
Abstract
In earlier studies we have shown that abuse in health care (AHC) is commonly reported among both male and female patients. In this study, we present an evaluation of an intervention against AHC based on Forum Play. The evaluation was conducted by means of pre- and postintervention interviews with the staff at a woman's clinic. The interviews were analysed using the constant comparative method. The results of this postintervention study stand out in loud contrast to the results of the preintervention studies. Staff had moved from a distant and fluctuating awareness of AHC to a standpoint characterized by both moral imagination and a sense of responsibility.
Introduction
Health-care evaluation is a growing research field. For instance, the World Health Organization's general population survey nowadays also includes questions about ‘health systems responsiveness’, which is a non-clinical quality of care concept. ‘Prompt attention’ was ranked as being most important and ‘to be treated with dignity’ came second when the study was conducted recently in 41 countries (n = 105,806). 1
The word ‘dignify’ comes from the Latin word ‘dingus’ which means ‘worthy’. But what does it mean to be unworthy?
Jacobson 2 found that violations of patients’ dignity were promoted by the power asymmetry between patients and staff, and occurred through processes of rudeness, indifference, condescension, dismissal, disregard, dependence, intrusion, objectification, restriction, labelling, contempt, discrimination, revulsion, deprivation, assault and abjection.
Jacobson 3,4 furthermore developed a theory that divides dignity into human and social dignity. She described human dignity as a principle and a value that belongs to every human being, while social dignity is generated in relation to others.
Both showing respect for a patient's autonomy and treating a patient with dignity have been shown to be separate factors independently associated with positive outcomes in health care, such as the level of satisfaction, while the probability of receiving optimal preventive care was only associated with being treated with respect. 5
Questions in NorAQ about AHC
Note: The section about AHC was introduced as follows: the following questions deal with AHC. We ask you to mark if you have experienced any of the following events as a child or as an adult. If you answer ‘yes’ to any of the questions 41–43 we consider – in this study – that you have been subjected to AHC
Only recently have voices been raised claiming that health care needs to open up to the creation of a safe environment where questions about AHC and patient safety can be discussed among staff. 12,13
However, there are different ethical standards that ensure that patients are treated well in health care. Among the many methods that health-care educators have used to teach ethics, we can only mention a few here. Fiction, for all classical literature, is an old tool that stimulates the development of moral imagination and a multidimensional understanding of human behaviour. 14 The method has also been used in higher medical education. 15,16 Moral imagination is a term and a concept that has become more and more common, especially in literature on professional ethics. One definition of moral imagination is ‘an ability to imaginatively discern various possibilities for acting in a given situation and to envision the potential help and harm that are likely to result from a given action’. 17
Role play is another method where staff can experience and get a better understanding of different perspectives. Based on neurophysiological studies and the notion that cognitive processes (e.g. imagining the patient's feelings in a certain situation) can change staff's emotional reactions towards patients, this method has been described to ‘sharpen’ staff's senses. 18 There is a need to assess the effectiveness of art-based teaching. 19
The reasoning behind human action is an old philosophical issue.
Glover argues that human action based on rational self-interest does not prevail because human beings are also equipped with moral resources: humanity. Human responses are one kind of such moral resources (e.g. the tendency to respond to others with some degree of respect). This response could be based on a general idea about human dignity, something that most people are born with, according to Glover.
In this project we set out to test a model for educating staff in handling AHC and protecting staff's moral resources by means of Forum Play. ‘Handling AHC’ here could mean handling AHC in a constructive way once it has happened, to intervene when it is happening or to prevent it from happening in the first place. In this study our aim was to evaluate the intervention against AHC based on Forum Play with the help of an external researcher.
