
Abstract

The use of antipsychotic drugs in the ‘management’ of dementia remains controversial. It has been largely attributed, naively, to care homes perhaps seeking a quiet life with sedated complicit residents. The reality is much more complex. First, there needs to be a wider public understanding of the needs and behaviours in the context of dementia. It may be that some use of sedation in acute circumstances may be warranted for the safety of the individual and those around them. However, for long-term care, intelligent commissioning, adequately trained, supported and rewarded workforce underpinned by sensitive but accountable regulation may well make behaviours and deficits that were deemed challenging or of unacceptable risk to actually be eminently manageable.
There are now some three care-home beds for every NHS establishment bed (all specialties) in England. Some two-thirds of these beds provide refuge and care for people with mental impairment, usually related to dementia. 1
The well-publicized real and apparent failings of care homes have made them an easy target for recurring public and media vilification with little systematic examination of issues. For many frail older people and their families care homes can and do offer dignified care in the face of often quite desperate adversity.
The use of antipsychotic medication in care homes provides a window to shortcomings regarding the organization and accountability of health and care services. Care homes are principally regulated (at the time of writing, November 2008) by a social care inspectorate that looks at life quality through a lens polarized to social care. With regard to medication, compliance with regulations regarding management of prescription orders, drug storage and administration dominate, the questioning of appropriateness and rationale for prescribed drugs is not a defined regulatory domain though sometimes inspectors do become engaged in such matters. In spite of the ‘social model’ of care, residents are now admitted, overwhelmingly, as a consequence of illness driven disability. 2
Before exploring present antipsychotic medication usage I relate an illustrative vignette of two dementia care units run by a distinguished charity that I observed over 20 years ago but it could have been yesterday or probably tomorrow! Unit A had nothing but praise from relatives, their family members with dementia were all perfectly dressed and coiffured – albeit somewhat sleepily sitting vacantly in a clean and fresh day room. Unit B had a series of complaints about disordered behaviour; generally the unit looked a bit messy and disordered with folk on the go involved in all sorts of activity. Both units had to a degree failed; unit A's residents were extensively medicated by day though apparently at night the place was ‘lively’. Unit B's resident's were largely free of significant medication and nights more peaceful, the senior manager however had failed to communicate adequately with visitors how the unit was run and why its residents' activity by day was actually ‘normal’.
Antipsychotic medication use in care homes could by now have been tackled by regulators, but neither the Healthcare Commission nor its predecessor the Commission for Healthcare Improvement (CHI) have systematically investigated medication use in care homes. The nearest investigation in scope was that undertaken and reported by CHI in 2002 regarding prescribing at the Portsmouth Healthcare NHS Trust at Gosport Memorial Hospital, a subacute facility where clinical practice had significant parallels with those of a typical care home. The executive summary of CHI's report summarized its findings:
3
CHI concludes that a number of factors, detailed in the report, contributed to a failure of trust systems to ensure good quality patient care:
there were insufficient local prescribing guidelines in place governing the prescription of powerful pain relieving and sedative medicines; the lack of a rigorous, routine review of pharmacy data led to high levels of prescribing on wards caring for older people not being questioned; the absence of adequate trust-wide supervision and appraisal systems meant that poor prescribing practice was not identified; there was a lack of thorough multidisciplinary total patient assessment to determine care needs on admission.
Following this publication, the NHS Chief Executive Bulletin drew attention to the report:
4
Commission for Health Improvement Investigation: Portsmouth Healthcare NHS Trust at Gosport War Memorial Hospital: CHI has completed a report of a special investigation into hospital services for elderly patients at a trust in Portsmouth. The report makes important recommendations about care of the elderly and can be found at: [CHI website and full report can be found at reference 3]
It is difficult to identify any systematic NHS response to the recommendations of this report in hospitals let alone a specific initiative with regard to psychotropic use in care homes.
