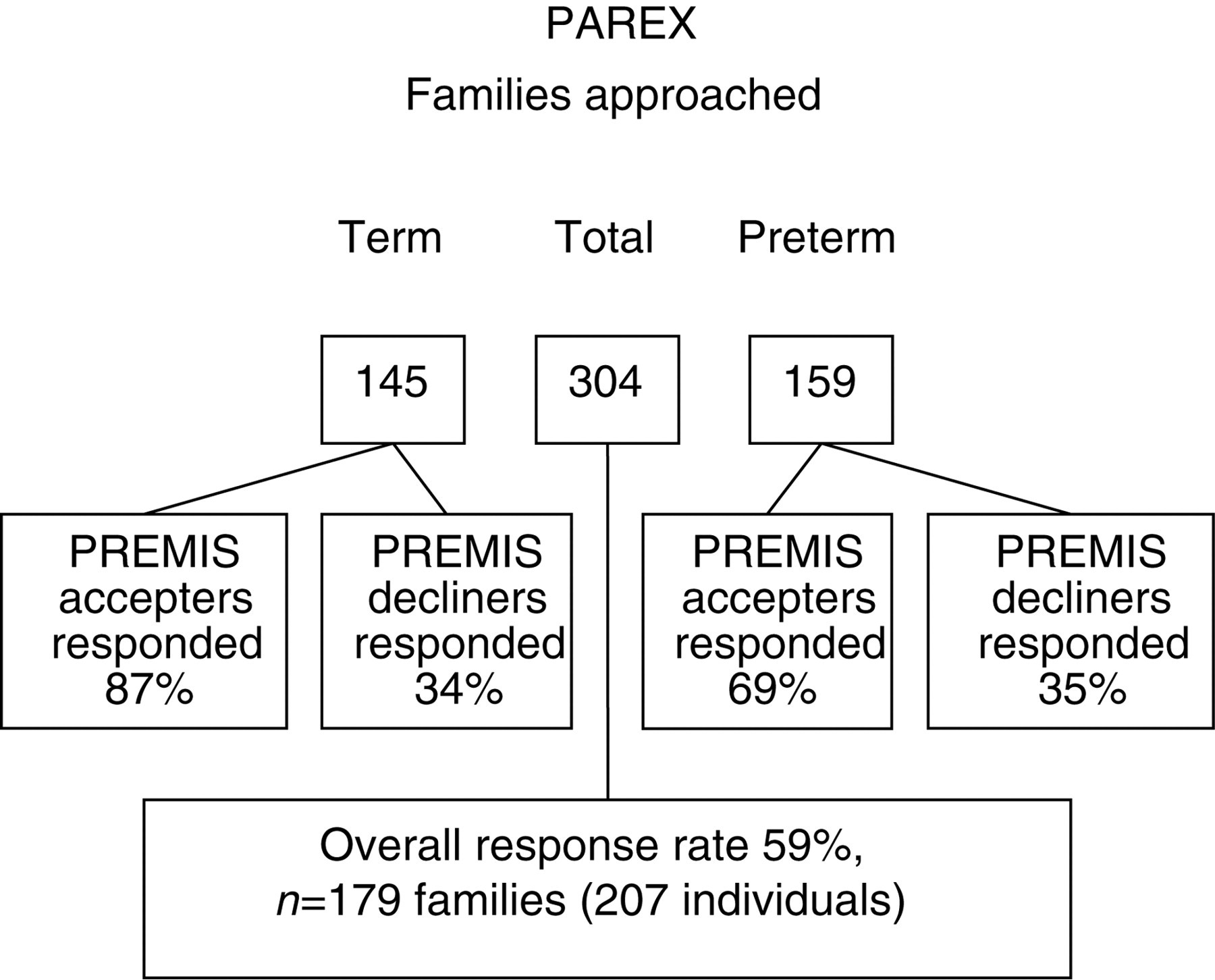
Families approached for PAREX study. PAREX = PARental EXperiences
PAREX Respondents
PAREX = PARental EXperiences; PREMIS = Preterm Immunisation Study; IQR = interquartile range
Views of immunization
Most (91% preterm and 94% term) infants were fully immunized. For those that were not, in each case parents had elected not to have the MMR (measles, mumps, rubella) vaccine.
