
Abstract

Introduction
There is ample evidence that harm happens frequently to patients in hospital. It is often avoidable and sometimes leads to death. 1–6 There is less evidence to determine whether interventions make a difference to this and if so what interventions may be most effective. 7 Vincent has suggested that ‘Organisations must move towards active measurement and improvement programmes on a scale commensurate with the human and economic costs of unsafe, poor quality care’. 8
The NHS Modernisation Agency (MA) and latterly the NHS Institute for Innovation and Improvement have been working with a group of hospitals striving to apply improvement methods to reduce avoidable deaths and avoidable harm. We were also aware of other hospitals working on this area and determined to evaluate the effectiveness of their interventions on reducing mortality.
Intention of study
The NHS MA ran a programme to reduce avoidable deaths in hospital from 2002 until 2005. Initially this involved three hospitals taking part in the ‘Pursuing Perfection’ programme, 9 which formed a community of practice in 2003, and in 2004 it was extended to cover another 12 hospitals, which were selected because they had a high Hospital Standardised Mortality Rate (HSMR). 10 Of the 12, eight hospitals were active participants. In 2004 the Health Foundation began to sponsor four hospitals across the UK in the ‘Safer Patients Initiative’ (SPI) 11 which similarly set out to reduce harm. Following the publication of hospital mortality rates in 2001, Walsall hospital, which had the highest HSMR at the time, had commenced a programme to reduce mortality. Their improvement work was supported directly by Professor Sir Brian Jarman. The hospitals are listed in Table 1.
Following the closure of the MA and replacement of many of its functions by the NHS Institute for Innovation and Improvement, we set out to evaluate the attempts to reduce mortality in hospitals.
Methods
What was done
The first step was to ask Professor Jarman to assess the impact of interventions in the hospitals in the MA community of practice programme plus Walsall (Table 1a). He analysed the cumulative quarterly HSMR across the 12 hospitals, and demonstrated that HSMR of 112 to 114 up to early 2004 came down to 100 in 2006, a reduction of more than 10% (Figure 1).
The hospitals participating in the Matrix scoping study, overall HSMR calculation and Hospital Exchange Workshop *At the time of study, all were NHS Trusts; many are now Foundation Trusts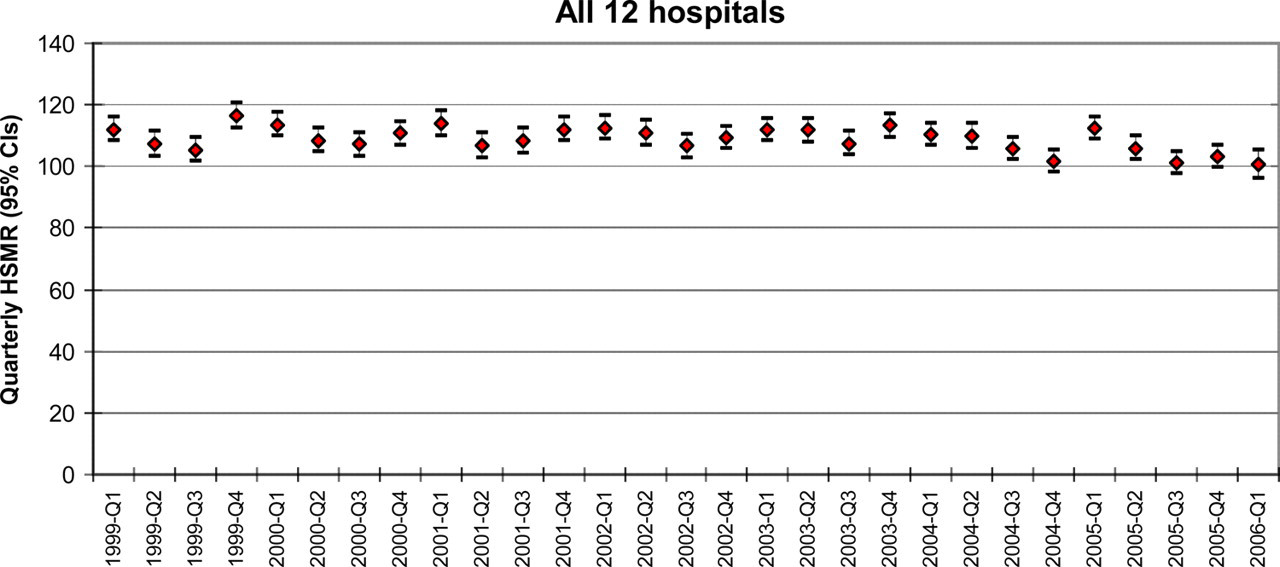
The NHS Institute worked with a research company (Matrix Research & Consultancy) to draw up a structured telephone questionnaire. The responses to the questionnaire were collated and analysed, and published online. Details of the methodology are given in the report ‘Scoping of evidence in relation to interventions to reduce avoidable mortality’. 12
In May 2006 we held a ‘Hospital Improvement Exchange’ workshop in London, jointly sponsored by the NHS Institute and the Health Foundation. In addition to the 11 MA sites and Walsall, representatives also came from the four SPI sites (Table 1b). One Trust, Luton, was a member of both groups.