Forum Theatre was developed within a literacy program in Peru in 1973 by Boal. 20–22 In his work, Boal developed many different theatre techniques which were influenced by Paulo Freire's work on empowerment and the Pedagogy of the Oppressed. 20,23
In Sweden, both the term Forum Theatre and Forum Play are used. Forum Play, a kind of role play, is played in closed groups without a long rehearsal, while Forum Theatre is rehearsed and played in front of an audience unknown to the theatre group. The collective name of Boal's theatre techniques is ‘Theatre of the Oppressed’. Boal describes Forum Theatre as follows: Music is the organization of sound in time; plastic arts, the organization of colours and lines in the space; theatre, the organization of human actions in time and space. Theatre is a representation and not a reproduction of social reality. FORUM-THEATRE presents a scene or a play that must necessarily show a situation of oppression that the Protagonist (the person who carries the dilemma) does not know how to fight against, and fails. The spect-actors are invited to replace this Protagonist, and act out – on stage and not from the audience – all possible solutions, ideas, strategies. The other actors improvise the reactions of their characters facing each new intervention, so as to allow a sincere analysis of the real possibilities of using those suggestions in real life. All spect-actors have the same right to intervene and play their ideas. FORUM-THEATRE is a collective rehearsal for reality. – Augusto Boal, Rio de Janeiro, 2004
24
In this paper, we use the term Forum Play, since scenes were created in the moment during workshops. Nonetheless, the intervention shared the basic assumptions in Forum Theatre.
Methods
Sample and procedure
The Forum Play workshops were conducted from January 2008 to January 2009. All staff members at the study clinic (n = 136) were invited to participate in Forum Play workshops led by two professional Forum Play leaders. 25,26 Seventy-four participants took part in at least one of the 17 half-day workshops that were held (74/136; 54%).
The workshops had 5–25 participants, including the research team and mixed staff categories (one workshop was held for gynaecologists only).
Interview guide
All postintervention interviews were booked by a coordinator employed at the clinic. The interviews were conducted in a quiet room at the hospital. The interviews lasted, on average, 60 minutes, and a secretary transcribed the interviews verbatim.
Analysis
The transcribed interviews were analysed by an external evaluator (CB). The research question was: what is abuse in health care? Constant comparative analysis, which is the basis of Grounded Theory, was used to process the data. 27–29 A basic assumption of Grounded Theory is that there are similarities in the ways that people experience life. The transcribed interviews were analysed line by line according to Glaser's scheme of open coding to generate substantive codes (i.e. words indicating a relationship to the research question). 27,30 The codes were constantly compared in order to identify similarities and differences and to generate categories which would present the underlying meaning of AHC for the informants. 30 Categories were constantly compared with each other, and data were scrutinized to verify their relevance and find out how they were related in order to identify the core category. The core category is a theoretical construct abstracted from empirical data that answers the central research question(s). 30 To improve the trustworthiness of our analysis, the data were reviewed several times and considered repeatedly. Some flow charts or matrices were developed to compare and contrast cases and properties of emerging concepts and categories. Categories were confirmed by repeatedly returning to the original data and by ensuring transparency in the processing of data; all results can easily be traced to their origins.
Ethics
Written informed consent was obtained from all participants before the interview. Our request to conduct the study had been approved by the Regional Ethical Review Board (registration number 194-06).
Results
Four categories were identified during the constant comparative analysis regarding AHC: neglecting, derogatory, insensitive and non-empathic (Figure 1). All categories are related and thus influence each other, but they are separate, aiming to construct the core category. The core category and categories identified and described are abstracted to a theoretical level. All categories are presented in order to illustrate the origin of the core category, minimizing human dignity, which is presented at the end of the findings.
