
Abstract
Abstract
This final article will summarize the treatments and outcomes of some common cancers, and include examples where the natural history and potential for treatment of different types of cancer can affect the impact that a delay in diagnosis has on causation.
Breast cancer
Cancer of the breast is the commonest malignancy in women, affecting one in 12 during their lifetime. In the majority of women, the diagnosis is made while the disease appears to be localized, but recurrence or dissemination may be detected after an interval apparently free of disease, sometimes many years later. In recent years, the addition of adjuvant systemic hormone therapy and chemotherapy has reduced recurrence rates and increased the likelihood of survival for women with breast cancer, particularly where there is evidence of spread to axillary lymph nodes at the time of diagnosis, and screening mammography has enabled the diagnosis to be made earlier in some women with a consequent improvement in the chance of cure.
The majority of women present with a breast lump, although only one in 10 lumps will be found to be malignant. Alternatively, the diagnosis may be suspected following screening mammography which may also detect premalignant changes (ductal carcinoma in situ). The diagnosis is made by triple assessment, a combination of physical examination, mammography and/or ultrasound scan and fine needle aspiration cytology. If localized breast cancer is confirmed, the tumour and surrounding breast tissue are removed, if possible by wide local excision, and at the same time tissue from the axilla is usually removed to examine whether or not lymph node spread has already occurred. If initial surgery fails to remove the tumour completely, or there is evidence of remaining ductal carcinoma in situ, a wider excision is necessary and mastectomy may be advisable in about one-third of women with breast cancer, sometimes followed by reconstruction of the breast.
Wide local excision of breast cancer is usually followed by local radiotherapy to the remaining breast in case there are residual cancer cells or premalignant areas that have not been detected. In this way, the likelihood of recurrence is reduced to a similar level as achieved by mastectomy (some women choose to have mastectomy to avoid the need for radiotherapy). If there is thought to be a high chance of local recurrence, for example due to proximity of the tumour to the deep margin of excision or the presence of metastases in the axillary lymph nodes, postoperative radiotherapy may also be given following mastectomy. The stage of the breast cancer is usually confirmed by histological examination (Table 1).
Clinical staging of breast cancer
In the last 10 years, it has become standard practice to offer adjuvant systemic therapy since this has been shown to reduce the likelihood of recurrence and improve the chances of long-term survival. The greatest benefit is seen in women under the age of 50 years where there is spread to axillary lymph nodes at the time of diagnosis. For women with no involved axillary lymph nodes, survival is increased to a lesser extent by chemotherapy. Adjuvant chemotherapy also benefits women over the age of 50 years, and there is improved survival with the addition of adjuvant Tamoxifen for five years. In premenopausal women with oestrogen receptor positive tumours, there may be an additional benefit from hormone therapy after chemotherapy.
The potential benefit of treatment in an individual patient can be predicted using one of the large databases of patients treated over the years (such as the Nottingham Prognostic Index [NPI] or Adjuvantonline).
Although the use of adjuvant therapy has brought about a gratifying reduction in morbidity and mortality from breast cancer (Figure 1), about half will eventually develop metastatic disease which is incurable.