Parents were asked to complete the statement, ‘I think vaccinating babies is —’ from multiple-choice responses, indicating their views in principle, and any qualifying concerns. Ninety-seven percent of all parents felt that vaccinating babies is ‘a good idea’ (Table 2). Parents of preterm participants showed the highest rate of unqualified support (55%). Where parents qualified their support it was almost entirely in relation to concern over the possibility of side-effects rather than pain, most common in term participants. All free comments expanded on worries over the MMR vaccine.
Responses to the question ‘What do you think about vaccinating babies?’
PREMIS = Preterm Immunisation Study
Views on the recruitment processes for PREMIS
Most (but not all) parents of term and preterm infants were approached for participation by the study lead (JEB). All were given written and verbal information. Overall, 88% indicated that they did ‘get a chance to read’ the parent information leaflet; parents who declined to participate were less likely to have done so than those who consented (59% versus 93%, P < 0.05). Most felt that it was ‘easy to understand’ (92% PREMIS participants, 85% of decliners). Most (78%) indicated that they had ‘an opportunity to talk to the researcher’. Cumulatively, 98% of consenting parents felt that the approach was done well (74% ‘very well’, 24% ‘quite well’). Fewer, but still a substantial majority of, parents who declined also cumulatively felt that the approach was done well (71%), but their support was more tempered (30% ‘very well’, 41% ‘quite well’). Significantly more of the parents of term than preterm babies who consented to PREMIS viewed the recruitment process in the most positive way (done ‘very well’) (χ 2 4.0, P < 0.05), but the greatest difference in perspective occurred within the parents of term babies: 85% of those who consented viewed the process most positively, compared with only 30% of those who declined (χ 2 25.0, P < 0.001) (Table 3).
Responses to the multiple-choice question ‘I thought the recruitment process was done …’
PREMIS = Preterm Immunisation Study
Knowledge of PREMIS
The questionnaire asked parents about the purpose of PREMIS. The aim – to assess vaccine efficacy – was identified by almost all consenting parents but by less than half of those who declined (χ 2 72.7, P < 0.001). The term parents who consented to PREMIS were as well informed as the consenting parents of preterm babies (Table 4).
Correct identification of vaccine and vaccination policy-related facts
PREMIS = Preterm Immunisation Study
Parents were asked four questions on the implications of taking part in PREMIS. For each question, the correct responses were identified significantly more often by parents who consented to PAREX than by those who declined. These questions asked whether the study altered timing, type or number of vaccines (it did not) (χ 2 46.5, P < 0.001; χ 2 25.9, Fisher's exact test P < 0.001, respectively), and number of blood tests (increased by the study) (χ 2 57.5, P < 0.001). Of note, less than half of the parents who declined to participate identified that PREMIS involved venepuncture (43% compared with 97% of participating parents) (Table 5).
Correct identification of PREMIS-related facts
PREMIS = Preterm Immunisation Study
The PREMIS venepunctures
The questionnaire explored the role of venepuncture in the decision to decline participation, and reactions to venepuncture for participants. Parents were asked ‘Was the thought of the blood tests a problem?’ and could reply either – yes and I refused the study; yes, but I did not refuse the study; or not a problem at all. Although the majority of those who declined attributed their decision to the requirement for blood tests, fewer expressed this view than might have been expected (57% of preterm decliners and 60% of term decliners). This figure is, however, greater than the number of declining parents who indicated that they were aware that PREMIS would involve blood tests (n = 17, 43%) (see Table 5), suggesting a degree of confusion on this subject among this group of parents, which may relate either to the format of the question, or to the time between receiving study information and the questionnaire.
