
Abstract
This paper reports the results of a survey study examining the knowledge, motivations and concerns of egg-share donors and recipients, and assesses the clinical and policy implications of these findings. The survey, combining quantitative and qualitative items, was completed by 48 donors and 38 recipients who took part in an egg-sharing scheme at the London Women's Clinic between 2007 and 2009. Although the most important motivation for all egg-sharers was to have a baby, both donors and recipients displayed multiple motivations, including elements of self-interest and altruism. Many viewed egg-sharing as a reciprocal process in which two women with different needs help one another. The results are reassuring from an ethical and policy perspective: they suggest that if information about egg-sharing was more widely available (especially through general practitioners), more women may consider becoming egg-share donors, gaining swift access to their own treatment and reducing the UK's egg donor shortage.
Introduction
According to the Human Fertilisation and Embryology Authority (HFEA), which uses a definition of infertility as a ‘failure to conceive after frequent unprotected sexual intercourse for one to two years’, infertility is estimated to affect around one in six or seven UK couples, equating to approximately 3.5 million people. In fact, infertility constitutes the most common reason why women aged 20-45 see their general practitioner (GP), after pregnancy itself (http://www.hfea.gov.uk/infertility-facts.html). In addition, growing numbers of single women and women in same-sex relationships are consulting the medical profession for reproductive assistance. While many fertility problems will be resolved by drug regimens, increasing numbers of patients each year are undergoing high-tech fertility treatments, such as in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI), and many are conceiving with the aid of donor sperm and eggs. Egg-share donors and recipients constitute a specific subgroup within this population, about whose particular experiences very little is known. This paper reports on the knowledge, concerns and motivations of this group of fertility patients and, building on previously published papers from the same study,2,3 discusses the clinical implications of our findings for GPs, fertility specialists and the future of egg donation in the UK.
Egg-sharing is the name given to an arrangement whereby a woman undergoing fertility treatment (IVF or ICSI) donates a portion of her eggs to an anonymously matched recipient in exchange for a reduction in treatment costs. At the London Women's Clinic, egg-share donors only pay an initial consultation (£295) and HFEA fee (£75) associated with their treatment, and receive their IVF for free. Egg-share recipients pay £5760, plus the consultation and HFEA fees. (For both groups, additional services such as ICSI and the use of donor sperm incur additional charges.) The eggs produced by the donor are split equally between donor and recipient. If there are a large number of eggs, one donor may provide for two recipients (the maximum allowed in the UK). If the donor does not develop a sufficient number of eggs to share (usually a minimum of eight), she can choose to abandon that cycle of treatment or to continue with the cycle and keep all the eggs for her own use (in which case the usual IVF fees of approximately £5000 will be payable).
While supporters of egg-sharing argue that it has distinct advantages over ‘non-patient’ donation, such as providing ‘a balance of therapeutic risk and reward’ by removing the need for a healthy woman to undergo ‘ovarian stimulation’, 4 extending access5,6 and promoting ‘altruistic reciprocity’,5,7 critics have been concerned that such schemes may exploit women who are otherwise unable to afford IVF and compromise consent;8,9 that benefits in kind may lead to the commodification of human gametes;10,11 and that egg-share donors whose treatment ends unsuccessfully will be psychologically damaged .12,13 Despite these debates, such schemes have been regulated in the UK since 1998 14 and, according to figures from the HFEA, since 2002 egg-share donors have constituted the majority of British egg donors, where the principles of cost-neutrality and non-anonymity have attracted few non-patient donors. 15 In fact, the UK is said to be suffering from an acute ‘donor shortage’, 16 leading to long waiting lists and very limited choices (e.g. regarding phenotypic matching) for those seeking donor eggs, resolved in some cases by recourse to cross-border reproductive care (CBRC) in destinations where eggs are more readily available . 17 The possibilities and challenges of CBRC have been discussed elsewhere 18 and for the purposes of this paper, suffice it to say that a desire to recruit more donors in the UK and to make the best use of donations was a central concern of the HFEA's recent review of gamete donation policies.19,20 Following the review, egg donors can receive up to £750 compensation per cycle (replacing the previous cap of £250 for loss of earnings plus expenses). This has been presented as an ‘attempt to remedy the shortage of donors and to reduce the numbers of infertile women going abroad to countries where regulation may be less strict, while not tempting vulnerable women to donate for financial reasons’. 16