Hospitals participating in the Hospital Information Exchange in addition to those in Table 1a
The event was structured to share knowledge about what interventions had been implemented, and which seemed to have worked. Expert facilitators established consensus on the most effective strategies.
What was found
Each site started with a local assessment of safety. The first challenge was to convince clinicians of the frequency of errors causing harm, which are estimated to occur in around 10% of patients. 4,6
In the community of practice sites the starting point was a case-notes review of 50 consecutive deaths occurring within the hospital. The audit was made quicker and more effective by using a ‘Trigger Tool’ adapted from one previously proposed by the Institute for Healthcare Improvement. 13 The trigger tool is a checklist of items to look out for during casenotes review and makes it easier to identify errors quickly. Examples of such items include administration of Vitamin K or naloxone, unplanned return to the operating theatre, substantial biochemical abnormalities or significant drop in haemoglobin.
A useful framework to learn which areas need most attention is a 3 × 2 or 2 × 2 matrix, stratifying deaths into those occurring in the Intensive Treatment Unit (ITU) and High Dependency Unit (HDU) versus those in patients admitted to the ward and patients admitted principally for symptom control versus those receiving active treatment. 14
Outputs from the case-notes audit and 2 × 2 matrix were particularly effective in raising awareness of the errors that were occurring in their own hospitals. This helped greatly in engaging staff in improving patient safety.
Issues raised by the case-notes review were augmented by serious untoward incident reports, and by senior executives walking round to visit departments and find out what staff concerns may be (‘executive walk-rounds’). Triangulating these three sources of information yielded more information about differing types of hazard or error.
Table 2 shows the issues we found were most likely to be linked to higher HSMR. This list immediately suggests areas for possible improvement, such as ITU admission criteria, improved end-of-life care systems and the use of care bundles in the ITU. 15 In practice, most activities were focused on improving care on the wards.
Causes of high HSMR established by the Matrix Scoping report 10
What solutions were implemented?
All trusts identified the need to improve timeliness and reliability of care for patients who deteriorate on the ward. It is known that many patients admitted to ITU have been unstable for some time. The NCEPOD report 2005 ‘An Acute Problem?’ showed that the response to a deteriorating patient on the ward was often slow and inadequate. 16 Patients admitted from wards to ITU had been unstable for a mean of 12 hours. In addition, many patient deaths reported to the National Patient Safety Agency (NPSA) through their National Reporting and Learning System are associated with ‘deterioration, not recognised or responded to’. 17
The Trusts found this had been an issue for them and addressed it with a suite of interventions. This began with improving the timeliness and completeness of nursing observations, which were generally very poorly done at the outset, particularly respiratory rate recording. 7 The use of track and trigger tools, such as modified early warning scores (MEWS), 18 was coupled with training for nurses in the management of the sick patient (ALERT), 19 and in assertiveness and communications tools such as SBAR (Situation Background Assessment Recommendation). 20 Then an appropriate response by a critical care outreach service, medical emergency team or hospital at night team completed the implementation. It is evident that no single intervention would make much impact unless all the other components of the system are in place. Further guidance on this issue has now been published by the National Institute for Health and Clinical Excellence (NICE) 21 and the NPSA has published recommendations for implementation. 22
Several sites reported that through the measures above, calls to the critical care outreach team increased and crash calls decreased at the same time (Box 1). Given the very poor outcomes from crash calls in general wards, this would be expected to result in fewer deaths.
All the hospitals involved in the Hospital Information Exchange have been implementing systems to deliver timely care to sick patients on wards. For example, Conwy & Denbighshire Hospitals instigated MEWS scoring and a Critical Care outreach system. The charts below show what happened when the outreach service was expanded. It had been a daytime service from 08:00 until 18:00, five days per week. In February 2006 this was increased to a 24-hour service. The process control charts below show how a substantial increase in calls to outreach was associated with a fall in crash calls. (Results presented at the IHI/BMJ International Quality Forum, Barcelona, April 2007. Charts reproduced courtesy of Delyth Williams.)
