
Abstract
Social, legal and health-care changes have created an increasing need for ethical review within end-of-life care. Multiprofessional clinical ethics committees (CECs) are increasingly supporting decision-making in hospitals and hospices. This paper reports findings from an analysis of formal summaries from CEC meetings, of one UK hospice, spanning four years. Using qualitative content analysis, five themes were identified: timeliness of decision-making, holistic care, contextual openness, values diversity and consensual understanding. The elements of an engaged clinical ethics in a hospice context is not generally acknowledged nor its elements articulated. Findings from this study have the potential to explain some of the most challenging ethical problems and to contribute to their resolution. It may also guide future deliberation and raise CEC members’ awareness of the recurrent issues and values of their CEC practice.
Introduction
The increasing complexity of everyday hospice practice places increasing demands on health-care professionals (HCPs). In response, different forms of clinical ethics support have been developed. In the USA, all health-care institutions are now obliged to have a process for considering ethical issues in patient care. 1 This supported the development of ethics case review by clinical ethics consultants and committees (CECs). Although the UK has no such requirement, the number of CECs has grown from 20 in 2000 to 85 in 2011. 2 CECs generally have three functions: case analysis (current and retrospective), policy analysis and ethics education. The first function, case analysis, is the focus of this paper.
In end-of-life care, ethically difficult decision-making is common - for example, in relation to capacity, autonomy, best interests, conflicting opinions, equity, futility, patient safety and the withholding and withdrawing of treatments (particularly artificial feeding and hydration). Alongside clinical complexity, social, political and legal changes present further challenges for health-care provision, with the need for health-care organizations to be more transparent and accountable. 3 The increasing complexity of treatment options, both in scope and in technological sophistication, can risk over-medicalization. The expanding number and diversity of HCPs and organizations that are often involved in an individual's care, particularly in palliative care, can undermine the patient's voice and leave care directionless, with no clear lead clinician. 4 Continuity of care has reduced, particularly from doctors, following subspecialization, increased delegation, altered working patterns and reduced hours. Rising expectations of patients, society and HCPs, coupled with increasing legal and professional scrutiny, also carry an ethical impact on palliative care. The spiralling cost of health and social care (due to increasing longevity and treatment advances) directly opposes the reducing budgets that are available. The projections of ‘potentially infinite demand and finite resources’ support the need to ration health care, such as hospice beds. 5
Inevitably clinical ethics is ‘deeply engaged in the clinical setting’ 6 and a CEC or group can help HCPs to negotiate constructively some of the most challenging ethical issues. However its potential is not generally acknowledged or its elements articulated. Clinical ethics is ‘essentially and inextricably bound up with’ actual patient care. This paper, detailing the themes that arose during hospice CEC discussions, articulates some of the components of an engaged ethics. It has the potential to guide future deliberation and to raise CEC members’ awareness of the recurrent issues and values of their CEC practice.
Design
A qualitative study of written summaries from a hospice CEC spanning four years (2007-2011) was performed. We set out to respond to the question: what themes arise in the CEC discussions as presented in meeting summaries? The core CEC membership contributing to the case discussions included external support from three academics (two Professors and one Reader) and broad internal multi-professional representation from medicine, nursing, education, chaplaincy, physiotherapy, speech and language therapy and social work. At quarterly CEC meetings there was a discussion of the ethical dimension of anonymized clinical cases where a significant dilemma or challenge had been encountered. Using contemporaneous notes, written summaries were prepared and archived (by CG), after formal CEC agreement of accuracy.
The data in the summaries were subjected to qualitative content analysis. 7 This involved identifying meaning-units that were then condensed to codes and led to themes that captured the manifest and latent content of the data. By ‘manifest’ content we mean the description of the visible, overt content of the data. By ‘latent’ content we mean an analysis of the ‘underlying meaning of the text’. 7 On completing the initial analysis (by GH), with saturation of themes, the elements of a more pragmatic approach to real-life ethical situations had become apparent. This was presented at an open CEC seminar and fine-tuned. AG and CG cross-checked the codes and themes to strengthen the credibility and trustworthiness of the analysis.