However, this policy change targets non-patient egg donors only, and beyond the decision to allow egg-sharing to continue, no discussions took place on whether or how recruitment of patient donors should be optimized. This oversight may be explained in part by the contentious history of egg-sharing and in part by the limited knowledge that has been available about egg-sharers, both of which are addressed by this study. One of the central debates regarding the practice of egg-sharing has pivoted on questions around egg-share donors’ motivations. Although the HFEA's initial decision to regulate egg-sharing was based on their conviction that ‘egg-sharers are not motivated by money, but by the desire for a baby’ 14 critics have remained concerned that the benefit-in-kind could form a financial incentive8–11 . While it is clear that egg-share donors form a specific subgroup whose motivations, attitudes and experiences cannot be deduced from data on other types of donors (e.g. volunteer donors, commercial donors, known donors or non-compensated patient donors as discussed in a systematic review by Purewal and van den Akker, 2009), 1 very few studies have involved egg-sharers. The limited empirical evidence available has suggested multifactorial motivations for egg-share donors, often including the desire to help themselves and to help another5,7,21,22 but remains inconclusive on how different motivations are constituted, and on many of the broader questions surrounding egg-sharers’ experiences. Focusing not just on egg-share donors but also on egg-share recipients, the present study obtained empirical data on the knowledge, motivations and concerns of these women, and assessed the implications of the findings for policy and clinical practice.
Methods
Data for this study were gathered by questionnaire. There were two versions of the questionnaire: an interactive online version and a traditional paper version. The content was based on issues raised by a literature review of the field. The questionnaire was developed through extensive piloting: in the first stage it was tested by non-egg-sharers for functionality and by nurses involved in the delivery of egg-sharing for sensitivity; in the second stage volunteers who had taken part in egg-sharing at the Swansea, Cardiff or Darlington branches of the London Women's Clinic completed the questionnaire and fed back comments to the researchers for further improvement. Ethical approval for the study was obtained from the Cambridge University Psychology Research Ethics Committee.
All potential participants for whom current contact details were available were invited to participate in the study. They were initially contacted either by letter or by telephone by a member of staff from the London Women's Clinic in 2010. Those who expressed an interest in participating in the study were either e-mailed a link to the online version of the questionnaire or sent the paper version, depending on their stated preference. Each woman was telephoned approximately one month after being sent the questionnaire, reminded about the study and asked to submit their completed responses if they had not already done so. For reasons of anonymity, the study team had no means of telling which of the women had or had not already sent their responses. All data were analysed independently at the University of Cambridge Centre for Family Research.
Sample
The study population included all women who took part in egg-sharing (either as a donor or recipient) at the London Women's Clinic (Harley Street branch) in the years 2007, 2008 or 2009. This cohort was chosen as the women had undergone egg-sharing after the removal of donor anonymity and had some time to retrospectively reflect on their treatment. The London Women's Clinic conducts the greatest number of egg-share cycles in the UK, around one in nine of all cycles for the years in question (personal communication). Of the 246 women who fulfilled the inclusion criteria, the contact details for 72 were no longer active. Of those for whom current contact details existed, 35 could not be reached despite several attempts. This left a potential sample of 139 egg-sharers who were invited to take part in the study. Of these 31 declined to participate. The remaining 108 women were sent copies of the questionnaire.
From these 108 women, 102 returned a completed questionnaire. However, as 16 were eliminated due to late arrival and partial or incorrect completion, only 86 questionnaires were included in the final analysis. This represents a response rate of 62% (86 out of 139), which is high considering the sample characteristics, subject of study and length of the questionnaire. The sample comprised responses from 48 donors and 38 recipients.
Although efforts were made to ensure a representative sample, the study respondents were more likely to have successfully conceived through egg-sharing than expected from clinical success rates for the relevant years at the London Women's Clinic indicate (personal communication). Of the 86 respondents, 63% (54 respondents, comprising 31 donors and 23 recipients) had conceived children through one or more cycles of egg-sharing. This is higher than the 42% success rate for the overall population of egg-sharers in the same years (63 out of 124 donors and 41 out of 122 recipients). The discrepancy between these figures may be explained in several ways. Firstly, the clinic was more likely to have current contact data for those women who had given birth after egg-sharing. This is due both to the increased attendance of successful egg-sharers at the clinic and their greater likelihood of keeping in contact with the clinic. It is also possible that women who were successful through egg-sharing were more likely to see it as a relevant aspect of their lives and, therefore, take part in this research.