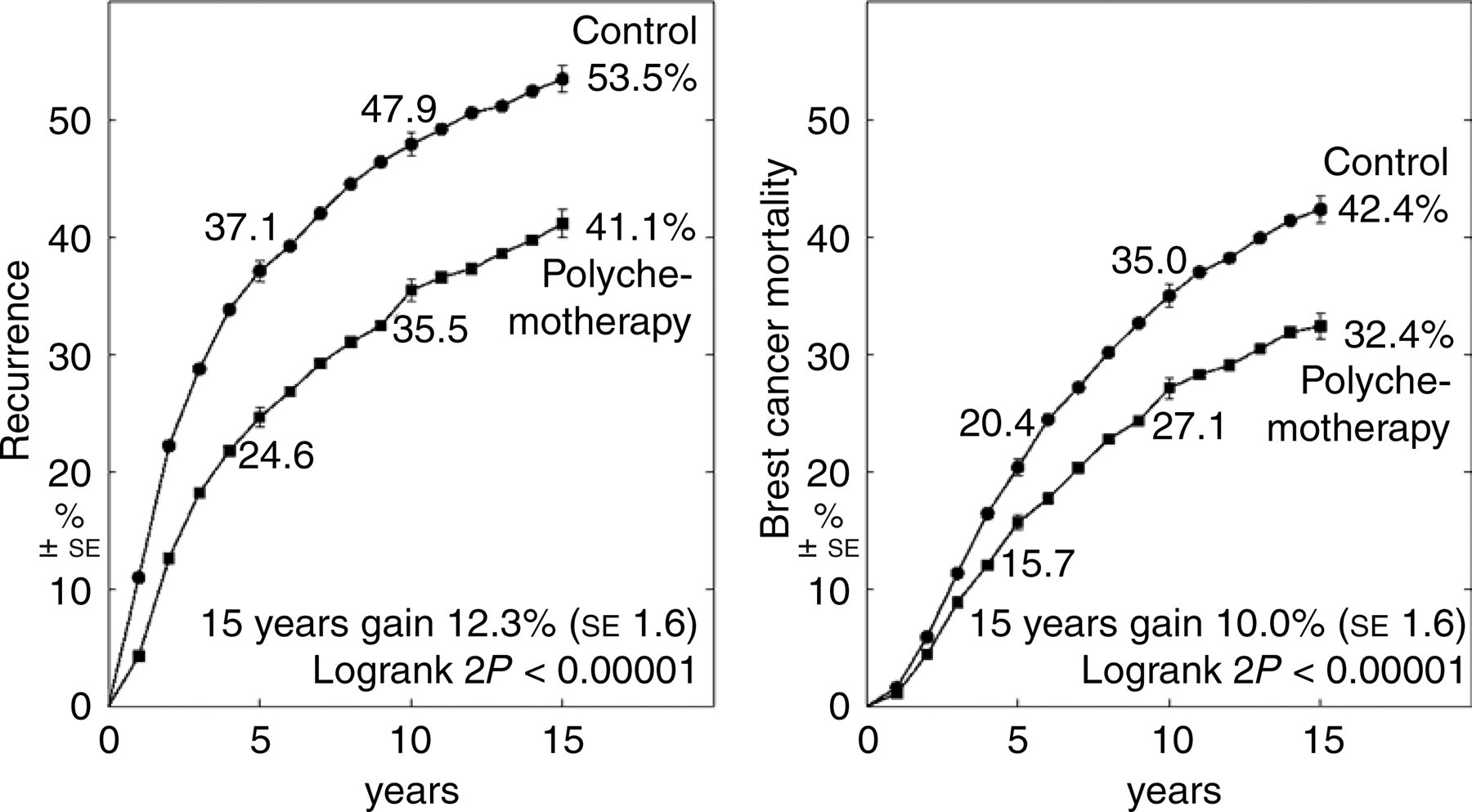
Polychemotherapy versus none: 15-year outcome (life-table curves by entry age). (A) Entry age, <50 years old (6901 women: 35% N+); (B) entry age, 50–69 years (18,629 women: 70% N+)
Useful remissions may be achieved by local radiotherapy, hormone therapy or chemotherapy. Local recurrence may be curable by surgery and/or radiotherapy in selected cases, and may also be treated by systemic therapy in view of the possibility of more widespread disease.
Medicolegal examples
Janet, aged 31 years, consulted her general practitioner (GP) as she had found a small painless lump in her breast. The GP examined her and reassured her that it was a ‘cyst’ and did not refer her for investigation because he thought she was ‘too young’ to have breast cancer. Janet became pregnant about three months later and just before her baby was born she noticed that the lump had grown. Janet was referred to a breast surgeon who confirmed the presence of cancer and performed a mastectomy and axillary dissection which showed a moderately differentiated adenocarcinoma with no metastases in 10 lymph nodes. She received chemotherapy after her baby was born and also received Tamoxifen as her tumour contained oestrogen receptors.