The core category, minimizing human dignity, and the four categories constructing it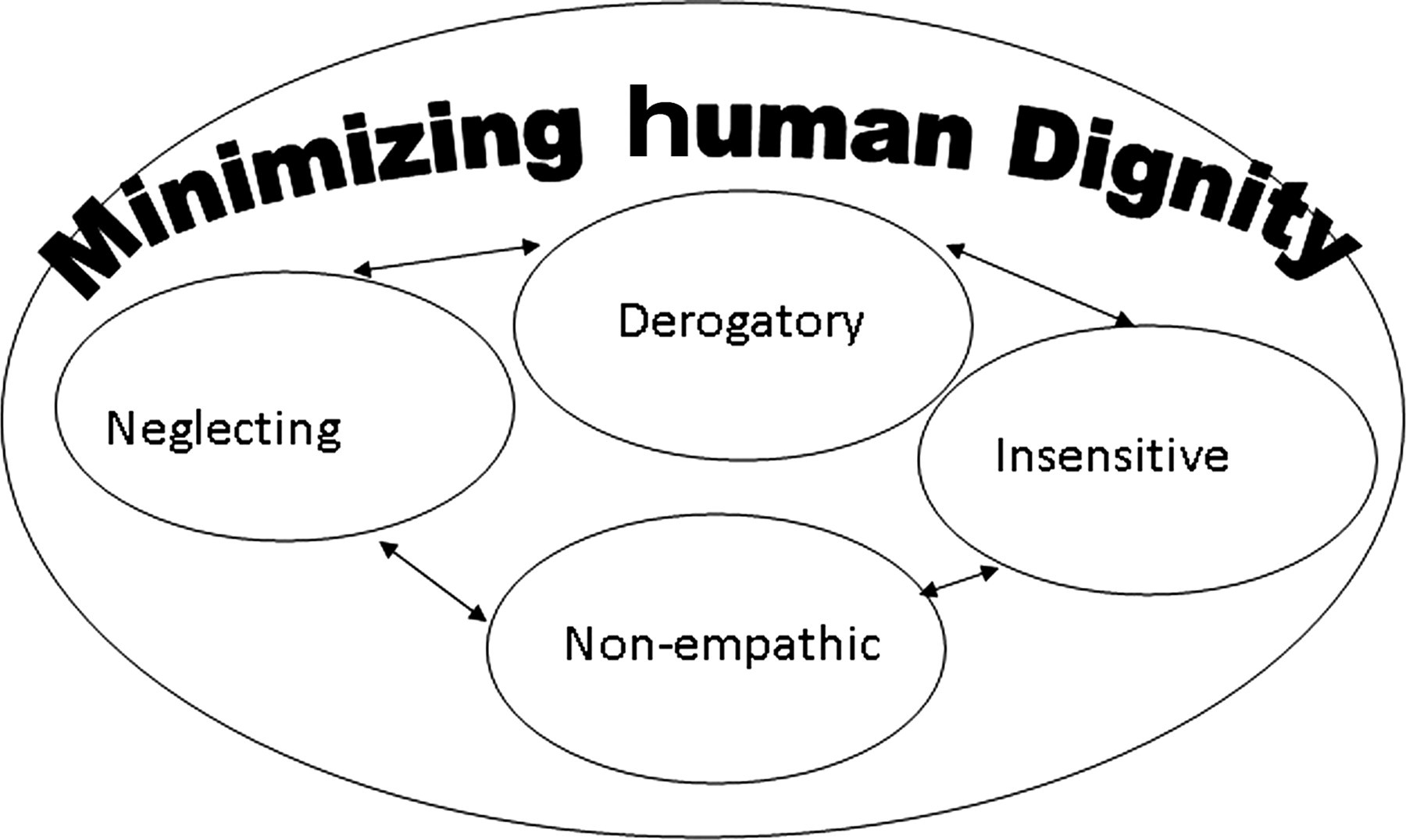
Neglecting
Staff described neglect as paying little or no attention to the patient (i.e. neglecting is an act). In caring encounters it was also seen as lack of attention or care. One of the most striking events in a person's life is to be ignored and not being seen as the human being he or she is. Neglecting could be, for instance, pretending that you do not see the patient. In the health-care system staffs abuse the patients, sometimes consciously and sometimes unconsciously. Patients can perceive carelessness and feel neglected. Time is a significant aspect of feeling ignored by the staff. When staff are in a hurry, patients feel that everything has to be done as quickly as possible, and patients are not seen as human beings: they are being objectified. Withholding information is also a way of neglecting a patient. Neglect is something that does not only happen between staff and patients; it could also be seen between staff members. Everybody can be neglected. A quote about not respecting patients’ integrity follows here. For example the ones who… come for a medical abortion and they sit out here in the waiting room and then… they [staff] start asking them [things] out there. How are you… jaunty and happily, because I can hear that sometimes when I sit over there… And then I think… they don't need to start asking [questions] out
Derogatory
This is when persons make disparaging remarks, or when they are deliberately offensive. Making someone else lose their face is a typical example of a derogatory act. Often a derogatory acts are noticed as verbal comments, condescending statements or the ridicule of a person. It could also be to talk over a person's head (often the patient's). Sometimes a derogatory act can be considered a disparaging action, improper behaviour or a caring encounter where the patient is exposed indecently. Actions where patients are kept in a firm hold, against their will, are also derogatory.
