
Abstract

Introduction
Although medical ethics and law teaching is a required element of the medical undergraduate curriculum, there is a need to ensure that theoretical knowledge is translated into relevant decision-making skills. With at least 85 clinical ethics committees (CECs) providing support for ethical dilemmas arising in clinical practice, 1 might the development of a student clinical ethics committee (SCEC) facilitate both ethical awareness and competency?
The SCEC established at King's College London, School of Medicine (KCLSM) aims to raise awareness and facilitate discussion of ethical issues encountered by students in clinical practice while supplementing current core ethics teaching. In addition, the SCEC introduces students to the workings of a CEC. As medical students do come across ethical dilemmas frequently within their clinical placements, 2 it might be reasonable to suggest that a student forum for ethical discussion, a SCEC, would be a useful adjunct to more theory-based ethics teaching. Just as clinical placements seek to root the sciences of anatomy, physiology, pharmacology (and so on) in the practical medical management of patients, a SCEC could help students reconcile potentially complex moral reasoning with ethically sound patient care.
It might be assumed that as medical students progress through their undergraduate training, their ethical awareness and ethical decision-making skills improve as a result of teaching and clinical exposure. However, studies have shown a worrying trend of ethical erosion in medical students’ capability to identify and manage ethical dilemmas as they progress through their undergraduate education. 3–5 Unresolved ethical dilemmas encountered by students may erode their ethical principles and ‘ethical self-identities’ 3 and inhibit development in moral reasoning. The reasons for this include lack of time for reflection and a focus on scientific medical knowledge. The SCEC seeks to tackle these deficiencies by offering time for ethical reflection and, by purposefully taking a narrative approach to discussion, considers the perspectives of the patient and others involved in the case.
Method
Although no previous reports of a SCEC have been published, students devising the format at KCLSM were assisted by materials available from the UK Clinical Ethics Network and the experience of observing meetings of local CECs. In essence, the SCEC receives a case referral from a medical student, openly discusses it within the group and writes up a summary of the points raised. Documents formally detailing the organization, function and composition of the SCEC have been composed by student members (see Box 1).
Documents detailing the organization, function and composition of the SCEC
• Terms of reference (membership, referrals and meetings)
