
Abstract

Introduction
Interventional radiology (IR) is the use of imaging guidance to effect treatment. The discipline evolved from invasive diagnostic techniques such as angiography, performed by radiologists to diagnose structural cardiovascular diseases. It developed after Charles Dotter an American radiologist performed the first angioplasty on a woman due for bypass surgery the following day.
During the last two decades, IR has grown as more young radiologists have trained in the USA and Europe, their skills have improved and the possibilities unleashed by emerging technologies have suggested unlimited horizons. IR procedures are replacing traditional surgical techniques bringing many benefits to patients and to the health service. IR techniques can usually be performed on an outpatient basis or with an overnight stay in hospital, resulting in substantial financial savings. They are almost always safer than the equivalent surgical methods and allow much faster recovery, enabling patients to return to normal activities more quickly.
Examples of the contribution of IR to modern patient care include the following:
Arterial embolization for the treatment of haemorrhage, e.g. in major trauma, gastrointestinal haemorrhage, bronchial haemorrhage and postpartum haemorrhage. Surgery in such situations carries substantial risks. In addition, it may result in avoidable adjunctive procedures, such as hysterectomy, which may affect profoundly the patient's life; Embolization is also frequently used to deal with iatrogenic haemorrhage, e.g. following renal or liver biopsy. In the past, severe haemorrhage following such procedures necessitated major surgery to save the patient's life; Embolization of intracerebral aneurysms has almost replaced craniotomy and aneurysm clipping; A substantial proportion of patients with malignant obstructive jaundice cannot be treated with endoscopy or surgery and require percutaneous intervention, usually involving the insertion of metallic stents. Benign postoperative biliary strictures can be treated by balloon dilatation, obviating the need for major surgery; Narrowed or obstructed arteries in many organs can be treated with balloon angioplasty, which may be followed by the insertion of metallic stents. Examples include stenosis of arteries to the viscera causing kidney failure or bowel ischemia, and carotid artery stenosis causing transient ischaemic attacks; Ureteric strictures can be treated with balloon angioplasty. Malignant ureteric obstruction can be stented; Tumours in the kidney, liver, lung and other organs are increasingly treated with percutaneous thermal ablation or cryotherapy. These procedures can obviate the need for nephrectomy partial hepatic resection or pneumonectomy; Partially collapsed vertebrae or other bones in patients with osteoporosis or skeletal metastases can be palliated with cementoplasty enabling rapid return to normal activities; Aortic stent grafts, often performed in partnership with vascular surgeons, are fast replacing conventional surgery for aortic aneurysms and aortic dissection.