Measures
The online and paper versions of the questionnaire had the same content and comprised the following 13 sections:
Background information; Relationship status and family life; Route to egg-sharing; Circumstances of egg-sharing; Information and communication about egg-sharing; Experiences in the clinic; Motivations for egg-sharing and concerns about egg-sharing; Information and preferences about donor/recipient; Thoughts and feelings about donor/recipient; Thoughts and feelings about the recipient's children; Disclosure and relationship with your child; Retrospective assessment of egg-sharing; The regulation of egg-sharing and assisted reproduction.
Each section contained between 10 and 12 questions, including a mixture of multiple-choice and open-ended items. While the former enabled direct comparisons across standardized response options, the latter allowed respondents to express themselves as they wished. Sections 1-6 and 12-13 were the same for all respondents. Sections 7-11 were constructed differently for donors and recipients as necessary, although efforts were made to ensure that where possible questions were in parallel and could facilitate comparisons. Section 11 was only applicable to respondents who had ‘successfully’ given birth following egg-sharing. Respondents who had taken part in multiple cycles of egg-sharing were requested to complete the questionnaire, where appropriate, with reference to their first cycle. However, the question regarding whether or not they had a child through egg-sharing was, necessarily, applicable to their overall experience. Thus, it is important to be aware that some respondents classified as ‘successful’ may have taken part in multiple cycles of egg-sharing, and may have had previous unsuccessful experiences (including miscarriages following initial conception).
For most of the participants, the questionnaire took between 45 minutes and two hours to complete, depending on the extent of their responses to the optional open-ended items. Quantitative data from the study were analysed with SPSS (version 19) using t-tests, chi-square tests or Fisher's exact tests as appropriate. Qualitative data were thematically analysed using the software Atlas.ti (version 5.2). This paper presents findings from sections 5, 6 and 7 of the questionnaire only. Data from sections 1 to 4, 12 and 13 2 and 8-11 3 have been published elsewhere.
Results
The results presented here are organized into three thematic sections: (1) knowledge about egg-sharing; (2) motivations for egg-sharing; and (3) concerns and anxieties about egg-sharing. It should be noted that not all respondents answered every question. Unless stated otherwise, the percentages for each response are derived from the total numbers who responded to that particular question.
Knowledge about egg-sharing
Almost all of the egg-share recipients (88.6%) and half of all egg-share donors (44.7%) first found out about the existence of such schemes through the IVF clinic. Other relevant sources of information were the Internet and magazines or newspapers. Only 4.3% of egg-share donors and 2.9% of egg-share recipients had first received information about egg-sharing from their GP (see Table 1).
Information about egg-sharing
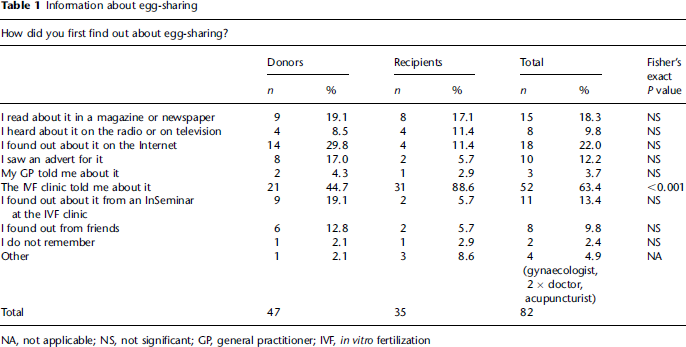
NA, not applicable; NS, not significant; GP, general practitioner; IVF, in vitro fertilization
The study sought to understand the first impressions of egg-sharing by donors and recipients by asking them to choose among 10 possible response options. For the majority of egg-share donors, their first impression was that egg-sharing ‘would be a chance to do something special for someone else while having my own treatment’ (80.4%), that ‘it was a good idea’ (78.3%), and that ‘it sounded like something I would like to do’ (56.5%). A third of both egg-share donors and recipients, ‘thought it was an obvious solution’ (34.6%). Interestingly, while the majority of recipients felt that egg-sharing was their only option (54.3%), contrary to concerns, this was only true for a small minority of donors (6.5%; Fisher's exact, P< 0.001; see Table 2).