Approval was obtained from the hospice's research committee. External ethics approval was not necessary as this was a service evaluation (‘analysis of existing data’). Crucially, no patient data were ‘studied’ and CEC members were aware that internal and external dissemination of their anonymized contributions was an integral CEC function.
Results
Five over-arching themes emerged from the analysis: (1) timeliness of decision-making, (2) holistic care, (3) contextual openness, (4) values diversity and (5) consensual understanding. Each theme is derived from meaning-units within the summaries that were linked by codes (sub-themes) (see Tables 1–5)
Theme 1: timeliness of decision-making
Theme 2: Holistic care
HCP, health-care professional
Theme 3: Contextual openness
Theme 4: Values diversity
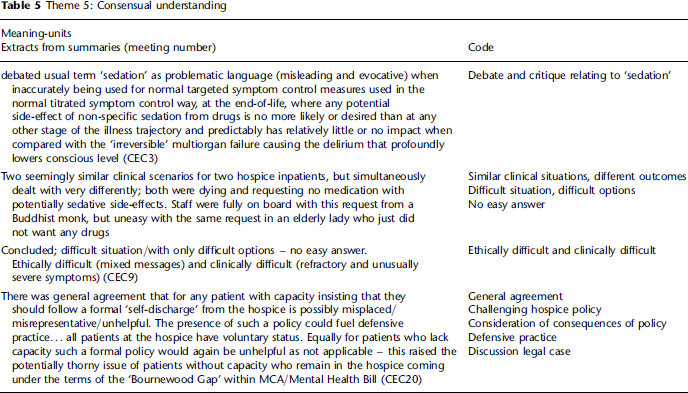
Theme 5: Consensual understanding
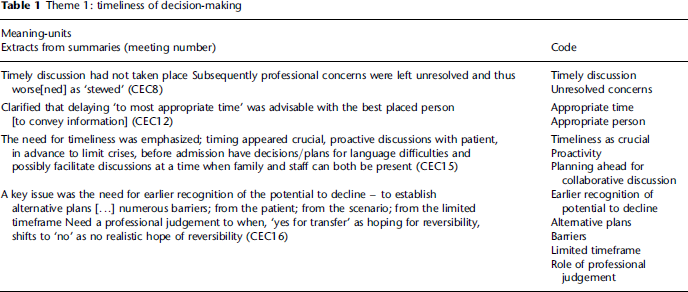
Timeliness of decision-making
The data suggest that key clinical decisions are sometimes delayed and difficult discussions all too easily avoided, in the hope that another HCP would have the necessary conversation. Emerging concerns should, the data suggest, begin to be addressed as soon as possible and not be left to ‘stew’. For example, in a well-meaning desire to avoid confrontation there are examples of HCPs delaying challenging family members who appear, for example, to be over-feeding a patient. However, the CEC discussion engages with the possibility that this may unwittingly endorse the unhelpful behaviour, which then gets entrenched and is harder to manage. Similarly HCPs may postpone a difficult disclosure, only for that patient to lose trust when they become aware that information was withheld. HCPs may, for example, avoid discussing the predictable need for ventilator support in a person with motor neurone disease until an on-the-spot decision is needed, by which time it is too late, as the person may then be unwell, distressed and possibly confused. Conversely, the data illustrate that badly timed truth-telling may be morally no better than a measured failure to disclose or even to lie (see Table 1).
