
Abstract
Acceptance of elderly or marginal health individuals as kidney donors is debated, with practices varying between centres. Transplant recipients, live kidney donors and health-care professionals caring for patients with renal failure were surveyed regarding their views on live donor kidney transplantation (LDKT) of marginal health (diabetes, hypertension, atherosclerosis, obesity, etc.) and elderly donors. Participants were recruited within a tertiary renal and transplant centre and invited to participate in focus groups and structured interviews. They also completed an anonymous questionnaire. Of 464 participants who completed the questionnaire (36% health-care professionals and 64% patients), 49% and 64%, respectively, stated that marginal and elderly donors should be accepted for LDKT. In the structured interviews, emphasis was given to presenting to donor, recipient and their respective families a calculated risk regarding the effect that either a nephrectomy or transplant has on long-term quality of life. Participants stated that an independent third party in addition to the transplant team should discuss involved risks. Issues of ‘how desperate’ the recipient's situation is should also be considered. Health-care professionals stated that regardless of the strength of will of an individual to donate a kidney (despite age, health problems or personal risk), they should always have the right to say ‘no’ if performing a specific LDKT was against their professional and ethical values. About half of those surveyed considered that marginal health and elderly donors were acceptable for LDKT. Emphasis was given to the explanation to donors and recipients of the risks involved in such transplantation.
Introduction
The first successful kidney transplant from a live donor was performed almost 50 years ago. 1 The acceptance of elderly or marginal health individuals as potential kidney donors is under debate, with practices varying between centres. 2,3 Most would reject potential donors aged over 65 years as well as donors with marginal health problems such as borderline hypertension or obesity. However, the number of patients on dialysis and transplant waiting lists increases every year. 4 Thus, the number of available kidneys for transplant might increase if more live donors were accepted. A way to increase the live donor pool would be to accept elderly (aged over 65 years) yet healthy individuals as well as marginal health live donors.
It has been suggested that the age of a donor of over 55 years negatively affects the one- and five-year graft survival rate. 5,6 Grafts from older donors may display tissue inflammation at the time of procurement that may increase immune recognition. 7 There are changes associated with age in the number and size of glomeruli, a progressive decrease in glomerular filtration rate (kidney function) as well as increased immunogenicity of the aging kidney. These data seem to contradict those who advocate that physical age does not count and biological age of the donor should be the criterion to proceed with the transplant.
The use of marginal health donors has been associated with a worse outcome when compared with ideal donors. 8–10 Most transplant teams 11 will not accept a donor with hypertension since, according to the Swiss registry, 12 these donors require three times more medication than those who develop hypertension after donation. Yet studies show that using kidneys from marginal health donors improves patients' quality of life 13,14 with an associated benefit in life-expectancy when compared with maintenance dialysis. 8,15
The aim of the present study was to survey the views of health-care professionals and patients within our transplant centre, one of the largest in the UK, on these issues. The definition of marginal health donors is according to the British Transplantation Society guidelines, 16 which also form an integral part of current practice in our department.
Materials and methods
The project was approved by the Harrow Research Ethics Committee, as well as the R&D department of Hammersmith NHS Trust. The study participants comprised:
medical staff (consultants and trainees) of the West London Renal and Transplant Centre (WLRTC); nursing staff of the same centre and its satellite haemodialysis units; patients on dialysis (haemodialysis or peritoneal dialysis) in the WLRTC and its satellite units; patients with a functioning cadaveric kidney transplant, followed up in the outpatient department of WLRTC; patients with a functioning live donor kidney transplant followed up in the outpatient department of WLRTC; live kidney transplant donors followed up in the outpatient department of WLRTC.
The first phase of the study was conducted by inviting participants to complete a questionnaire. The questionnaire had two parts – the first about basic demographic information of the participants and the second the ethical issues pertaining to live donor kidney transplantation (LDKT) (see Appendix).
The questionnaire was anonymous and confidential with time for completion being 10–15 minutes. Not only was this a prerequisite to obtain approval from the ethical committee but also the participants of the study would probably answer more frankly with no fear of revealing personal thoughts. It was based on a thorough literature search as well as on the questions on ethical issues faced in everyday clinical practice by members of staff in the WLRTC regarding LDKT. It was piloted previously and formed part of a questionnaire used previously by the authors. 17 The questions involved acceptance or not of marginal health or elderly donors. There were extensive discussions with various members of the unit and the questionnaire was revised taking their comments into consideration. The questionnaire was also presented to our local clinical ethics committee meetings taking into account the advice of experts in medical ethics. The questions were presented as objectively and neutrally as possible; however, we have to take into account that the participants of the present study have had experience with LDKT and the procedures involved.