First impressions
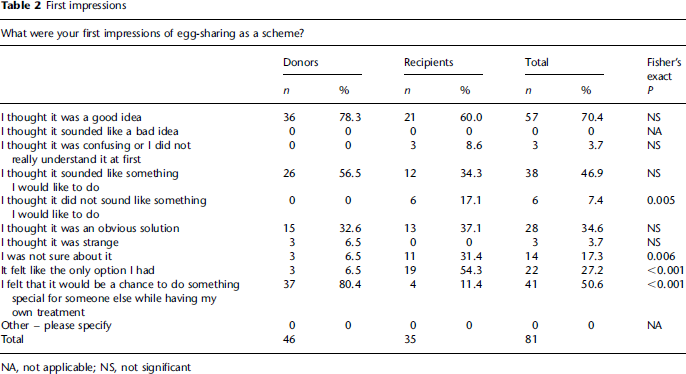
NA, not applicable; NS, not significant
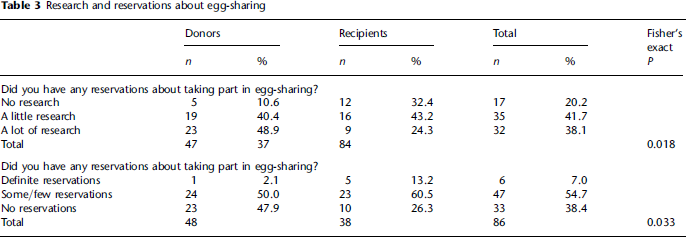
As shown in Table 3, egg-share donors reported undertaking a greater amount of research than egg-share recipients before taking part in the scheme, and were less likely to have reservations regarding their participation (Fisher's exact P = 0.018 and P = 0.033, respectively). Both egg-share donors and recipients discussed the scheme with relevant others before taking part. Key individuals with whom they communicated were partners (where applicable, 85.4%) and the IVF doctor (73.2%). Some women also discussed it with a variety of family members and friends. Our results indicate that counsellors (46.3%), GPs (20.7%) and support groups (6.1%) may be under-utilized by those considering egg-sharing (see Table 4). Since the HFEA requires all egg donors to receive implications counselling, these figures may be more indicative of donors’ feelings regarding communication rather than whether or not they attended a counselling session. Detail provided in optional open-ended items by some egg-share donors and recipients expressed frustration that they had not been made aware of egg-sharing earlier, either by their GPs or National Health Service (NHS) consultants:
Research and reservations about egg-sharing
Communicating about egg-sharing
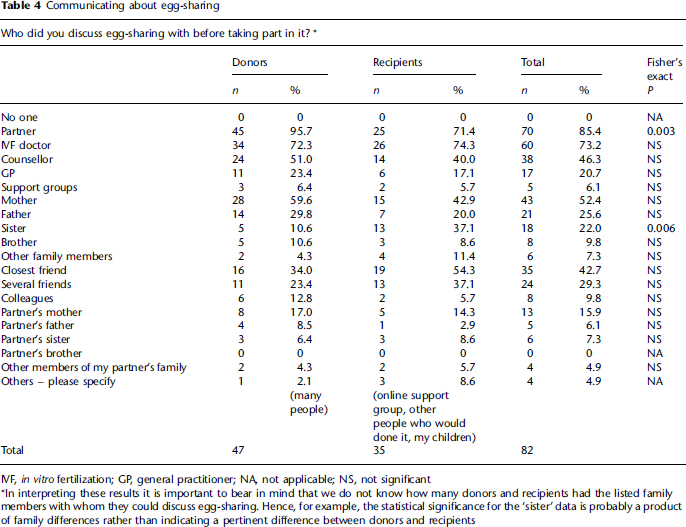
IVF, in vitro fertilization; GP, general practitioner; NA, not applicable; NS, not significant
In interpreting these results it is important to bear in mind that we do not know how many donors and recipients had the listed family members with whom they could discuss egg-sharing. Hence, for example, the statistical significance for the ‘sister’ data is probably a product of family differences rather than indicating a pertinent difference between donors and recipients
I think it is a shame that my NHS consultant didn't tell me about it. I only found out about it when researching on the Internet where we could get the cheapest IVF treatment. (Donor)
Motivations for egg-sharing
Both donors and recipients were asked about their motivations for taking part in egg-sharing. For both donors and recipients, the desire to have a child was a key motivator (87.2% and 96.4%, respectively). Although similar in this regard, there were important differences between the motivations of donors and recipients. For donors, an equally important motivation was to obtain a cheaper treatment (87.2%) as well as the wish to help someone else have a child (66.0%). Interestingly, 21.4% of egg-share recipients were also motivated by a desire to help someone else to have a child (see Table 5).