Starting discussions did not necessarily suffice to support key decision-making. The data suggest that discussions must continue as an ongoing and iterative process of ‘updating’ as required. Subsequently when decisions have to be made quickly, e.g. when a patient suddenly deteriorates, actions do not appear hasty or inappropriate. For example, informed consent is an evolving process, not just a one-off ‘tick-box’ encounter to obtain a patient's signature. Key information needed to be exchanged with all the potential stakeholders in a timely manner. Potential stakeholders include patient, family, friends, significant members of civil society (churches, clubs, etc.) as well as health-care agencies (e.g. general practitioner, hospice and hospitals). The CEC discussion recommends that relevant information needs to be shared, as much as is realistic and as soon as possible. This includes negotiating the respective responsibilities at the earliest possible stage by establishing a clear lead clinician. Effective decision-making also requires the right information, to be exchanged in the right place with the right method. Maintaining good feedback appeared essential for continuity of care, especially at critical times, on changing place of care (e.g. hospital-to-hospice transfer, as key professional stakeholders change) or changing the focus of care (e.g. active to conservative management). Good feedback requires more accurate and explicit documentation of advance care planning in addition to good verbal handovers. Handover remains just as important for patients at the end-of-life requiring conservative management; emphasizing earlier recognition of the potential to decline and ensuring that care does not veer back to more active management.
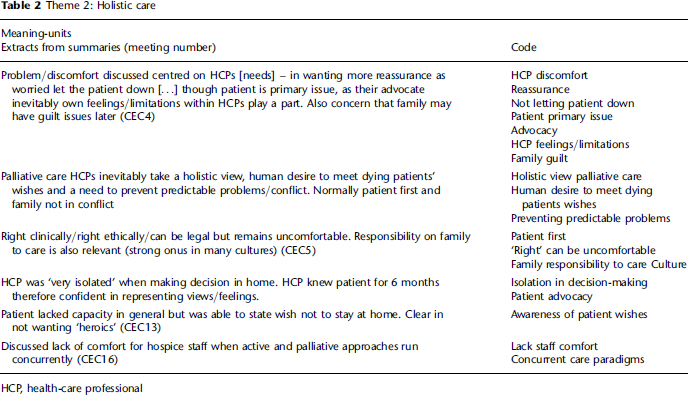
Holistic care
The centrality of holistic care, in particular the concepts of compassion and empathy, is evident within hospice CEC discussions as HCPs negotiated challenging practice situations. CEC members identified with and accepted others’ fears (even when unexpressed) and their need for comfort. Though the benefit of holistic care is evident, the data suggest that a balance appears to be struck between the HCPs’ care for the patient and their family, and care for the HCPs themselves (see Table 2).
Ethical concerns raised by hospice HCPs often reflected their perceived failure to meet admirable, but possibly unrealistically high, expectations. There was a greater need for talking, finding out, teasing out and interrogating any possible misunderstandings, negotiating and compromising, and dealing with any underlying denial (including one's own). However, the cost of getting close to and advocating for patients and families was the need for HCP comfort and reassurance that they are doing the right thing. Yet HCPs also need to appreciate that doing the right thing - legally, ethically and clinically - may not feel comfortable. The CEC discussion data support the view that holistic care can be fostered by interrogating the physical, social, psychological and spiritual preferences and needs of others; helped by sequentially putting ourselves in the position of the patient, family, health-care colleagues and relevant managers. ‘What would a typical person want or not want for their loved one in a situation such as this?’ is an initial test for a decision-maker at any level.
Although there was some evidence of contextual constraints, caring was considered paramount and a good deal of sensitivity was demonstrated in the hospice CEC discussions, acknowledging the vulnerability of patients, families and colleagues and their need for comfort rather than wanting ‘heroics’.
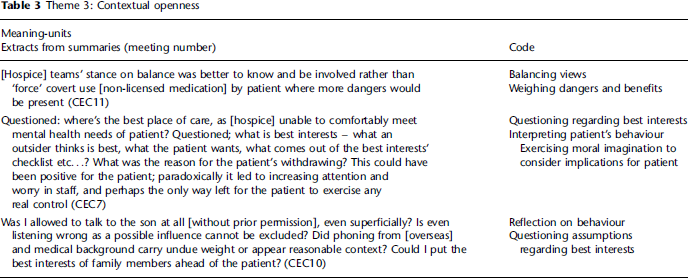
Contextual openness
Contextual openness is closely connected with timeliness and holistic care. It means an openness of mind and receptivity to changes of context from one place and one time to another. Key decisions, even in one case, do not remain the same; one has to remain sensitive to how a shift in context (e.g. a change of heart by a patient, or a new and surprising piece of information) can require a change in nearly everything else in one's decision-making (see Table 3).