Vignette

Some sites identified synergy between work on improving the flow of patients through the hospital with a synchronous reduction in mortality. In East Lancashire, daily senior-led ward rounds, along with other bed management initiatives, resulted in far fewer medical patients outlying in beds allocated to other specialities. At the same time that outliers were eliminated, there was a reduction in mortality equivalent to four lives per week. 23
Other common interventions identified at the ‘Hospital Improvement Exchange’ workshop were:
Infection control measures, especially reliability of hand washing; Introduction of surgical site sepsis care bundles; Other sepsis bundles, such as central venous catheter bundle, ventilator associated pneumonia bundle, etc.;
15
Theatre safety through uptake of briefing and debriefing in theatres, to reduce the impact of human factors in causing errors in surgery; New procedures to reduce drug errors; Improving chronic disease management especially for coronary heart disease and chronic obstructive airways disease.
The scoping report found that aside from the ‘core’ interventions, Trusts adopted a wide array of interventions relating to the appropriateness and timeliness of care, the appropriateness of the setting of care, medicines management, infection control and non-clinical issues such as data quality in coding. Interviewees also identified changes in the attitude of clinical staff to the collection of evidence and an improvement in the reporting of adverse incidents.
12
How did they make change
Trusts supported by the MA used methods from the Model for Improvement. 24 Tests of change were planned and implemented, often on a very small scale (one patient, one clinician) before modifying the intended change to maximize benefits, then scale up to full implementation. This experimental method has proved effective in minimizing the risk of unintended consequences. In practice it means changes can be implemented quickly, with minimal planning and maximal learning. However, this method was not universal – Walsall used a more formal clinical governance structure to address particular specialities or conditions where high mortality was an issue. 25
While the majority of critical success factors identified related to the activities at a clinical team level it was evident that sustainable improvements could not have been achieved without top team sponsorship or a structure to support the implementation of interventions.
Outcomes
Jarman found that the HSMR for the 12 Trusts included within the review had reduced during the 18-month period of intervention (Figure 1). Participants highlighted a variety of other benefits that Trusts had experienced, from a reduction in the length of stay to improved compliance with protocols. A number of Trusts were keen to stress that the whole package of change, rather than any particular intervention, had contributed to changes in organizational behaviour and improvements.
Conclusions
Improvements will only be effectively carried through if safety and quality improvement are clearly articulated as an organizational strategy. Organizations without senior executive commitment struggled to make effective changes or failed to sustain them. Leadership, managerial and clinical, is critical to success. This realization led to the publication by the NHS Institute of two guides on reducing avoidable deaths in hospital: Medical directors drive improvement 26 and Chief executives lead the way. 27
Local acceptance that a problem exists is essential. Where to start depends on local prioritization following a diagnostic process based on triangulation of sources of information, of which the case-notes review is most powerful. Executive walk-rounds uncover safety issues but also demonstrate leadership commitment to building a safety culture. Incident reports are necessary but not sufficient to highlight errors. 6
Measurement of improved outcomes is important to support such initiatives, both to ensure that the changes really are having a positive impact and to encourage participation. As quality guru WE Deming said: ‘All improvement requires change, but not all change is improvement’. We found that continuous plotting of crude unadjusted weekly deaths as a time series was an effective and timely way of monitoring improvement, later validating this retrospectively with monthly or quarterly HSMR. Statistical process control charts were widely used to display a variety of measures (Box 1).
There is no shortage of knowledge regarding what might work. Having a suite of interventions to try, coupled with the support of service improvement experts enabled organizations to implement effective change. However, there is no single intervention that works alone; rather, multiple interventions create a culture of safety across the organization and encourage vigilance for error in individuals and clinical teams. 28 Clinicians, improvement experts and frontline managers working constructively together gives the best chance of a successful, sustained improvement. 29
Overall it is clear that work on reducing mortality in hospitals can succeed. The difficulty in analysing success is that many changes were introduced, so it is hard to attribute causation to any single intervention, yet overall HSMR was reduced by 10%. Clearly, if such a reduction could be achieved in all hospitals, the impact on mortality would be considerable. Extrapolation from this analysis, even with conservative assumptions about what might be achieved, would suggest that 10,000 lives could be saved per annum in England alone.