The Commission for Social Care Inspection (CSCI) is the principal regulator for care homes and is charged to ensure that medicine management complies with a set of standards whose purpose is to ensure that medicines prescribed by doctors and dispensed by pharmacists are stored safely and administered in accordance with prescribed instructions and that full records are maintained. CSCI have raised standards of medicine management in care homes through close attention to the processes for which care homes are responsible. Arguably, the regulatory scrutiny by CSCI inspectors has improved compliance such that inappropriately prescribed and dispensed treatment has been administered more consistently rather than significantly reduced! CSCI do not have a responsibility to routinely collate clinical diagnoses or scrutinize the appropriateness of prescribed medications on people resident in care homes as confirmed in their evidence to the All Party Group on Dementia (APPGD). 5
The National Institute for Health and Clinical Excellence (NICE) and the Social Care Institute for Excellence (SCIE) produced an extensive report on dementia. While most reactions focused on this reports' determination regarding the specific treatments for dementia, there was consideration and guidance regarding the place of other treatments and the specific guidance regarding antipsychotics could not have been clearer:
6
Do not use antipsychotic drugs for mild-to-moderate non-cognitive symptoms in:
DLB, because of the risk of severe adverse reactions; Alzheimer's disease, vascular dementia or mixed dementias, because of the increased risk of cerebrovascular adverse events and death. Consider antipsychotics for severe non-cognitive symptoms (psychosis and/or agitated behaviour causing significant distress) only if:
risks and benefits have been fully discussed; assess cerebrovascular risk factors and discuss possible increased risk of stroke/transient ischaemic attack and possible adverse effects on cognition; changes in cognition are regularly assessed and recorded – consider alternative medication if necessary; target symptoms have been identified, quantified and documented, and changes are regularly assessed and recorded; co-morbid conditions, such as depression, have been considered; the drug is chosen after an individual risk–benefit analysis; the dose is started low and titrated upwards; treatment is time-limited and regularly reviewed (every 3 months or according to clinical need). In DLB, monitor for severe untoward reactions, particularly neuroleptic sensitivity reactions (development or worsening of extrapyramidal features or acute, severe physical deterioration).
Much of the information regarding antipsychotic drug prescribing for people with dementia in care homes has rested on small number studies and anecdote, for example the recent APPGD report 5 cites prescribing rates based on a study of 331 care-home residents. As electronic prescribing becomes more prevalent such information should be comprehensive and readily available making practice more transparent. Some innovative pharmacies are sufficiently advanced to be able to supply such data. Here I report anonymized information obtained from a specialist pharmacy relating to its dispensing of prescribed antipsychotic drugs to 5090 patients resident in 145 care homes (personal communication). This data-set reports that the average number of prescribed items per patient was 7.5 and overall 881 (17.3%) residents were prescribed antipsychotic drugs. Figure 1 demonstrates the distribution of antipsychotic prescription in care homes. These represent a range of registration types of homes; however it is striking the number of homes with high proportions of residents on antipsychotic agents.
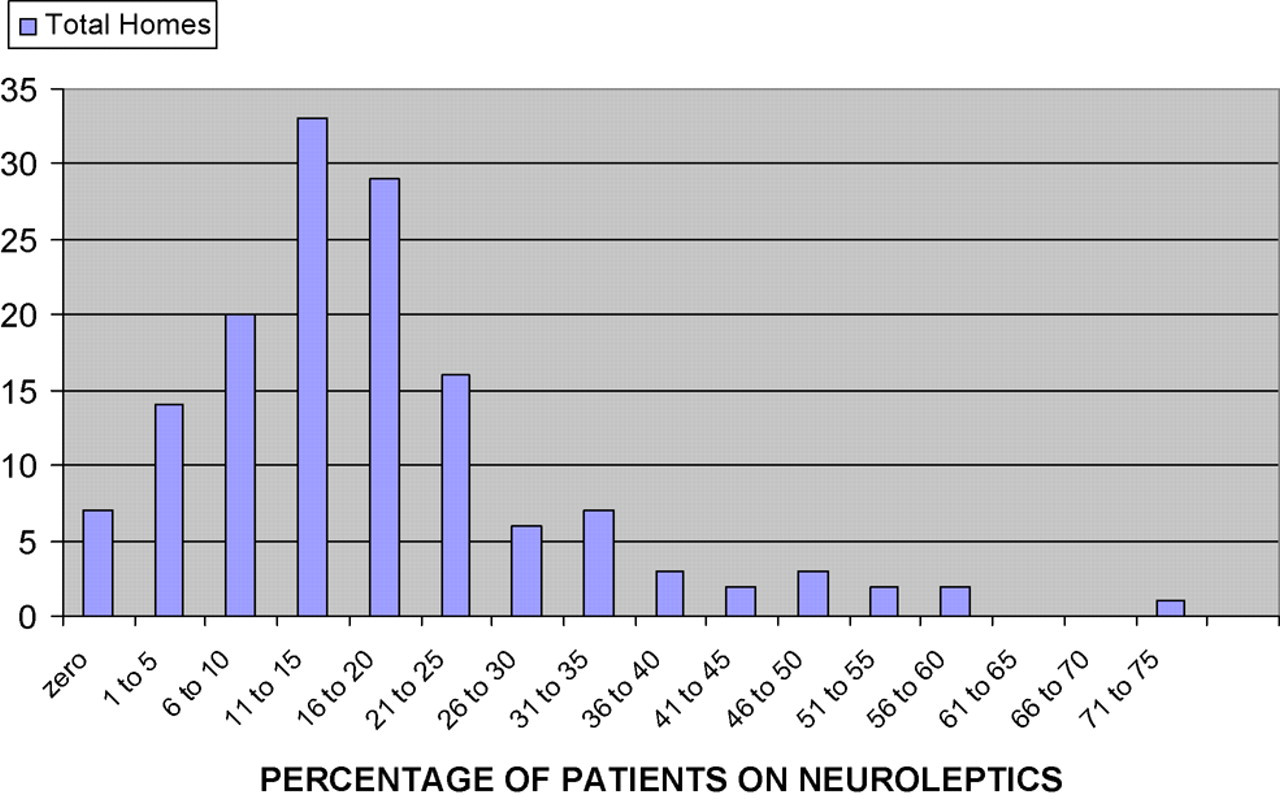