Motivations
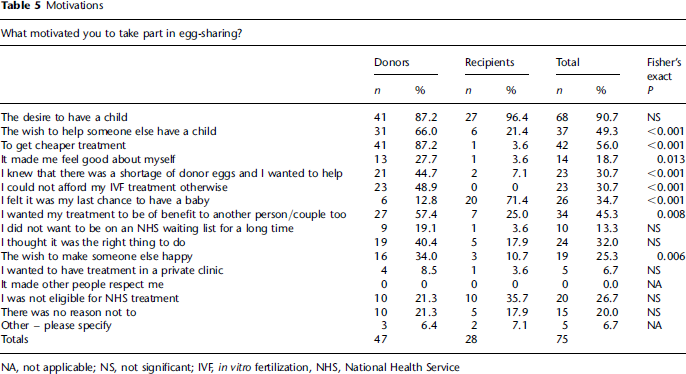
NA, not applicable; NS, not significant; IVF, in vitro fertilization, NHS, National Health Service
Large numbers of both donors and recipients elaborated further on their motivations to egg-share in response to optional open-ended questions. Two recipients articulated their preference for egg-sharing over other forms of egg donation (including CBRC) in the following ways:
Taking part in the egg-sharing programme made me feel most comfortable because the donor went through the whole procedure mainly for herself and not only for me. So any health risks involved she took mainly because she wanted to get pregnant herself.
The reason I initially went with egg-share in the UK was to have an ID release donor whom the child could contact when it grew up. I felt this was probably in the best interests of the child.
Several others made remarks relating to the egg-share donor's motivations, of which this statement is typical:
I liked the idea of the donor wanting a baby also and not just buying an egg.
Many egg donors spoke of a need to balance the financial constraints of their situation with their desire to help another, and thus their feeling that egg-sharing provided the best option for them:
Egg sharing was the best option for me for two reasons. The first being that… I realized someone who could not even produce their own eggs would be suffering more than I. The second, it would also help with the costs of this treatment.
We made our decision 50-50 on altruism and financial support.
The issue of treatment access was raised by several donors and recipients: women bemoaned their inability to receive treatment within the NHS and made a plea for the importance of funded fertility treatments. While two donors explicitly reflected that, although happy to help another, they would not have donated if they could have received treatment through the NHS, several others wrote of their desire or happiness to donate regardless of their own financial situation.
It felt right to share - I give blood, I am on the organ donor list and registered on the bone marrow register.
Even prior to knowing about the egg-sharing programme I had discussed with my partner that I would like to ‘give something back’ and wanted to donate. (Donor who was using donor sperm)
For many donors, their decision to egg-share emanated not just from a need to fund their own treatment, but crucially out of an empathy with the potential recipient and her plight:
Egg-sharing seemed like a natural thing to do when we realized that there were many more people out there wanting to have a family like us, but were struggling in other ways that we could help with.
I can empathise completely with my recipient. … we both shared a longing to be a mother and I was more than happy to help another woman realize her dream of having a child.
The idea of reciprocity as integral to an egg-sharing programme was evident in the statements of many donors and recipients who saw themselves as engaged in a two-way relationship:
I just thought it a great way of making IVF a lot more available for the donor and also giving the recipient the chance to become a mother. (Recipient)
It is a system in which two women with the same problem and the same desires help each other to achieve their goal to become a mother. (Donor)
I can give something back by helping the donor financially. (Recipient)
Wonderful women with a meeting of minds without meeting physically - still able to do amazing things for each other. Such a no-brainer solution to the many varied problems of infertility. A real win-win solution - even if one or other DOES NOT get pregnant. (Donor)
Several women mentioned that the clinic had enabled them and their matched donor or recipient to anonymously exchange cards. This gesture was seen to concretize the reciprocity of the relationship. For example, one woman wrote:
I was very grateful that the clinic passed on a card I wrote wishing the recipient good luck and they passed one back to me which I treasure and am extremely grateful for.