The data illustrate how ethical concerns sometimes reflected personal rather than professional discomfort with scenarios, as hospice HCPs struggled to adjust to inconsistencies in the views, behaviour or choices of patients and their families. HCPs sometimes need to accept that in the context of the unease and sadness of the dying patient, the patient or family may transfer feelings of fear and loss to HCPs in the form of complaint and blame (and vice versa). It is easy to lose this openness when working with dying people every day.
A lack of contextual openness in the HCP outlook is revealed in the ‘unnecessary unhappiness’ of the HCPs. That is, not accepting the truth that in any specific clinical context, everything that could have been known and that could have been done, may have been known and done at the time; so any residual lack of satisfaction with the outcome had nothing to do with any act or omission on the part of the HCP. The data suggest that what appears right at one moment is revealed to be wrong at the next, but often that does not mean that one has made a bad decision or that one could or should have done ‘better’. It would not be true to the human condition to expect every single hospice death to follow the presumed perfection of the ‘good death’. This does not mean that one should not always do one's best - it means that doing one's best is no guarantee of a perfect outcome. If the HCP is very attentive to the specific context of a case they can directly see the truth of this. Thus, it is imperative that our professional training does not hamper our ability to see the wider picture; clinical decision-making takes place in a real living world constantly shifting and riddled with uncertainties, typically quite distinct from the theoretical environment of academic learning. The final extract in Table 3 illustrates the process of reflection and questioning required when there is uncertainty regarding family involvement without patient consent.
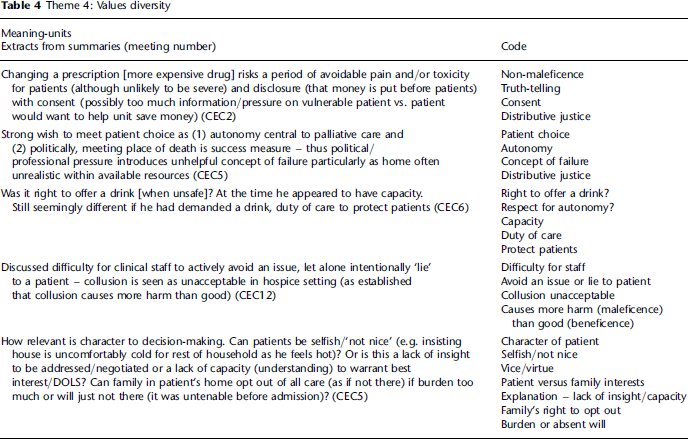
Values diversity
It is often because of diversity in values that the previous three themes are so important. ‘Values diversity’ describes the differences between individuals and between groups on what is important in their lives. These are moral, customary, religious and existential, political, aesthetic, and matters of meaning, personal character and life-style preference (Table 4).
The data highlight how ethical dilemmas and conflicts commonly followed when key stakeholders failed to appreciate each others’ ‘outlook’ or ‘stance’. HCPs may insist on a patient giving a ‘reason’ for a stance without appreciating that many of one's own stances have no explicit reason yet still remain the ultimate basis on which sense is given to life. Even across different professions there will be different assumptions and priorities; doctors, nurses, social workers, therapists and chaplains do not necessarily agree, even when they have exactly the same facts on a case. Patients and their families may be even further removed in their views; each may be shocked by the views of others. Thus, the data suggest that it is imperative to re-think our compliance in the psychological sense; to be able to respond more favourably to the explicit or implicit requests of patients and their families.