If Janet had been referred a year earlier, the tumour would have been smaller but her prognosis (based on the NPI) would have been about the same. As there were no metastases in the lymph nodes, she was in the same NPI category both at the time of treatment and a year earlier and still had approximately a 60% chance of living for more than 15 years.
Elizabeth, aged 58 years, was having regular screening mammograms every three years and had been told that they were normal. However, two years after the most recent mammogram, she found a lump in her breast and consulted her GP. She was referred urgently to a breast surgeon who diagnosed cancer of the breast and she had a wide local excision and axillary dissection. Histology showed a grade 3 poorly differentiated ductal carcinoma with metastases in two lymph nodes and she received postoperative radiotherapy and chemotherapy. Retrospective review of the mammograms taken two years earlier revealed some calcification in the position where the cancer was found, and it was the opinion of an expert radiologist that the abnormal calcification should have been noted and the breast surgeon informed about the suspicious findings. This would have enabled the diagnosis of breast cancer to have been made two years earlier, when on the balance of probabilities, Elizabeth's cancer would not have spread to the lymph nodes and her prognosis would have been significantly better.
Cancer of the colon and rectum
Cancers of the colon and rectum are the second commonest cause of death from cancer in the western world, accounting for about 15% of all cancers and affecting about 30,000 people each year in England and Wales. Cancer of the bowel is relatively uncommon under the age of 40 years, although inherited gene defects may give rise to tumours at a younger age than usual.
In the early stages, colorectal cancer may not cause symptoms, but a change of bowel habit is the commonest presenting feature, often accompanied by rectal bleeding, or anaemia may develop through occult blood loss. The tumour may cause obstruction of the bowel and this most commonly occurs in the sigmoid colon.
The tumour may be palpable on digital rectal examination, and investigation by flexible sigmoidoscopy or colonoscopy and barium enema may be necessary if the diagnosis cannot be made with rigid sigmoidoscopy. Carcinoembryonic antigen levels may be raised in the blood, which can then be used for monitoring the response to treatment.
The initial treatment of colorectal cancer is surgery wherever possible, removing the tumour and adjacent lymph glands. Histological examination will enable pathological staging, as shown in Table 2.
Pathological staging in cancer of the colon and rectum
Most tumours are adenocarcinomas which may be well or poorly differentiated, the latter often having a higher tendency to spread and a worse prognosis. Distant spread may occur to the liver or lungs, as happens in over 40% of patients in stage Dukes C (where there is histological evidence of spread to the lymph glands).
In the last 10 years it has become standard practice to give adjuvant (insurance) chemotherapy to patients with Dukes C tumours, with an anticipated 7–10% increase in long-term survival. It would therefore appear that some patients with microscopic (occult) spread to the liver may be cured by chemotherapy given prior to the detection of metastatic disease.
Where there is evidence of distant spread at the time of diagnosis, or which develops subsequently after initial treatment, useful palliation may be achieved by chemotherapy, with an average improvement in survival of about 5 months, although cure is not possible. Standard adjuvant and palliative chemotherapy is a combination of 5-fluorouracil and folinic acid, but newer agents such as Capecitabine, Irinotecan, Oxaliplatin and Avastin have shown promise in the treatment of metastatic disease. Radiotherapy may be used in combination with curative surgery for rectal cancer, and has a limited value in palliation of localized metastases.
The proportion surviving for five years after treatment are shown in Table 3.