For PREMIS participants, the actual experience of venepuncture was assessed by two structured questions as well as opportunities for free text. Most said that they and their baby were either ‘fine’ (31% baby, 47% parent) or ‘a little upset’ (56% baby, 37% parent). There were many free text comments relating to the blood sampling. Some were positive, for instance: ‘I expected it to be a lot worse’, ‘study doctor very gentle and had no trouble taking blood and that helped me keep calm’ and ‘apart from a virtual blood test I don't think it could be done better’. Some indicated that there were difficulties, for instance: ‘I found it quite hard to calm him when I was also getting upset’, ‘when my son cried I just wanted them to stop’ and ‘it was very upsetting to see your baby getting blood tests – I don't think anything can change that’. Asked specifically whether anything could be done to make the blood sampling easier, 23 parents said ‘nothing’ or ‘no’ and 17 parents of the preterm babies acknowledged that venepuncture is difficult due to the size of preterm babies or ‘difficult veins’. Several parents felt that doctors vary in terms of sympathy and level of skill at venepuncture and one suggested that only senior doctors should take blood from such small babies.
Uptake of the booster
Although now part of the standard childhood immunization programme in the UK, at the time of the study a booster Hib vaccine was only potentially available via PREMIS; we therefore wished to know how this was viewed, especially by parents who declined to participate. We asked ‘If you were told that your baby's vaccinations had not worked would you want an extra top-up vaccination (a booster) for your baby?’ Almost all of those who consented to PREMIS (96%) indicated that they would want a booster; significantly fewer (52%) of the declining parents were interested in this option (χ 2 55.4, P < 0.001). There was greatest uncertainty among the parents of term babies who declined, with 24% indicating that they were ‘Not sure’ about taking up a booster.
All 97 babies (82 preterm, 15 term) who showed insufficient immunity were offered a booster; in 61 cases (55 preterm, 6 term) parents both accepted the booster and permitted a further venepuncture; the other 36 accepted the booster but declined further blood testing.
Views of research
Parents were asked for their views on neonatal research. Consenting parents were the most positive, 86% feeling that ‘It is a good idea, more should be done’, compared with 50% of parents who had declined (χ 2 25.6, P < 0.001). Among the parents of the term babies, notably fewer of those who had declined expressed enthusiasm for research involving babies (54% versus 92% of PREMIS participants) (Table 6).
Parental views on medical research in infants
PREMIS = Preterm Immunisation Study
Twenty-three percent of consenting parents felt that participating in PREMIS had positively changed their views of medical research; this was also reflected in entirely positive free text comments, such as, ‘it was a privilege’, and ‘more aware of how important research is’. Some suggested altruism; ‘we made the decision to help future babies’, ‘we were glad we were asked to join – it is nice to put something back’.
Discussion
The original immunization research study, PREMIS, is an example of research that may benefit a broad population of children, but there were challenges: it required all participants to undergo venepuncture and (especially for term babies) was likely to be non-therapeutic.
Even with a much-reduced sample size of term babies, accrual was problematic. Parents of term and preterm babies responded to the immunization research very differently, reflected in their differential consent rates.
PAREX showed experiential, attitudinal and demographic factors affecting this. Of the parents who chose to return a questionnaire, those consenting to PREMIS were more likely to have had a preterm baby, be positive about neonatal research, were more knowledgeable about the study and were less likely to have been educated at a higher level. The blood tests were not a particular worry. Those who declined PREMIS were most likely to have had a term baby, were less positive about neonatal research, were less knowledgeable about PREMIS and were more educated. Fifty-nine percent cited the venepuncture as the reason for their decision. Apart from the level of education, these associations appear to be a product of recent events. It is likely that they arose predominantly in relation to two influential areas: the timing of the birth of their baby and subsequent related experiences, and the different recruitment processes used for PREMIS.