The distribution of the percentage of patients on neuroleptic drugs in the 145 care homes. The average percentage of patients on neuroleptic drugs in a care home lies between 11% and 15%
Cutting this data-set by Primary Care Trust (PCT) raises questions of prescribing patterns, Table 1 shows considerable variation both in the overall prescribing of antipsychotic drugs and also the variation in ratio of newer ‘atypical’ agents and older ‘typical’ agents. Concern regarding increased mortality relating to newer ‘atypical’ antipsychotics has led to recommendations that they be avoided, however their continued prevalence may reflect prescribers' anxieties regarding the greater propensity of known extra-pyramidial drug-related side-effects associated with older ‘typical’ agents.
The usage of neuroleptics within each PCT (and the split between the newer and older drugs)
Atypical neuro = total number of new neuropleptics (olanzapine, risperidone) in the ‘Total drug’ category; Typical neuro = total number of old neuroleptics (quetiepine, haloperidol, flupenthixol, sulpiride, amisulpiride, chloropromazine, trifluroperazine, promazine) in the ‘Total drug’ category
Note: This data is blind to individual diagnosis and home registration status and case-mix. It is possible in the PCTs with smaller numbers the data may be unrepresentative and that in other PCTs alternative supplying pharmacies may introduce various inconsistencies that undermine the robustness of the data. However these quibbles are unlikely to justify that across 13 PCTs an observed three-fold variation in the rate of the prescribing of neuroleptics is warranted
The question of who is responsible for initiating antipsychotic agents and where and how that occurs is crucial. Table 2 reports that 46% of antipsychotic prescriptions were initiated after admission.
Neuroleptic drugs were started after admission?
*30 days after admission
Note: While this information is available within the database, it is not entirely reliable. Date of Admission is held along with the Start Date of the drug. However the limitation is that often the care home do not provide an accurate date of admission or omit this entirely. Also, in the case of new homes using this pharmacy the date of admission is taken to be the date the home joined our service. Nonetheless it is likely to be highly indicative
It is worth reflecting why so many people are being commenced on antipsychotic medication before entering a care home. For those being cared for by their family in the community at large it may represent a desperate attempt to extend a family's capacity to cope, while in hospital settings where people with dementia are often admitted following a crisis such as a fall or intercurrent illness it may be a pragmatic solution to the distress of the individual and the risk of disturbance and harm to themselves and those around them. Transfer from hospital to a care home continues to be blighted by inadequate information especially for receiving general practitioners who typically are not the patient's usual or previous doctor and are, unsurprisingly, reluctant to actively initiate a programme of drug reduction without adequate information (an individual's full record asset may take a considerable time to ‘catch up’ with their current doctor). The evidence base for antipsychotic medication in the treatment of dementia in care homes is generally lacking but the experience that doctors have of treating behavioural problems is rooted in their hospital training. Noble practitioners opting to seek higher levels of care to meet an individual's changing needs seldom find responsive commissioners; generally the imperative something must be done immediately means that more often than not a sedative prescription is offered.