All participants received an information sheet explaining the study, a consent form to sign and the questionnaire. They were also given two prestamped envelopes (one for the consent form and the other for the questionnaire) with the address of the chief investigator for return via mail. The forms were distributed in departmental meetings for medical and nursing staff, outpatient departments, dialysis units or were sent to patients at home. Participants were encouraged to contact the chief investigator with any queries; his contact details were included in the information sheet. Having two separate envelopes and the fact that non-responders were not chased up achieved anonymity. Obviously it was impossible to chase non-responders since all responses were anonymous.
The second phase of the study was based on structured interviews within focus groups. Each participant invited to complete the questionnaire was also asked in the consent form whether he/she was willing to participate in a focus group. The investigators performed selection randomly using computer software. The aim of the interviews was to obtain valuable information regarding the reasoning for the selected choices in the questionnaire. Thus the discussion during the interviews was based on each topic raised in the questionnaire. Two investigators conducted the interviews, one organizing the discussion and the second taking notes. We avoided recording the interviews since this might discourage participants to speak freely. All the definitions used in the questionnaire and discussions were based on the British Transplantation Society guidelines on LDKT.
16
In total, 12 focus groups were formed (4–6 participants in each group). In detail the number of focus groups according to every category was as follows:
doctors: 2 focus groups (12 participants in total); nurses: 2 focus groups (11 participants in total); live donors: 4 focus groups (16 participants in total); live and cadaveric donor recipients: 2 focus groups (8 participants in total); dialysis patients: 2 focus groups (8 participants in total).
The only category that contained double the number of focus groups was ‘live donors’ since their role in LDKT is paramount and thus the arguments presented by them in the discussions would be of special interest. The validity of qualitative analysis depends on the number of arguments presented and their variability; therefore, it is not affected by the different number of participants in the focus groups.
Statistical analysis of the quantitative phase was performed by entering the data into a Microsoft Excel 2003 spreadsheet with results expressed as percentages. Then participants were divided into health-care professionals and patients and the results compared with the chi-square test. P ≤ 0.05 was considered statistically significant.
An exploratory qualitative approach using ‘grounded theory’ methodology 18 was used, as is appropriate when very limited pre-existing information is available. 19 The grounded theory is a systematic qualitative research methodology used in the social sciences, emphasizing the generation of theory from data available. Grounded theory has the goal of generating concepts that explain people's actions regardless of time and place. From the data collected, the key points are marked with a series of codes, which are grouped into similar concepts and categories that form the basis for creation of a theory. Thus according to the grounded theory, data collected during the qualitative phase of the project (interviews) consisted of coding the arguments and ideas in relation to the questions of the questionnaire. Categories containing these arguments were formed and the most representative phrases for each argument were included in tables; e.g. acceptance or not of elderly live donors. The deontological or utilitarian element between each argument was identified and examined under the prism of the four principles in medical ethics: respect to autonomy, beneficence, non-maleficence and justice. An effort was also made to identify the basis of each argument, such as religious belief, cultural background, emotion, knowledge, altruism, expectation of benefit, spontaneous reaction, etc. Data collected through the two phases were triangulated in order to enhance validity and reliability. 20
Results
General (quantitative) analysis
Of the 1105 questionnaires distributed, 464 were completed, constituting a response rate of 42%. There were 248 women and 216 men, and the majority (48.1%) were aged 31–50 years (Table 1). Most participants were married; other demographic data are presented in Table 1. Participants were of different religions and ethnicities but the majority were, respectively, Christian (62.1%) and British (48.5%) (Tables 2 and 3).
Demographic data of participants
Religion of participants
Ethnic origin of participants
The participants comprised recipients of live kidney grafts (14.4%); recipients of cadaveric grafts (8.8%); live kidney donors (14%); medical staff, with similar numbers of trainees (6.7%) and consultants (6.5%); nursing staff (23.1%); and other participants such as relatives (1.1%). Of the patients, 25.4% were on dialysis (86% on haemodialysis, 12% on peritoneal dialysis, 2% not answered), 38% had never been transplanted before, 18% had undergone at least one kidney transplant and 44% did not answer.