In addition to a sense of direct reciprocity between two women, some donors also spoke about a more generalized form of reciprocity. One unexpected finding from this study was the high percentage of donors who were in lesbian relationships (27.1%) 2 and several lesbian donors explained that their decision to donate eggs through an egg-sharing programme was influenced by their need for donor sperm:
We chose to egg-share so that we could help others, especially as we needed sperm from a donor.
Chose to egg-share as we required donor sperm and felt we would like to reciprocate the gesture.
In response to specific questions about their financial circumstances, significant numbers of donors indicated that they would have considered donating some of their eggs even if there was no benefit in kind (38.3%) and regardless of their ability to pay for treatment (54.3%). Only 27.7% of donors said that they would have considered donating eggs to research rather than to another woman (Table 6).
Donors’ views on egg-sharing
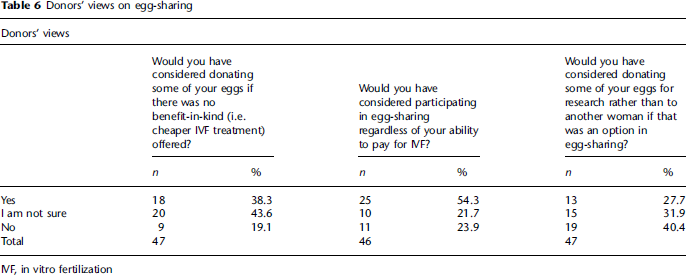
IVF, in vitro fertilization
Concerns and anxieties about egg-sharing
As with motivations, we enquired about donors’ and recipients’ anxieties and concerns about egg-sharing. The main concern or anxiety for almost all donors and recipients was not becoming pregnant (93.8% and 94.0%). Unlike the data on motivations, the anxieties and concerns of donors and recipients were, in general, commensurate. However, there were three significant differences. The worry that not enough eggs would be collected, although important for both donors and recipients (77.1% and 94.4%), was a greater concern for recipients (Fisher's exact, P = 0.030), who were also concerned about the donor changing her mind (P = 0.001). In turn, while the majority in both groups were concerned about being disappointed (72.9% and 62.4%), almost half of the donors (43.8%) were also anxious about disappointing the recipient (P < 0.001; see Table 7).
Concerns and anxieties
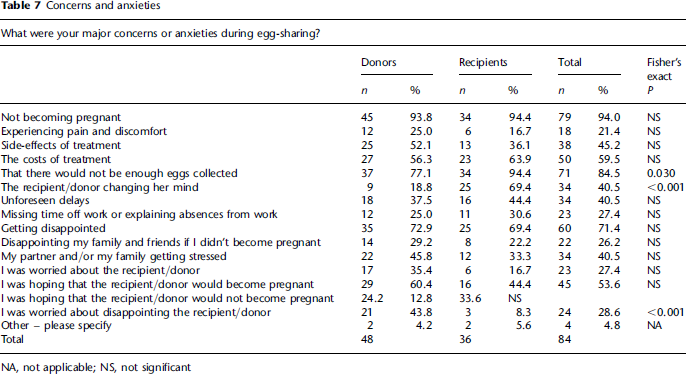
NA, not applicable; NS, not significant
The responses of those women who completed open-ended items varied somewhat. Although most donors and recipients reported positive experiences throughout, some did not. Two donors who reported negative experiences attributed these directly to their participation in the egg-sharing programme, as they perceived their care to have been altered:
I believe that they over-stimulated me because they knew I was an egg-sharer. If I bad been going it alone 1 don't think they would have kept me on the dose 1 was on.
My symptoms (severe pain, unable to walk, sleep, bend) were minimized and 1 was made to feel like a hypochondriac. After my negative pregnancy test, there was no follow-up call. It felt like you've given us your eggs - job done.
In response to the very general question ‘Is there anything you would like to tell us about your clinical experiences?’, by far the most common aspect noted by respondents (whether positively or negatively) was their communication with the clinical team. Whether this was the ease of getting in touch with staff on the telephone, the accessibility of the information received, or the perceived personal interest shown by staff, communication was reported as a key factor in defining their experiences by 59% (13/22) of respondents who answered this question.