• Core competencies of SCEC members
• Framework for discussion
• Case referral form
• Feedback form
• Confidentiality agreement
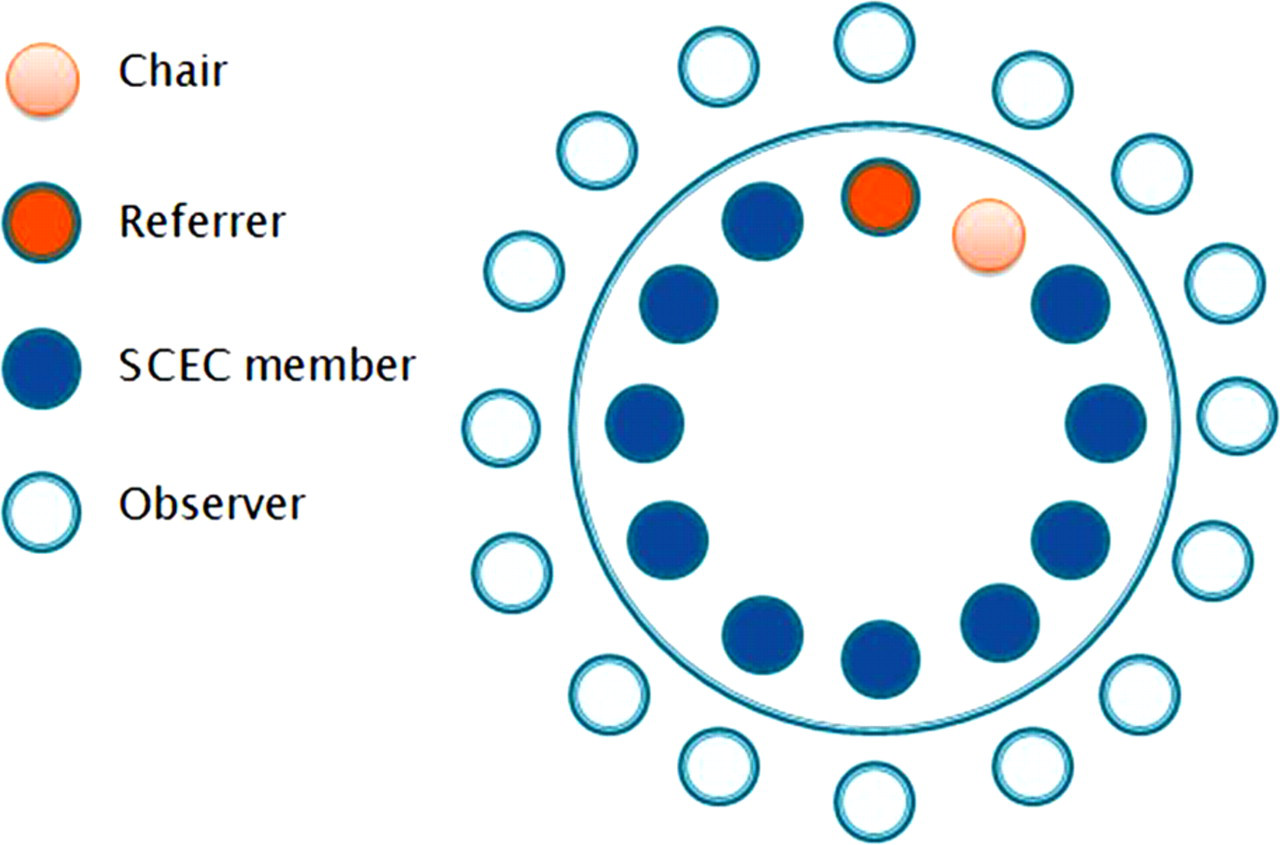
Meetings are attended by 10–15 student members in their clinical years of medical training, one experienced ethicist/educationalist (CJ) and a chair (a student or member of faculty) to lead the discussion. The referrer also attends to present the case and answer questions of fact that arise.
To facilitate informed discussion, SCEC members must demonstrate some learning in clinical ethics, for example through:
taking the student selected component specifically dedicated to training students for the SCEC; or having a relevant qualification in the field of ethics, e.g. diploma in medical/health-care ethics/intercalated BSc/other relevant degree.
In line with core competencies proposed for CECs, 6 all SCEC members must demonstrate core competencies through active participation (Box 2).
Core competencies of SCEC members
• The role of clinical ethics committees
• The key areas included in the SCEC framework for discussion
• Relevant health-care ethics and law
• Relevant clinical terms and disease processes (as a group)
• Recognition of and ability to discuss, moral conflicts within a clinical setting
• Ability to elicit and understand the perspectives of all parties
• Ability to formulate and justify morally-reasoned solutions
• Communication skills including active listening
• Ability to facilitate discussion and respect others’ views
The work of the SCEC is advertized via campus posters and emails. Any clinical year student is invited to refer a case by completing a referral form (Box 3), the details having been suitably anonymized, with the signed consent of the doctor in charge of the clinical case. The SCEC has no decision-making authority; it functions solely as an educational tool. To enhance this, meetings are open to all students within the university, although to aid coherence only SCEC members participate openly in the discussion. Observers are, however, invited to comment at a point during the discussion and at the end of the meeting, and are requested to complete feedback forms in order to evaluate the SCEC. All those attending do so on the understanding that the case referred is confidential (Figure 1).
Referral form
Year of study of referrer __________
Date referred __________
Confidentiality and guidance on anonymity:
Confidentiality is essential to the relationship between health-care professionals and patients and a breach of confidentiality can result in disciplinary action. In order to maintain confidentiality all cases referred to the SCEC must be appropriately anonymized by:
• Removing all unique identifying features in the case study (e.g. patient's name and hospital number).