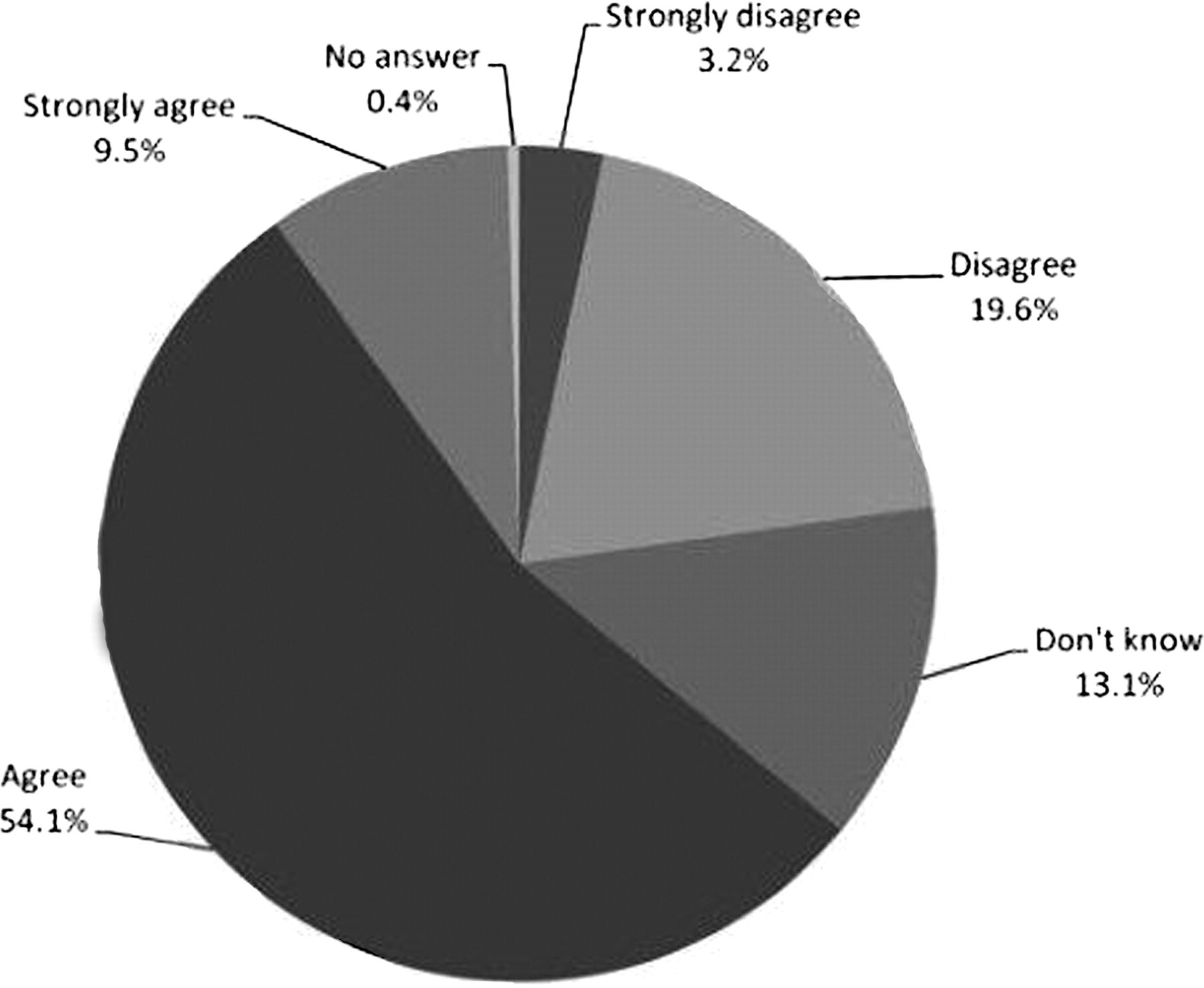
Most participants (48.8%) advocated that potential donors with marginal health problems such as borderline hypertension or obesity, who are adequately informed and prepared to take the risk, should be accepted as potential donors (Figure 1) including participants who either ‘agreed’ or ‘strongly agreed’ with such an idea. A third of participants were reluctant to accept such a potential donor. It is noteworthy that higher percentages of participants aged over 50 years were prepared to accept high-risk donors. Specifically, 97/153 (63.4%) of the 51–70 year group and 24/36 (66.7%) of the 71–90 year group agreed or strongly agreed with accepting such patients for donation.