The proportion surviving for five years after treatment
Medicolegal cases
Mary, aged 58 years, was finding her job very stressful and consulted her GP as she had noticed some rectal bleeding and her bowels had become loose recently. He examined her and found piles for which he gave her cream, and suggested that her bowel problem was due to stress and she should consider retirement. Mary coped with her bowels, but thinking that the continuing stress was causing her symptoms, she retired nine months later. However, her bowel problems continued and she began to lose weight. She saw her GP again three months after retiring as she was no better, although she was happier, and he referred her to a colorectal surgeon. A moderately differentiated adenocarcinoma of the large bowel with multiple metastases in her liver was diagnosed which was not curable and she received chemotherapy.
As there were numerous liver metastases, and some were several centimetres in diameter, it is likely that they had been present for more than a year and earlier referral and surgery would not, on the balance of probabilities, have prevented spread to her liver or enabled her to be cured.
John, aged 39 years, was especially anxious when he consulted his GP about the recent rectal bleeding he had noticed, as his father and grandfather had both died from bowel cancer. He was referred urgently to a surgeon and the examination in the clinic showed that he had piles. John was admitted to hospital three weeks later for a more thorough examination of his bowel and treatment for piles. It was not possible to pass the colonoscope beyond the mid-transverse colon but there were obvious piles which were ‘banded’. The bleeding settled and John was discharged from routine follow-up when he attended the surgical clinic six weeks after the examination. However, John still saw blood in his motions from time to time, but did not report this to his GP as he thought it was the piles.
A year later, John was feeling very tired and his GP arranged a blood test which showed that he was anaemic. The GP tested him for occult blood in his motions and as this was positive he was referred back to the surgeon. Examination showed no obvious bleeding from piles or in the lower bowel but barium enema showed a tumour in the ascending colon, beyond the area examined by colonoscopy a year earlier. The tumour and right side of John's bowel were removed and histological examination showed a poorly differentiated adenocarcinoma with small metastases in two lymph nodes close to the bowel. He received adjuvant chemotherapy and had no sign of recurrence or metastases two years afterwards.
The hospital admitted that following the initial incomplete examination, either a barium enema or repeat and full colonoscopy should have been arranged, although John was young, in view of his family history of bowel cancer. It was agreed that owing to the delay in diagnosis, John's cancer had been allowed to spread, resulting in the need for chemotherapy and a reduction in his life expectancy.
Carcinoma of the lung
Cancer of the lung is the commonest cause of cancer death in men in the UK, affecting 23,000 men and 11,000 women each year. It is becoming increasingly common in women, with over 7% of cancer deaths due to lung cancer. The commonest presenting symptom is coughing (about 70%) with dyspnoea (shortness of breath), haemoptysis (coughing up blood) and chest pain being present in nearly half the patients as well. Lung cancer is also frequently associated with fatigue and weight loss, which occur in over 50% at presentation.
The diagnosis is usually made by an abnormal shadow on chest X-ray, confirmed by CT scan and bronchoscopy with biopsy. Clinical staging is shown in Table 4.
Clinical staging of carcinoma of the lung
There are four main histological types: squamous cell carcinoma accounting for over 50%, small cell carcinoma accounting for about 20%, large cell carcinoma about 20%, and adenocarcinoma and other variants the remaining 5–10%. Small cell carcinoma is almost always widely disseminated at diagnosis, and responds well to both chemotherapy and radiotherapy, so is normally treated medically rather than surgically. The remaining ‘non-small cell carcinomas’ are treated by surgical resection if the tumour is localized and sufficiently peripheral to achieve complete removal. If lymph glands in the mediastinum (middle of the chest) are affected or there are distant metastases, cure is not possible. Only approximately 20% of all patients presenting with lung cancer are suitable for curative surgery. Patients with stage I disease (T1N0 and T2N0) have a slightly greater than 50% chance of living for more than five years after surgery alone. The majority of patients have locally advanced or metastatic disease at presentation and may benefit from palliative radiotherapy and/or chemotherapy. Although there is some evidence that treatment improves the survival of patients with locally advanced tumours by a few months, there is still little evidence that any therapy improves survival of patients with recurrent or metastatic lung cancer.