• Ensuring that remaining details would not allow the patient to be identified using the patient records system (e.g. do not include the patient's exact age, gender and diagnosis).
Clinician __________________________________________
Student _________________________________________
_________________________________________
_________________________________________
The discussion is led by the chair using a framework for discussion (Box 4). SCEC members may take on the role of chairing the meeting. One member takes the minutes and another is responsible for writing up the case discussion. The case write up is made available to SCEC members and the doctor in charge of the clinical case for comment before dissemination.
Framework for discussion
Referral number _________
(1) Summary of case
(2) What are the clinical and other relevant facts?
(3) Who is involved in the decision/what are their perspectives?
(4) What are the possible outcomes in this case and the practicality of these options?
(5) What are the morally significant features of each option?
i) Patient preferences, including religious and cultural factors
ii) Patient capacity (the ability to understand, retain, use/weigh and communicate information) (what are we assessing capacity of?)
iii) Best interests (quality of life, long/short term interests, stakeholder interests)
iv) Non-maleficence/harm
v) Justice/equity
(6) What are the duties of the health professionals involved?
(7) What does law/guidance say?
(8) What are the consequences of the option(s)?
(9) Pros and cons of the option(s)?
(10) Conclusion
Set up of the SCEC meetings
Results
Cases discussed thus far include treatment of a severely mentally ill patient for cancer, withdrawal of treatment towards the end of life against the wishes of the patient's family and suspected physical abuse in an antenatal setting.
Feedback from SCEC members and observers of the meetings has been collated and evaluated. Recurring themes illustrate that the SCEC facilitates students’ personal interest in clinical ethics in a ‘practical’ way, and that the group format leads to the expression of views ‘that one would never come up with alone’ through ‘dynamic discussion’. Students attending the SCEC meetings felt that their ability to handle ethical dilemmas in their future practice was enhanced through personal development and improved ethical awareness as well as increased confidence in group settings. It was noted that every student member contributed to the discussion.
Discussion
It may be that the SCEC functions merely as an ethics developmental tool only for committee members with little benefit to the student cohort at large. However, case discussions are written up and, where appropriate, will be posted on the medical school virtual campus with learning outcomes, links to the curriculum and further resources, thus aiding dissemination of the learning. The SCEC has welcomed student nurses and pharmacists to meetings. Their contribution provides a multidisciplinary foundation to ethical discussion and is effective at encouraging interprofessional learning and reflection.
In 2005 the Royal College of Physicians Working Party report on ethics in practice recommended that ‘ethics support is needed everywhere health care is provided.’ 7 Through attending meetings it is hoped that the SCEC will educate future health-care professionals to the ethics support that is available and encourage them to join, or even help establish, CECs as they progress through their careers.
Future challenges for the SCEC are largely pragmatic – increasing observer attendance and generating sufficient case referrals. Potential developments will include the establishment of an e-learning module to train health-care students in ethical discussion and creation of podcasts of the SCEC meetings, similar to ‘Inside the Ethics Committee’ on BBC Radio 4. The SCEC will continue to encourage wider access to SCEC membership, incorporating other health-care students as members.
Future empirical assessment of student members’ ethical awareness and ethical decision-making skills prior to and post attendance and participation in SCEC meetings will seek to assess the efficacy of the SCEC as an educational intervention. This may take the form of pre- and post-objective structured clinical examinations (and the authors welcome comments and further suggestions on this evaluation). An annual review of the case referrals and student feedback will be carried out.
Conclusions
Slowther et al. 8 noted that ‘a principal value of ethics support may lie in its contribution to the process of ethical decision-making'. The SCEC represents an innovative approach to engage future health-care professionals in the process of clinical ethics discussion that has been warmly received by members. The committee members encourage the set up of SCEC in other medical schools.
Footnotes
Acknowledgements
The authors acknowledge members of the SCEC.