Finally, the database was searched to determine patients who are on Alzheimer's treatment and also receiving antipsychotic drugs. The results (Figure 2) reveal three homes with more than 10 patients concurrently receiving medication for Alzheimer's disease antipsychotic drugs. It is considered inappropriate that patients diagnosed and treated with ‘antidementia medication’ be concurrently treated for aggression with antipsychotic drugs, and that in such cases the antidementia drug prescription should be critically reviewed.

Incidence of ‘dementia treatment’ being accompanied by antipsychotic drugs
Collectively this data seriously questions whether NICE guidance is being observed, and while blame has consistently been targeted at care homes themselves there clearly is a failure in following guidelines reflected in the overall prevalence and variation of antipsychotic prescribing.
How will progress occur, carrot or stick? Regrettably, the NICE/SCIE report has had little impact regarding day-to-day prescribing behaviour of antipsychotic treatment but it does provide standards by which, governance and professional behaviour could be challenged, for example potentially the GMC could assess professional practice. This may seem draconian but there can be little doubt that following the Shipman case prescribing approaches to controlled drugs for older people have become more cautious.
There has been a move for greater numbers of people with dementia being placed in ‘specialist residential dementia care’ rather than the nursing-led care of a nursing home. While the role and value of professional nurse leadership has some uncertainty in dementia care there are situations, for example when an individual exhibits a sudden change in behaviour, when clinical expertise can be important in determining the need for action. It is probably unreasonable to expect non-clinically trained care staff to be expert on the determination and causation of delirium or to have a sophisticated awareness of the adverse effects of various medications. Clearly, there are clinical risks in residential dementia care that can only be effectively addressed by health professionals and if these are not commissioned the risks are, simply, not being addressed.
More positively, a simple Quality Outcome Framework (QOF) addressing prescribing practice of care-home residents could be incentivized to reduce prescribing of antipsychotics progressively from 15% to 10% and then to 5% of the care-home population. Certainly there are sound anecdotal examples of dementia care where well-led care homes with pro-active and supportive primary care have achieved below a 5% rate of prescribing.
In isolation both these approaches are probably inadequate in the face of inadequate commissioning and care standards. Care homes can become overwhelmed by the challenge of people with dementia, individually or collectively and it has to be acknowledged that some of these homes will be lacking skills, leadership, or commitment. However even well-organized and equipped homes can fail through the collective burden of dependency exceeding the capacity to care and it is here that a commissioning responsibility needs to be recognized.
The assessment of the needs of people with dementia is often simplified and can be misleading. For example, asking whether an individual can shave may result in a positive response and so in terms of self-care a need is not recognized. It may only take 10 minutes to shave someone but for someone with dementia to be ‘set up’ to understand that it would be a good time to shave and to concentrate on shaving safely may take much longer and yet not be factored into care! Assessments continue to feature curious judgments, ‘pleasantly confused’, seldom being helpful!
The advent of the new regulator, the Commission for Care Quality (CQC) integrating the responsibilities of the Healthcare Commission and CSCI could achieve that which endless reports and outrage have failed to do through seeking information on prescribing rates of antipsychotics of people resident in care homes and investigating outliers. This approach would bring a focus to the boardrooms of PCTs and Local Authorities.
The increasing visibility of practice variation through automatically generated data-sets such as that used in this article have the power to increasingly challenge practitioners and impose greater accountability for divergence from best practice guidance. Whether responsibility for patterns of antipsychotic use in care will be seen as a failure of PCTs to establish effective surveillance and controls or as an individual professional liability remains unclear. Positive action now would probably reduce the risk of individuals or PCTs being part of a sentinel investigation that finally brings discipline and control to antipsychotic prescription in care homes generally and in dementia specifically.
Footnotes
Acknowledgement
I thank Pharmacy Plus for making available the data in this paper and acknowledge their professionalism.