In summary, the outlook for carcinoma of the lung is generally poor. On the one hand, some patients with adenocarcinomas may live for several years in view of the relatively slow growth of these tumours, but the majority of patients with non-small cell carcinoma die within a year of diagnosis owing to the highly malignant nature of these tumours and their tendency to disseminate before the diagnosis can be made.
Medicolegal cases
Gerry, aged 56 years, had smoked 20 cigarettes a day for many years and was due for a hip replacement. A routine chest X-ray before the operation showed a shadow at the apex of his right lung but this was not noticed by the anaesthetist or surgeon. The X-rays were not reported by the radiologist as they were filed away soon after Gerry had left hospital. Nine months later, Gerry had upper right chest pain and his GP arranged an X-ray which showed a tumour of the upper part of his right lung.
The hospital then realized that the previous X-rays had been overlooked and that the diagnosis should have been made nine months earlier. However, the tumour was infiltrating the chest wall at the time of diagnosis and published results showed that this type of tumour (superior sulcus tumour) would probably not have been cured by surgery.
Anthea, aged 65, had never smoked and rarely saw her GP. She was knocked off her bicycle and taken to casualty where a chest X-ray was taken to see if she had any broken ribs. The X-ray did not show any fractures, but there was a small shadow in the base of the right lung which was not noticed by the doctors who were focusing on her bones. Two years later, Anthea had a bad cough and her GP arranged a chest X-ray which showed a large tumour of the right lower lobe. Biopsy confirmed adenocarcinoma of the lung, but it was not operable and Anthea received palliative radiotherapy. Sadly, she died six months later; the hospital agreed that the shadow on the original chest X-ray should have been reported and resulted in referral for investigation, and if she had had surgery two years earlier she would probably have survived.
Carcinoma of the prostate
Adenocarcinoma of the prostate is one of the most common cancers in men and is increasing in incidence. It becomes more common as men get older and may be present in addition to the more common benign enlargement of the prostate. The cancer develops in the periphery of the prostate gland, whereas benign prostatic enlargement principally involves the central zone. Prostate cancer may spread to pelvic lymph glands, especially if the tumour is large or with a Gleason score of 7 or above, and this is associated with a poorer prognosis. Distant metastases to the skeleton are common, especially from poorly differentiated tumours.
Tumours may be well differentiated, moderately or poorly differentiated, the latter carrying a much worse prognosis than the better differentiated lesions. Gleason proposed a prognostic classification system which is based on the differentiation of the tumour seen in two representative samples from different parts of the gland. Patients with Gleason scores of 2–4 have well differentiated tumours with an excellent prognosis. Those with Gleason scores of 5–7 have moderately differentiated cancers and an intermediate prognosis. Tumours with a Gleason score of 8 are usually rapidly growing, poorly differentiated tumours, generally with a poor prognosis.
Patients with localized prostate cancer are often free of symptoms, or may have only mild urinary symptoms, which sometimes are thought to be due to benign enlargement of the prostate. Large malignant tumours may produce more obvious obstruction causing frequent nocturia, hesitancy and a narrow stream. Some patients present with pain due to bony metastases.
The diagnosis of prostate cancer is made by digital examination and biopsy guided by transrectal ultrasound, together with prostate specific antigen (PSA) estimation and bone scan to look for distant metastases. If the PSA is below 20 and the tumour appears clinically localized, a magnetic resonance image scan may be performed to evaluate the extent of the tumour and determine whether or not there is spread beyond the prostate gland or lymph node metastases in the pelvis, which would make the cancer inoperable. If radical treatment is being considered, it is now common practice to biopsy the pelvic lymph nodes first to see if there are any metastases. The tumour can then be staged according to the TNM classification of malignant tumours (Table 5).