A family's wishes to take or avoid a course of action that they believe is obviously ‘right’ for their relative may appear equally ‘wrong’ to HCPs, e.g. blocking the disclosure of a poor prognosis to a patient. However difficult, it is important for HCPs to remember that family members are generally better placed to understand the character, values and life-story of their relative. HCPs should not presume that the family's motives are misplaced. In this situation HCPs can present the biomedical facts, to explain and advise, but must not insist or exaggerate an opposing HCP position or they may risk making family and patient needlessly unhappy. A peaceful death requires more than just getting the biomedical situation optimized; a person is not simply a dysfunctional organism. Thus HCPs need a preparedness to re-think their approach to a failure of ‘compliance’, e.g. patients not taking their medications as suggested or failing to attend outpatient appointments.
The need to recognize and act on ‘values diversity’ gets more difficult in complex organizations, where the obvious can be missed while the complicated is analysed and made even more complicated. What is directly in front of the HCP may be overlooked if overly focused on the technical, procedural or legal. It is important not to forget that what is ordinarily most important in life for HCPs outside of work is often what is most important for patients. When trying to balance the key issues within complex medical problems, it is surprisingly easy to miss the ordinary and palpable. For instance, the patient's dignity, self-control, sense-making, memories, children, grandchildren, home comforts, favourite foods, own clothes, favourite music, belongings, pets, unfinished business, financial concerns, familiarity and routines. These things will often take priority in a patient's mind ahead of the biomedical factors and interventions that seem obvious to HCPs. If the ordinary and the biomedical requirement come into conflict, the patient will often, and has the right to, choose the ordinary. If common sense is forgotten in clinical practice we risk depersonalizing our care. Barriers can be generated if clinical decisions threaten these ordinary things, e.g. not ‘allowing’ a patient to go home because of professionally perceived limitations to care at home. While remaining clinically competent, HCPs must equally maintain common sense while balancing a range of ethical values, for example, autonomy, non-maleficence, justice and care. Otherwise we may ‘know’ much less than the patient; a patient may be happier at home despite their relative increase in vulnerability. We need to check what really matters to a patient and avoid technical language which could both confuse and distract patients from the seemingly more mundane but potentially more relevant aspects of their lives.
An underlying strand throughout much of the data, primarily for HCPs, is the importance of character or a virtues-based approach ‘ to clinical ethics practice. This was apparent both in the way that HCPs responded to patients and in the way that CEC members responded to cases; there is support for the virtues of wisdom, compassion, open-mindedness, justice, courage, humility, veracity and trustworthiness.
Consensual understanding
A shared understanding among stakeholders is essential to progress in difficult decision-making. This consensual understanding, derived from the CEC summary data, brings the preceding four themes together in ‘one place’. It requires the open clarification of assumptions (taken-for-grantedness) and identification of all the differing values and real priorities across all stakeholders. Consensual understanding also requires timeliness, e.g. knowing when best to deal with denial in a stakeholder. An adequate degree of trust is needed for a shared understanding to prevail and to maintain the social cohesion of the organization, and this requires effort to achieve and sustain. Trust is also necessary to negotiate contested issues, policies and practices (Table 5).
Consensus-finding centres on stakeholders working to achieve an understanding around shared values and goals, or at the least tolerantly acknowledging differences. Sufficient consensus can be achieved using the simple techniques of more transparent discussion and problem-sharing, both formally and informally, negotiating ‘contracts’ and clarifying mutually agreeable boundaries. Subsequently, it is possible to set priorities around areas of existing agreement (where patient's wishes meet what health care can provide) rather than get ‘stuck’ in areas of disagreement. Table 5 illustrates some of these issues and also an awareness of the need to avoid defensive practice.
Consensual understanding is not necessarily the same as consensus, which may not be achieved, e.g. when facing psychological denial or a strong attachment to a narrow interest. Consensual understanding importantly allows ‘agreeing to disagree’ as normal in some circumstances of stakeholder negotiations.