Derogatory acts could include physical actions or verbal expressions. The outcome is often the same: the patient is ill-treated, there is a bad reception and the patient is emotionally affected. A quote illustrating the saying of things that are abusive (e.g. ridiculous or derogatory): If you continue to talk about eh, about Greta for instance [a made-up patient]. I don't think that's fair. To… well ridicule Greta and that Greta has done this and Greta has done that… said something that came out wrong so to speak, things like that. Those are things that you can naturally talk about and think… it can be a little fun so to speak, but not in a mean way but you think that… that might be it, lifting the whole thing because it becomes… It might become hard sometimes to work with… confused people and all that so to say. But not… to
Insensitive
Staff described insensitivity as being unfeeling. This is about not taking time or considering the patient's needs; not being sensitive. Sometimes the intention is to be considerate by asking questions and not listening to the answers. Making a quick interpretation of the situation without having all the facts is to be insensitive. As staff members, we need to be present and considerate to patients, otherwise we are insensitive. Consideration is needed. Without consideration we act inhuman. Staff stated that the most common abuse was probably being insensitive; not being considerate and taking into account the patient's feelings and their situation. We, as human beings, are unique: we have different experiences and expressions. If we, as staff members, do not take that into consideration, we are insensitive and will also make the patients lose confidence in the staff or even the health-care system. Insensitivity was expressed by one informant as: ‘to step right into the patient's area, without being careful’ (Interview 3).
Non-empathic
This was described as not having the capacity for participating in and understanding the feelings and/or ideas of another person. Staff are obliged to ‘read’ and understand the patient and, in this caring encounter, establish a relationship with the patient. These situations demand a sense of empathy. Staff must be receptive to a patient's communication and also understand their communication. This understanding is shown via behavioural actions. But when staff are occupied with themselves or other tasks, they will become non-empathic. They will not even try to place themselves in the patient's situation or try to understand the consequences of an action. Non-empathy in staff could be a very frightening experience. Perhaps it is something very small, but it could be experienced as coldness or non-empathy. Non-empathy could be interpreted in what you are saying, how you say it and how you perform actions and tasks. Non-empathy is very much an attitude. As one staff member expressed it: ‘you need to think carefully about what you say and how you say it’ (Interview 11).
Core category: minimizing human dignity
The core category is a theoretical construct abstracted from categories and empirical data and identified by developing integrative hypotheses about the relations between the categories. The four categories – namely neglecting, derogatory, insensitive and non-empathic – overlap, but each of them could be regarded as a possible entrance to an outcome of minimizing human dignity.