The above are only selected examples of the contribution of IR (Figure 1). There are many other areas of IR activity, which involve almost every organ system and the evidence base for most is strong and evolving through randomized trials like EVAR, BASIL, ASTRAL, MIMIC, REST, EMMY, HOPEFUL
1–8
and many others.
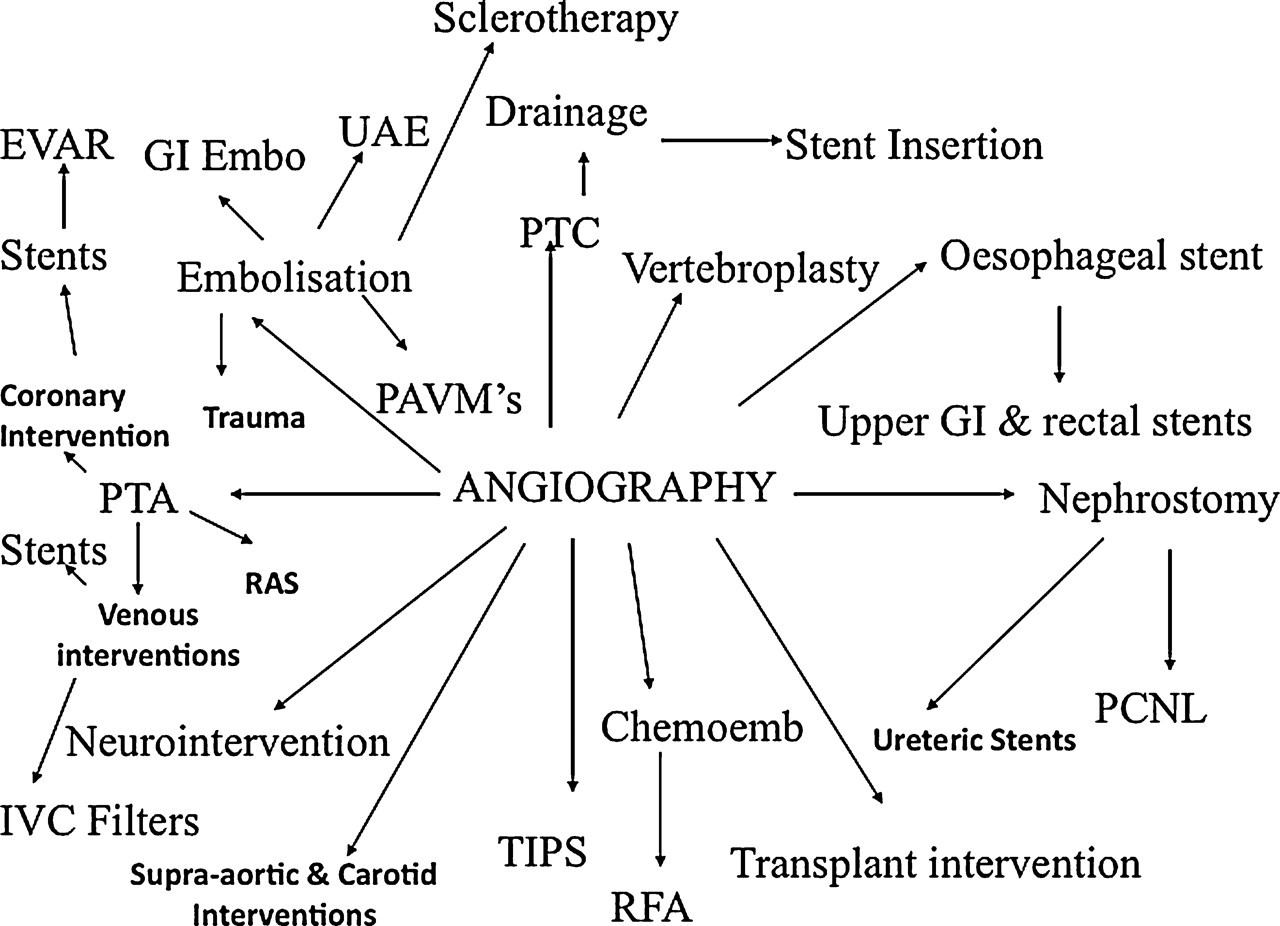
The range of therapeutic procedures in everyday use that have evolved from the diagnostic angiogram since 1964. EVAR = endovascular aneurysm repair; TIPS = transjugular portosystemic shunt for liver disease; GI Embo = gastrointestinal bleeding embolization; PAVM = pulmonary arteriovenous malformation embolization; RFA = radio frequency ablation of small cancers; PTA = percutaneous transluminal angioplasty; UAE = uterine artery embolization for fibroids; PCNL = percutaneous nephrolithotomy for kidney stones; IVC filter = inferior vena cava filter for preventing pulmonary embolism; Chemoemb = chemoembolization of liver cancer
The current situation
The availability of IR in UK hospitals is limited. Few hospitals offer a comprehensive IR service. In-hours, many patients with common conditions cannot access minimally-invasive IR procedures that would palliate or cure conditions which otherwise require major surgery and/or analgesics. For example, many patients with osteoporotic vertebral fractures, causing immense pain, who would benefit from IR procedures such as vertebroplasty do not have access to interventional radiology. In theory, they could be referred to another centre but the patchy and erratic availability of the relevant services, with no direct method of referral, makes this process difficult. In some areas of IR, particularly in the vascular field, it is relatively easy to gain access to the relevant service for some procedures such as angioplasty. In other areas, it is very difficult, as many procedures are carried out in a small number of centres, by practitioners who may not have outpatient clinics or the supporting infrastructure for receiving referrals. In such cases, the referrer may need to telephone the relevant interventional radiologist to find out how the referral can be made. Unsurprisingly, many potential referrals are never made, the referrer deciding to take the easier route of sending the patient to a surgeon for a more conventional procedure locally. In this and other respects NHS systems are, unwittingly, inherently biased against IR.