Acceptance of donors with marginal condition of health
A strong majority (63.6%) supported donation by elderly donors (over 65 years old) if they were adequately informed and prepared to take the increased risk (Figure 2). One participant thought that an elderly potential donor should be allowed to donate according to the recipient's age. If the recipient is over 60 years old, he/she should be allowed to donate but if the recipient is under 60 years old he should not be allowed to donate. Participants over 50 years old were even stronger supporters of elderly donation: 103/153 (67.3%) of the 51–70 year group and 25/36 (69.4%) of the 71–90 year group agreed or strongly agreed with accepting elderly donors.
Acceptance of elderly donors (over 65 years old) for donation
More patients (n = 296) compared with health-care professionals (n = 168) were prepared to accept (76.3% versus 56.5%) potential marginal health donors (P < 0.0001). However, health-care professionals would accept at a higher percentage (69.7% versus 60.1%) potential donors over 65 years of age (P = 0.0408).
Qualitative analysis
Most participants stated that elderly and borderline health condition donors should be accepted if ‘they are well-informed and prepared to accept the extra risk’. Obviously, they believe that respect to donor's autonomy is paramount and because probably of personal belief and cultural background, as many stated, the donor should be free to accept voluntarily an increased risk for such a donation. Another suggestion was that acceptance should be approved if the ‘recipient is willing to accept a kidney from such donors’ or ‘according to how desperate the situation of the recipient is’. Both these ideas represent the respect to the recipient's autonomy and free will as well as beneficence for the recipient. The basis for these arguments lies probably behind the expectation of benefit for the recipient, thus underlining a utilitarian element behind these ideas. However, there were participants, mainly health-care professionals, stating, ‘donors with medical problems are very persistent to donate but sometimes health-care professionals might have to say no’ or ‘sometimes donors do not realise future risks, like smokers do not realise the effect of smoking on their health, thus the transplant teams should make this decision’. The ethical principle behind those statements is non-maleficence from the health-care professional's point of view based on knowledge and professional experience as well as respect for their autonomy. They are obviously deontological arguments in order to protect the donors from increased risks.
Discussion
LDKT is the treatment of choice for end-stage renal failure (ESRF). However, there are many associated ethical issues, which are intensely debated. Our aim was to construct a questionnaire to survey views of individuals involved in kidney transplantation and dialysis. We achieved a satisfactory response rate in order to extract valid results. 21 Furthermore, by dividing these respondents into focus groups we managed to address the rationale behind the answers in the questionnaire.
Our study demonstrated that many participants support the acceptance of donors with marginal health status, strongly believing in the donor's autonomy as mentioned earlier. On the other hand, we should also respect the transplant team's autonomy regarding the choice of donors as there is an ethical obligation to solve medical problems and not create new ones. We firmly believe that every case should be evaluated and assessed individually. The evaluation of such cases is performed by an independent clinical party, providing the donor has agreed to donate after acknowledging risks involved. One could argue that the risk of nephrectomy for an elderly donor or for a borderline hypertension patient cannot be quantified exactly, since data are scarce, thus making adequate information for such donors impossible. However, such potential donors could certainly be informed that they are at higher risk for postoperative complications compared with younger or healthier donors. In our opinion, the transplant team has an obligation to balance risks and benefits, attempting to minimize the former and maximize the latter, for the donor's and recipient's sake.
In the structured interview there were controversial suggestions as to who should assume responsibility for allowing donors to donate: the transplant team or the donor.
Donation by marginal health donors
In a survey performed in the USA, public opinion supported donation by donors at added risk. 22 Patients with ESRF should have the opportunity, with informed consent, to choose to continue waiting for an ideal graft or receive a marginal kidney from a live donor. Strategies have been suggested 15 to improve the function of a marginal kidney, referring both to deceased and live donors, such as reduction in cold ischaemia time, delay in the initiation of calcineurin inhibitors until renal function is satisfactory and the transplantation of such organs in a healthy population over 60 years old (old-to-old programme). More recently the belief that moderate blood pressure, adequately treated, as an isolated medical abnormality, poses little risk to a patient's renal function and has led some centres to accept such individuals as potential donors. 23 Excluding donors with demonstrable diabetes is universally accepted among transplant centres. 24
Studies emphasize obesity as a main factor in progression of some forms of glomerular disease 25 as well as increasing the prevalence of proteinuria and renal insufficiency in patients who have undergone nephrectomy. 26 Epidemiological data have demonstrated that time-dependent risk on renal function is greater for obesity than hypertension. 27 The imbalance of nephron mass between donor and recipient in cases of significant differences in body mass index has been discussed as a non-immunological factor for deterioration of graft function. 28 Moreover, obese patients have a survival advantage on dialysis compared with non-obese, 29 yet authors have discovered that transplantation offers obese patients a survival advantage over dialysis 30 and 3-year graft and patient survival for the morbidly obese is similar to the non-obese. However, obesity leads to more complications and requires more days in hospital. 31 These reasons may not be enough to deny morbidly obese patients the survival and quality of life advantages of renal transplantation. Recent research shows that elevated donor cholesterol levels are associated with inferior graft function, probably due to renal microvascular or glomerular injury caused by chronic hyperlipidaemia. 32 Thus, careful donor selection is required prior to transplantation.