When staff pay little or no attention, patients are neglected and their value as human beings is minimized. This same effect was expressed when patients were disparaged or made to lose their face in public situations. Sometimes these are situations or caring encounters where the patient does not have the possibility to cover him or herself or take shelter. When staff are not being sensitive, showing in various ways that they are not considering the patients’ needs, they act inhumanly. This insensitive behaviour sends out signals that the patient is not valued, which minimizes their human dignity. Insensitivity and derogatoriness were closely linked to each other and can, in certain situations, strengthen each other. Even neglect and non-empathy are closely linked to each other. If staff are not having the capacity for understanding the feelings or ideas of the patient, it could be said that they are non-empathic. Neglect could be seen as an action, but non-empathic is more of an attitude.
The effect of these categories separately or intertwined will correspond with the core category minimizing human dignity; answering the question what is AHC? ‘Well, [it is] when you deprive somebody his human dignity in some ways…’ (Interview 1).
Discussion
The results from this postintervention study stand out in loud contrast to the results in the preintervention studies. 10,12 Staff have moved from a distant and fluctuating awareness of AHC to a standpoint characterized by both moral imagination and a sense of responsibility. This movement has positioned staff perspective much closer to the patients’ perspective. In earlier studies, male and female patients stated that AHC meant losing their value as human beings and their autonomy. 9,11 In the present study, staff expressed a very similar understanding summarized in the core category ‘minimizing human dignity’.
These results are also in accordance with the other postintervention evaluations in the same project. 31,32 The analysis of the very same interviews, conducted by the researchers who led the intervention, rendered categories similar to the one found in the present study but there were also differences. 32 The leader of the intervention found categories that could be interpreted as if there were still some resistance against recognizing AHC among staff, e.g. they still needed to underline that they thought of AHC as unintentional staff behaviour and they were hesitant to use the term AHC, preferring expressions such as ‘a failing encounter’ instead.
Moreover, the leaders of the intervention also found a strong imperative among staff to act against AHC, which contributed to the core category ‘a summoning stone in the shoe’. This aspect is absent in the analysis of the present study, but the urge to act was also found in another set of interviews conducted and analysed by another external evaluator. 31 In these interviews, staff gave many examples of when they had actually acted differently from how they used to do in order to prevent AHC. The aim of Forum Play is to give the participants options to act differently, and during the workshops the participants practiced many different ways of acting against AHC. In other words, staff was trained to counteract AHC in a ‘collective rehearsal for reality’. 21,24
The question remains, how can a distinct aspect be present in one analysis and not in another when both are analysing the same interviews?
First, a qualitative study starts and ends with the presumptions of the researcher. 33 One of the analysers had participated in the intervention, the other had not. The one who had participated had been trained in acting against AHC and had also developed an understanding for behavioural change in this context. Thus, acting against AHC was central in her own thinking. Line by line coding probably helped her not to get stuck in the acting aspect but also with identifying other categories. 34
Secondly, there might have been a slide in the interpretation of the research question: what is abuse in health care? To demarcate the analysis is always an act of balance in qualitative studies. Some researchers know that they tend to keep too much information in their analyses because ‘it might turn out to be important at the end’. Obviously, it is difficult for two independent researchers to put down the demarcation poles at exactly the same spot.
These assumptions are integrated and triangulation is often used to solve the problem, and then differences are discussed and finally there is a consensus. Is that always a beneficial way of dealing with differences in results? How do you know that important results are not masked in the effort to reach consensus? In our case, we consider a similar movement towards the patient perspective, which could be noted in both studies between the preintervention and postintervention studies as the most important finding. The studies support one theory – AHC is minimizing human dignity – and the action aspect adds something to that theory.
Our conclusion is that Forum Play contributed to the staff's increased awareness of AHC, and that they could identify themselves with the patient's perspective on AHC. Considering results from the other analysis of the interviews in this study, we can add that this awareness has implications for staff, e.g. it urges them to act against AHC.
Even though Forum Play is used all over the world, this study is one of the first to attempt to scientifically show that Forum Play promotes individual change. However, this is a small contribution, and more research will be needed in the future. In this particular project, it would be interesting to conduct a long-term follow-up study, and moreover, to evaluate possible changes on a structural level.