Discussion
Clinical ethics committees provide a process to examine professional values, analysing how HCPs treat and regard others. This process can aid HCP decision-making, by clarifying our thoughts and the nature of the problem. This in turn can foster equity, enhance communication (with patients, families and colleagues) and provide a constructive way to resolve disagreements.
The qualitative content analysis of summaries from a hospice's CEC meetings, spanning four years, revealed a rich and engaged clinical ethics practice. Five themes emerged that appeared to be at the root of most of the problems, dissatisfaction and failures within the scenarios discussed and to point to the means for their resolution. While in many ways unsurprising, realizing that we generally know what constitutes ‘good practice’, the identified shortfalls do signal ways to improve care. Agich 6 writes that ‘the meaning and interpretation of the actions in the clinical case are reconstituted by the individuals involved therein’. It is this collaborative reconstitution, derived from working together to reach consensual understanding, which represents the value of clinical ethics practice. The themes identified suggest the elements of an engaged clinical ethics that recognizes these issues, and goes ‘back to basics’ by building itself on clinical reality and rediscovering simple ethical truths that are in danger of being lost in complexity.
While the value of CECs has been disputed, 10 the analysis suggested that this hospice CEC maintained and furthered a positive moral climate and developed multidisciplinary dialogue and consensus. The discussions provided a better organizational understanding, an organizational memory (supported by openly available documentation) and organizational learning. These help to direct the follow-up of numerous problem areas and shape future discussions and education events to improve on the quality of care.
A common feature in ethically troubling cases was a breakdown or gap in communication that followed when clinical plans had not been worked through soon enough with the right people, and/or there was a lack of initiative, creativity or foresight in making a ‘connection’ between actions/events past, present and future. ‘Delayed clinical plans’ is a more formal issue which may be at least in part addressed by procedures and guidelines. In contrast, ‘lack of initiative’ is less able to be formalized, having to do with mindsets, levels of responsibility and cooperativeness; this may be addressed through leadership, education and organizational learning.
To improve the timeliness of decision-making, discussions concerning predictably problematic clinical areas need to start sooner, occur when the right people are available, be revisited when needed (with continuity), have their outcomes shared and be reinforced at key times. For decisions to be made at the right time, opportunities for open discussion must not be missed and may need to be created. In particular, HCPs should actively seek a window to clarify a patient's wishes around a suitable ceiling for future care. Yet sensitive issues must not be rushed either. HCPs must initiate and pursue deeper discussions when appropriate, not too late and not too early. While it may be difficult to always know the ‘right time’, a sense of timeliness could be seen as a virtue required of HCPs; the ability to judge a good time to have key discussions and to negotiate who would be responsible for these discussions and the subsequent decision-making. Improved timeliness can prevent avoidable distress by fostering prospective decision-making in difficult scenarios. Though good timing is an obvious ideal, greater organizational awareness of timeliness and willingness to take responsibility is needed to improve care. Education and support is required to ensure better inter-agency communication, ideally to include reflective practice and formal clinical ethics input. Equally patients need to be prepared that a change of setting, despite the presumption in favour of continuity of health-care decisions, will inevitably come with a concurrent need for reassessment and potentially a re-negotiation of plans.
Holistic care flows more naturally when we get to know the patient as a person rather than merely a vehicle containing the disease or dysfunction that needs medical interventions. Getting to know the patient and then being there with that patient takes significant time. Unfortunately, acute medical settings do not always highlight spending this extra time with patients as a priority. In contrast, hospices usually allow greater flexibility to allow a holistic approach. When providing holistic care, in typically difficult and stressful situations, it is important for HCPs to retain realistic expectations and to care for themselves. HCPs need better support to deal with the uncertainties and limitations of medicine, the service and themselves as individuals.