Discussion
The motivations, in particular of donors, for participating in egg-sharing schemes have formed a central area of ethical debate around this practice. The findings of this study corroborate the HFEA's initial statement, made as a justification of their decision to regulate rather than ban egg-sharing, that ‘egg-sharers are not motivated by money but by the desire to have a baby’. 14 Indeed, the desire for a baby is a very strong motivator for both donors and recipients taking part in these schemes. However, the findings also show that egg-share donors’ motivations are multidimensional and include financial considerations, and thus support the findings of earlier studies regarding the co-existence of egg-share donors’ desires to help themselves and also to help another.5,21,22 In fact, the great majority of our respondents - both donors and recipients - reported having multiple motivations and provided nuanced details in their qualitative answers of concerns and considerations about egg-sharing that were important to their decision-making process.
For recipients, these included concerns for the best interests of the child, which they felt would be best served through non-anonymous donation; concerns for the health and welfare of donors and a desire to avoid imposing unnecessary health risks on others for the sake of one's own treatment; and concerns about commodification of eggs, which were eased by the idea of ‘the donor wanting a baby and not just buying an egg’. Many donors highlighted their sense of empathy towards potential recipients ‘wanting to have a family like us’ and with whom they shared a ‘longing to be a mother’. For some donors egg-sharing offered a practical option, enabling them to address their financial concerns while helping another. For others, the decision to egg-share was made independently of their financial situation, informed to a greater extent by broader attitudes towards donation and reciprocity. In fact, for both recipients and donors, reciprocity was invoked as an important aspect of egg-sharing. Whether it was the direct reciprocity of helping to fund the treatment of a woman who provided them with donor eggs (as in the case of recipients), or the more generalized reciprocity of contributing to a pool of donor gametes from which they had benefited (as in the case of some donors), both recipients and donors felt that egg-sharing provided them with a valuable opportunity to ‘give something back’. These insights go beyond previous findings, not only by providing more detail about the multiplicity of motivations, but also by enabling comparisons between donors and recipients, and by highlighting the importance of reciprocity for both.
The study also reveals details regarding how donors and recipients come to acquire knowledge about egg-sharing; with whom they discuss their options; and what their concerns and anxieties are about taking part in egg-sharing schemes. The IVF clinic is the main source of information for most egg-sharers, followed by personal research on the Internet or in magazines and newspapers, with very little information obtained from GPs or other medical practitioners. This latter finding is very relevant since we know that GPs are a widely consulted source of information and advice by women who have trouble conceiving. Moreover, although we do not have detailed data from this study regarding the precise nature of the information that women were accessing from the Internet and from magazines, we do know that these fora can sometimes be confusing, inaccurate and biased, and are often beyond the reach of regulation. The fact that several of our respondents were frustrated not to have found out about egg-sharing earlier, through their GPs or NHS consultants, suggests that women saw these professionals as appropriate sources of information. Indeed, medical professionals, with their expertise and ethical commitments, are in a good position to impart reliable, impartial information to women who have trouble conceiving, not only regarding the existence of egg-sharing schemes, but also more broadly about options that are available to them and the health considerations of various reproductive technologies.
As expected, our study found that the main source of anxiety for both donors and recipients in egg-sharing schemes was not becoming pregnant. However there were additional specific worries for donors, such as concerns about disappointing the recipient, and for recipients, such as not enough eggs being collected or the donor changing her mind. We have some indication that egg-share donors may attribute negative experiences to their participation in the scheme, and would therefore encourage clear communication by clinic staff regarding whether - and if so, how - a donor's treatment is altered by the egg-sharing process. In addition, it is clear that patients regard communication with clinic staff (from receptionists to nurses to specialists) as a key aspect of how they evaluate their experiences, and clinics should therefore pay particular attention to this aspect of their care provision.
Having addressed important gaps in information regarding the knowledge, motivations and anxieties of egg-share donors and recipients; as well as egg-sharers’ circumstances and retrospective reflections on consent and exploitation; 2 and the feelings of donors and recipients about each other, each others’ treatment outcome and any resulting children, 3 the study makes an important empirical contribution to debates that are normally dominated by normative arguments. We have been able to reveal details of how egg-sharers perceive their own experiences, what they deem to be the important aspects of their treatment, and their judgements on a range of ethical, practical and emotional considerations. However, it is our hope that ethicist colleagues will also engage with these data to provide deeper theoretical and conceptual analysis of the themes of, for example, exploitation, reciprocity, altruism, commodification, consent and coercion as they pertain to the specific case of egg-sharing, and that as such we may contribute to broader interdisciplinary conversations on these important topics.