The high preterm consent rate for PREMIS (86%) adds to accumulating data suggesting that parents of sick babies within neonatal intensive care respond to neonatal research in a largely uniform way. At the time of crisis, parental autonomy can be severely compromised, leading to lower levels of engagement with the details of neonatal research and high levels of compliance, 13 a view supported by studies of parental knowledge and understanding of the trials to which they have consented. 2,14–17 A heightened sense of the need to protect a vulnerable baby and a desire for a solution are among the factors leading to a very rapid, potentially compromised, decision-making process. 14,16,17 Although PREMIS was conducted in the aftermath of a crisis, rather than as events around delivery were unfolding, it still produced a high consent rate among parents within neonatal intensive care, possibly suggesting that such experiences exert a persistent rather than a transient effect on responses to neonatal research. The relationship that is established between carers of preterm infants and their parents may also have had a beneficial effect on recruitment rates among preterm infants, since the study lead was also involved in clinical care delivery for the preterm infants. Venepuncture itself, a factor in term refusal, may also be less problematic for families of preterm infants where this procedure has both been seen and understood, and potentially become ‘routine’.
The positive views of research with babies expressed by parents of preterm infants may also come from a sense of empathy with the broader population of preterm babies and their families. The relevance of the research to their own situation may have led these parents to consent to PREMIS in such high numbers. There is no suggestion in the PAREX data that these parents consented through over compliance and without the relevant facts to hand.
In contrast, PAREX suggests quite clearly that for most parents of term babies the same degree of sympathy for research does not exist, and 74% declined participation in PREMIS (contrasting with 14% of preterm parents). The (separate) term parent information leaflet explicitly stated that ‘We need to establish what response normal healthy babies have to their vaccinations to allow us to compare preterm babies to this. Your baby is a healthy term baby (born after more than 37 weeks pregnancy) and could help us with this information’.
For these parents, under these circumstances, venepuncture was problematic, and was directly expressed as the reason for study refusal by 60% of refusing term parents who completed the questionnaire. The availability of the booster was also less important for term parents, who may have (rightly) been influenced by the fact that the existing data suggested that term infants were unlikely to require a booster, whereas preterm infants might. Different recruitment pathways may also be important – specifically the contracted time-frame for term parents to consider their participation, since the first few days after delivery can be a time of fatigue, pain, great change and high emotions. In addition, and in contrast to the preterm infants, the parents of term infants lacked any previous personal involvement with the research team.
Not all parents of term infants reacted to the approach for participation in the PREMIS study in this way. The views expressed by the minority of parents of term babies that did take part made it clear that they both had a different perspective on neonatal research and were well informed of the study aims and requirements. Almost all expressed approval of research involving babies, and were motivated to lend their support to a further, related study of their views. They were the group that was most likely to go on to reply to the questionnaire, and the PAREX study achieved a highly representative sample for this subgroup. They were positive about the recruitment process despite the lack of a pre-existing relationship with the recruiting medic, and had engaged fully with the immunization research, its background, aims and key features. They did not feel that their babies had been harmed by the venepuncture, which was central to the study.
Although the consent process appeared to contribute to differential recruitment rates for PREMIS, it also proved to be highly effective in ethical terms. It resulted in a study where those who had given their consent were knowledgeable and supportive of the research. Those who had withheld consent were less persuaded of the research and were somewhat less knowledgeable, but crucially had clearly felt able to reject the study. Studies with differing target populations may need both differential recruitment material and strategies.
Where research-related risk is low, as for venepuncture, it is easier to take a more flexible position on what might constitute therapeutic or non-therapeutic research, but what is needed is a model that can take into account the wide variety of research situations that exist. The confluence of PREMIS and PAREX certainly suggests that further reflection of the development and management of research studies with very different populations, and those that operate at the boundaries of ‘therapy’, is highly appropriate.
Conclusion
We have presented in detail the views of participating and non-participating parents in a neonatal study that included venepuncture, and demonstrated that parents who perceived that they or their baby would be upset by venepuncture declined the study. Parents who consented to the (PREMIS) study understood both the aims and processes of the study and for them the venepuncture itself was of minimal impact. We hope that this information may assist research ethics committees considering the acceptability of (apparently) non-therapeutic interventions.
This study has also shown that differentiating a therapeutic study from a non-therapeutic one is not easy, and indeed may be viewed differentially by consenting parents. Researchers may find that differential approaches to different groups of potential study participants may be helpful in ensuring that parents are in the best possible position to know whether or not participating in a study is right for them.