Contextual openness appreciates that appropriate outcomes for the same clinical decision will change over time, from context to context and according to the individuals involved. Decisions may have to change swiftly with shifts in the context, e.g. clinical condition, resource pressures and misunderstandings. While algorithms, protocols, guidelines and procedures are all crucial aids to complement the evidence in reaching a conclusion, HCPs must also have the courage and responsibility to have contextual openness to practice situations. The responsibility for clinical decisions should be shared; HCPs clarify the applicable treatment options, with a presumption in favour of meeting the patient's wishes. Yet HCPs are obliged to explore a patient's choice; this does not mean disregarding patient autonomy, but the opposite, taking autonomy into account in a more balanced and insightful way. What does a patient asking for seemingly futile artificial hydration at the end of life really want - increased hydration or increased hope? Conversely, HCPs also need to be open to context ‘within’ the broad framework of standard practice. How much harm would the allowing of artificial hydration cause, in contrast to a blanket refusal to give it? Professional wisdom should still be seen as a key virtue required of HCPs. 8
Clinical dilemmas follow if HCPs do not display sensitivity to the diversity of values between the different stakeholders. Despite the clinical necessity of generalizations (non-discriminatory pattern recognition is part of assessment) we must appreciate the differences in what is important to different people or groups. HCPs must first acknowledge that their professionalism carries its own values; this is particularly difficult as these are typically second-nature and therefore ‘invisible’. Though these professional values will typically overlap with patient values, they can often diverge from them too. We sometimes need to go out of our way to understand the world-view or lifestyle that underlies requests that do not make immediate sense to us. There may be a life-story, a narrative, which needs time and patience to understand, particularly if at odds with HCP paradigms. For example, the patient may feel strongly that a hoist is undignified and would rather risk being harmed than use one. Here understanding and negotiation may be necessary; remembering that what is most important to HCPs outside work is often the main issue for patients.
The need for a shared appreciation of all perspectives in difficult clinical decision-making makes consensual understanding pivotal to good practice. Investment is needed in CECs and internal and external educational programmes that promote consensual understanding. The consequent increase in rapport, tacit agreement and cooperation can smooth all care activities, in contrast to the alternative, where each ‘camp’ retreats to entrenched positions of non-communication or even unmoving opposition. Following the CEC discussions, the hospice's HCPs were better placed to develop and sustain a consensual understanding that implicitly underpinned decision-making and work together in an efficient and harmonious way for mutual benefit.
Conclusion
The five themes, derived from the discussion of real cases, appear robust in relation to the work of this hospice CEC. They suggest the elements of a deliberative engaged ethics with the potential to strengthen future case reviews and potentially resolve or even prevent conflict among the stakeholders (patients, families, HCPs and others) in difficult clinical situations. The analysis also identified virtues that should enable HCPs a more ethically engaged approach to care. Sharing the findings - within CECs and throughout organizations - contributes to the integration of ethics into day-to-day practice and could result in higher levels of consensus, thus enhancing the quality and dignity of care. Clearly, differences of opinion, resource limitations and system errors will remain, but hopefully at a lower level. The themes that suggest the elements of an engaged clinical ethics will continue to be tested and shaped by actual practice.
We cannot claim that our findings are fully generalizable, but suggest that valuable insights have been obtained from the summaries. It was not possible to discern among the contributions of different HCPs or to observe if any patterns were identifiable in relation to gender, class, ethnicity or experience. Further research is necessary to include observation and recording of CEC discussions and interviews with CEC members. Our findings support the point that clinical ethics is indeed ‘deeply engaged in the clinical setting’. 6 The themes that emerged have the potential to guide future deliberation and to raise CEC members’ awareness of the recurrent issues so they can respond more proactively as they recognize the pitfalls and opportunities.
Footnotes
Acknowledgements
We thank the members of the Clinical Ethics Committee who share so generously their perspectives and professional wisdom. We would also like to acknowledge the contribution of the late Professor Paul Wainwright who co-chaired the CEC and contributed to the case analysis.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.