Strengths and limitations
This is the first study since the removal of donor anonymity in the UK in 2005 to enquire about the knowledge, motivations and concerns of egg-share donors and recipients. It is also the first study enabling direct comparisons between egg-share donors and recipients, revealing their similarities and differences on a range of factors. The use of online and postal questionnaires enabled disparate participants to be accessed, allowed participants to complete the study in their own time, and were an efficient means of data collection. The range of questions, combining multiple-choice and open-ended items, has allowed both statistical analysis of quantitative data and a more in-depth examination of certain elements that can only be provided by qualitative data. However, although opportunities were provided for respondents to complete open-ended items in their own words, these are not a substitute for face-to-face interviews, which would have allowed the researcher to explore emerging themes, to obtain much more detailed information, and to pursue any inconsistencies or topics of further interest.
One of the main limitations of this study was its relatively small sample size (n = 86), and the potential for bias within this sample. This was due to the difficulties encountered in trying to contact the study population, many of whom proved impossible to reach (as described in the Methods section). Of those who could be contacted, the 62% response rate is high considering the retrospective study design, sensitivity of the topic and use of questionnaires. 23 Due to the nature of the study, it is worth bearing in mind that potential respondents with stronger opinions (either positive or negative) may have been more likely to respond. Perhaps unsurprisingly, we also had a higher proportion of successful egg-sharers responding to the study than the clinical success rates for the same period indicate. An additional limitation was the recruitment of participants from a single clinic; it is possible that egg-sharing is practised somewhat differently in different clinics, leading to variations in the experiences of egg-sharers. Further research incorporating multiple centres can provide a broader overview of egg-sharing as currently practised throughout the UK.
Conclusions
The findings of this study lead to several conclusions that, we believe, should have an impact on clinical practice and on policy-making. The first of these regards information provision about egg-sharing. Based on findings from the research, which shows IVF clinics to be the main knowledge providers, we would advise the broader availability of information about egg-sharing from a wider variety of sources, such as GPs and other medical practitioners (such as NHS gynaecologists), and also infertility networks and support groups. Currently under-utilized, GPs are in a unique position as an early and repeated point of contact for women having trouble conceiving, and can therefore provide impartial, informative advice about fertility treatment and facilitate greater consideration of the issues involved. While it is crucially important not to pressurize potential donors or recipients, it is equally important to address the paucity of information and the lack of opportunities for such individuals to discuss their options. The second conclusion regards motivations and the ethical implications that may be drawn from these. Clearly, most egg-share donors are motivated by the desire to have a baby, to obtain cheaper treatment, and to help another with whose plight they have empathy. Thus, while informed to an important degree by financial considerations, egg-share donors’ decision to partake in such schemes does not suggest primarily commercial motives. Moreover, our findings reveal the role of empathy and the importance of reciprocity for donors and recipients who take part in egg-sharing schemes. These are ethically reassuring and highly relevant considerations which must be borne in mind in future policy discussions regarding egg donation in the UK. Finally, the findings regarding egg-sharers’ concerns and anxieties lead to the conclusion that clinics should be very clear about aspects of egg-sharers’ treatment that might vary from ‘ordinary’ IVF, that they should be sensitive to the specific worries generated by being a donor or recipient, and that they must recognize the paramount importance of communication as a definitive feature of patients’ experiences.
Within the broader context of donor egg shortages, as well as cutbacks to health services which have led to reduced NHS provision of IVF in some areas of the UK, egg-sharing presents a means for more women to access IVF while simultaneously providing more donor eggs. The sum of findings from this study, reported here and elsewhere,2,3 lead to the conclusion that, with wider information provision and more awareness, egg-sharing schemes could have the potential to elicit more donors and to meet the needs of more recipients, under conditions that are preferential and reciprocal for both sets of women.
Footnotes
Acknowledgements
Ethical approval for the study was obtained from the Cambridge University Psychology Research Ethics Committee. The authors are grateful to all the respondents who took part in this study, and would like to thank Emma Smith from the London Women's Clinic for her help with contacting potential participants. They are also grateful to the three anonymous reviewers for their thoughtful and constructive comments.