Clinical stages of carcinoma of the prostate
There is still debate about the optimum management for early prostate cancer, especially in patients with well differentiated tumours who are asymptomatic, with a slightly raised PSA between 10 and 15. It has been difficult to recruit patients into clinical trials which include a ‘no treatment’ option, but there is so far little evidence that early intervention by surgery, radiotherapy or hormone therapy improves survival in patients with well differentiated tumours (Gleason grade <4). Many high grade tumours (Gleason 8–10) are not cured by early intervention, since in the majority, distant spread probably occurs before the diagnosis can be made.
Treatment of early (T1 or T2), localized prostate cancer may be by surgery or radiotherapy. Small tumours, confined to the gland clinically, may be removed by radical prostatectomy which is now possible with the sparing of local nerves, thus preserving potency in the majority. Local radiotherapy may sometimes be given by inserting radioactive sources or more usually by external beam radiotherapy, using carefully shaped fields to reduce the dose of irradiation to normal tissues, in particular avoiding the rectum.
Locally advanced, recurrent and metastatic prostate cancer is usually treated by hormone therapy, by suppressing androgen production from the testis using Zoladex or Prostap, or removing the testes, and/or using an androgen blocking agent such as Cyproterone acetate, Casodex or Flutamide.
The best prognostic indicators in carcinoma of the prostate are clinical stage, pretreatment PSA level and Gleason score. Table 6 summarizes published long-term results with conventional external beam irradiation. The results of treatment of T3 cancer of the prostate are less favourable, as shown in Table 7.
Survival with external-beam irradiation in patients with stage T1b and T2 carcinoma of the prostate
*Overall survival rate (%); disease-free survival (%) in parentheses
†Surgically staged patients
‡Includes T2a tumours
The results of treatment of T3 cancer of the prostate
The Memorial Sloan-Kettering Cancer Centre has derived a nomogram by collation of published results of the treatment of prostate cancer by surgery and radiotherapy, which is used by many oncologists to advise patients on the benefits of the various treatment options. Since this takes account of the PSA level at diagnosis, the Gleason stage and clinical or pathological stage of the tumour, it enables the prognosis to be estimated for individual patients and therefore gives a more accurate prediction of the likely outcome than published series reporting results by stage without stratifying for Gleason stage or pretreatment PSA level. As a result, the survival figures quoted for all patients (well and poorly differentiated) are generally better than for poorly differentiated (high Gleason grade) tumours alone.
Medicolegal cases
As Eric was 60 years old he had a routine check-up with his GP. Examination was normal and the GP arranged blood tests including PSA which was 17, but through an administrative error the abnormal result was over-looked by the surgery. Eric did not know about the raised PSA and thought the tests had been normal. He next consulted his GP again a year later when he started to have difficulty passing urine. The GP referred Eric to hospital where a repeat PSA showed 40 and tests showed that he had cancer of the prostate that had started to spread outside the gland. It was not possible for Eric to have surgery, but he was treated with hormone therapy and radiotherapy to his prostate.
He had a poorly differentiated tumour and, according to the nomogram prediction, on the balance of probabilities, he would not have been cured a year earlier. He is currently in remission and his prognosis is probably similar to what it would have been following treatment a year earlier.
David, aged 42 years, noticed that he was having increasing difficulty passing urine and his GP referred him privately to an urologist. Physical and ultrasound examination of the prostate was normal apart from a small cyst on the outside of his right testis, which the urologist removed and this was reported benign. John's difficulty passing urine persisted and the surgeon used prostatic massage, without any lasting benefit. Eighteen months later, David asked to be referred for a second opinion; blood tests showed a raised PSA of 17.5 and examination and biopsy showed a moderately differentiated adenocarcinoma of the prostate. He had a prostatectomy which left a small amount of residual tumour and was therefore followed by external radiotherapy. Two years after completing treatment, David's PSA started to rise, and he is now on hormone therapy and has responded well, but his cancer is not curable.