Donation by elderly donors
In this survey, most participants accepted elderly people (over 65 years old) as potential donors. In a previous study, 17 67.6% of health-care professionals agreed with accepting elderly people as live donors, a percentage which is similar to the present study. We believe that although physical age is important, it does not always reflect functional status of an individual's kidney. Our view may be supported by questioning why using certain age limits, such as 65 or 70 years old, is reasonable, as this might be interpreted that a kidney of a 64-year-old individual is appropriate for donation while that of a 66-year-old is not! In our opinion, the ‘biological age’ of the donor and the functional ability of a potential donor's kidney should be the most important criterion for donation. The result of our survey seems to support such a view. However, in order to satisfy those who argue that kidneys from older individuals have a shorter life span or decreased functional reserve, we suggest that they can be donated to older recipients, so removing them from the transplant waiting list and increasing indirectly the position of younger patients on that list.
Cameron 33 advocated that there are neither medical nor ethical grounds for excluding from renal transplantation those aged under 70 or even 75 years of age, with elderly living donors having an important place in LDKT programmes. The difference between the donor and recipient age seems to play a decisive role in patient outcome. 34 Other researchers have not found any difference in graft survival according to the donor age. 35 As mentioned earlier, the majority of centres (94% in France) 3 avoid using donors aged over 65 years. However, one-year graft survival of organs from donors over 60 years is comparable to kidneys obtained from younger donors with a similar incidence of acute tubular necrosis. 36 This has led many US transplant programmes to extend their upper age limits for acceptable donors and many have ‘no upper limit’. 37 In one study no significant difference was found in the two-year graft survival rate of kidneys from older donors (over 55 years of age) transplanted into younger or older recipient age groups. 38 Furthermore, other researchers 39 discovered that transplantation of kidneys from older donors (over 60 years of age) led to better patient survival rates in older recipients (over 60 years of age) than in younger ones (under 60 years of age) although these were deceased donors. Gill et al. 40 found no interaction between living donor age and recipient age, suggesting that transplantation from living donors up to 65 years may be considered for all adult recipients since the incidence of acute rejection episodes increases if the donor is older than 65 years. 41 Also after further research, 42 it was recommended that kidneys from older donors should be matched with old recipients and that donors older than 70 years should not be used for transplantation. 43
Study limitations
Limitations of this study include participants belonging to specific groups with experience in renal transplantation or dialysis and may not reflect opinions of the general population on certain issues. This may create inherent bias for our study with a highly selected population, a low response rate and no attempts to increase it with chasing up non-responders. However, our aim was for this pilot study to simulate similar studies for donors, recipients, their families and the general population as a whole to have some initial results and figures supporting certain opinions in a debate regarding the ethical issues in LDKT. Some findings might be influenced to some extent by the established practice in our centre. Multicentre large number surveys are recommended in order to influence and assist the transplant community and government in formulating future renal transplantation policy.
Conclusion
As with any medical ethical study, views expressed by the participants in our study regarding the ethics of LDKT are undoubtedly dependent on the social, cultural and clinical/scientific context in which transplantation surgery is practised. The severe shortage of organs, low risks with donor nephrectomy, benefit for both donor and recipient, outstanding long-term results for the wellbeing of the donor as well as for the recipient and kidney-graft survival, makes kidney donation an attractive alternative for the treatment of ESRD. Elderly and marginal health kidney donors may be accepted as potential donors provided recipients are well informed regarding complications and outcome of such transplants and that they offer their consent.
We believe that this project has produced provoking data concerning elderly and marginal health live kidney donors. We hope that it might be used as a reference tool for future larger surveys that will further contribute to the development of LDKT. Such surveys may be performed at a national or even international level. Their results may lead to change in practice regarding the acceptance of elderly and marginal health live donors by transplant centres.