It was agreed that the urologist should have arranged a PSA when David first consulted him, especially as it later was known that David's brother and grandfather both had prostate cancer, and this test would probably have resulted in the diagnosis being made 18 months earlier. It was agreed that the chance of cure would have been higher if David had been treated while it was at an earlier stage.
Malignant melanoma
Malignant melanoma is relatively uncommon, affecting just over 3000 people each year and representing just over 1% of cancers in UK. The incidence has been increasing in recent years, possibly due to greater ultraviolet radiation exposure on foreign holidays.
More than 90% of melanomas arise in the skin and early diagnosis can be made by recognition of clinical features. The most important features are obvious growth in size and thickness, irregular shape or irregular colour. Other suspicious features include a diameter greater than 7 mm, inflammation, oozing or bleeding, and a change in sensation (usually a mild itch).
The majority of malignant melanomas are superficial spreading melanoma which is generally flat in the early stages. Nodular melanoma accounts for 15–30% of melanomas and often has grown fairly rapidly over a few weeks or months. These lesions may be red, grey or black, but 5% are amelanotic (without pigment). Amelanotic melanomas are more common on the trunk and head and neck, occur more frequently in men and tend to be more aggressive than other types. Rarer forms of melanoma include acral lentiginous melanoma and lentigo maligna melanoma.
Treatment is by wide local excision, with smaller margins (1 cm) for thin primary tumours but more extensive margins (up to 3 cm) for thicker tumours. There appears to be no benefit from elective lymph node dissection, but where there is an obviously enlarged lymph node a radical dissection is performed, removing the regional lymph glands ‘en bloc’. There appears to be no benefit from adjuvant chemotherapy and trials are still underway to evaluate the benefit of adjuvant interferon.
The prognosis depends on the thickness of the lesion, localized melanomas with a thickness of <1 mm being associated with a greater than 90% chance of 15-year survival, but where the thickness is above 4 mm, or the lesion is ulcerated and more than 2–4 mm thick, the chances of 15-year survival fall below 50%. Patients with thick tumours are more likely to have involved lymph nodes. Those with only one node involved have approximately 45% chance of surviving 15 years, but if more than four lymph nodes are involved only about 15% will survive 15 years.
In view of the poorer prognosis of thick lesions, early diagnosis and treatment is important. Moreover, avoiding excessive exposure to ultraviolet light, using a high factor sunblock if necessary, is being encouraged in an attempt to prevent the development of malignant melanoma.
Medicolegal cases
Shirley, aged 45 years, had a mole on her ankle and, as it was unsightly, persuaded her GP to remove it. He thought it was benign, but sent it to the laboratory for histology which the local pathologist thought was abnormal, probably not malignant, but he was sufficiently concerned to advise referral to a dermatologist. The GP referred Shirley to the local dermatologist and sent the report, but she was not offered an appointment. The dermatologist thought that the report was no cause for concern but did not ask for a review of the pathology by an expert in dermatological pathology. Shirley noticed a lump in the scar two years later and was referred to a surgeon. Excision revealed malignant melanoma and review of the previous histology showed a malignant melanoma and confirmed that the new lesion was in fact a recurrence of the undiagnosed melanoma removed incompletely two years before. The thickness of the recurrent melanoma was significantly greater than the first tumour and as a result, the chance of her surviving to 15 years was reduced to <50%.
Paul, aged 21 years, had a mole removed by his GP which was thought to be benign and was not sent for histological examination. Three years later, Paul had a lump in his groin and biopsy showed malignant melanoma. He was referred to a plastic surgeon who removed the glands and widely excised the original scar. There was a metastasis in a groin lymph node, but there was no sign of recurrence in the scar. Although three years had lapsed without appropriate treatment, in view of the fact that there was no local recurrence, the metastasis must have spread before the mole had been removed three years earlier, and therefore the failure to diagnose malignant melanoma had not affected the eventual outcome.