The availability of IR out-of-hours is even poorer than the situation described above. A recent survey by the Royal College of Radiologists suggested that only 15 out of 100 NHS acute trusts provide a comprehensive formal on-call IR rota and that six of these were in London. Of the rest, only two have formal arrangements for transfer to a trust that can provide service. The latter increases the already onerous on-call burden in those few hospitals providing service and, as there are rarely any financial arrangements, such patients are considered to be high-cost low-income drains on already over-stretched budgets.
This situation is unsatisfactory and places patients at risk and has been highlighted in several reports by governmental and non-governmental bodies. 9–13 There are many emergency conditions in which IR can make a major contribution, including postpartum haemorrhage, gastrointestinal bleeding, acute colonic obstruction, subarachnoid haemorrhage, intra-abdominal abscess, obstruction of the urinary tract, rupture or dissection of the thoracic aorta, leaking aortic aneurysm, renal haemorrhage and peripheral vascular occlusion. In some cases there is an acceptable surgical or endoscopic alternative treatment. In other cases, alternative treatments are not available or are associated with a significantly higher morbidity or mortality. For instance, the Advanced Trauma Life Support guidelines, used for trauma victims in the UK and all over the world recommend angiography and embolization for life-threatening haemorrhage and stent grafting for tears in the aorta. 14 There are only 15 centres in the whole of the UK where this is available round the clock. There are 175 acute hospital trusts in the NHS where a trauma victim could be taken. If IR were a discipline within surgery, this unacceptable situation would have been addressed long ago. However, the historical development of IR within the specialty of radiology, which has no direct responsibility for patients and lacks the necessary infrastructure, has allowed the persistence of arrangements that place patients at risk on a daily basis.
The reasons for the patchy availability of IR
There are three main reasons for the lack of availability of satisfactory IR services in most hospitals.
Lack of designated IR posts
In 2007–2008 there were just 13 IR consultant posts advertised in the careers section of the British Medical Journal. As seven of these were re-advertisements for unfilled posts it is likely that there were just six posts out of a total of 370 radiology consultant adverts. This is because most posts advertised in radiology are for radiologists with an interest and there is no onus on departments or hospital trusts or instruction from the Strategic Health Authorities to provide in or out-of-hours specialist IR. There is however an onus to provide a diagnostic imaging service.
Therefore the breadth of training and skills are not available in most hospitals to provide comprehensive in-hours service and the number of interventional radiologists in any one department is usually too small for an acceptably low frequency of on-call duty especially when the out-of-hours demands are so onerous.
The lack of designated IR posts produces a viscous cycle. With no clear career structure or job opportunity many potential IRs do not pursue their original career plans.
An insufficient number of IRs
A substantial proportion of applicants for trainee posts in radiology profess an interest in IR. However, during their training period, the majority become more interested in diagnostic aspects of the specialty and very few apply for posts with an interest in IR. Surveys 15 have suggested that the lack of a clear career structure or any jobs in IR is an obvious disincentive for entering this discipline. Frequent onerous on-call is not an attractive lifestyle. This partly results from the lack of numbers of dedicated IR posts as above in a ‘chicken and egg’ conundrum. In addition, junior radiologists cite the lack of direct access to patients and the resultant ‘filtering’ of referrals by clinicians, reducing the opportunities for private practice, as further diminishing the attractiveness of IR. Training opportunities, despite a robust training curriculum in IR are limited as there are so few jobs.
The financial arrangements for IR
Radiology department budgets are over-stretched. There is a heavy workload of diagnostic work provided by expensive items of capital equipment that require regular renewal. Diagnostic radiology is labour intensive and the staffing requirements of radiology departments huge. Interventional radiology is a relative ‘new kid on the block’ and has a similar requirement for expensive capital equipment and staff but in addition uses large quantities of expensive disposable items and implants. While diagnostic services have to be provided, there is no requirement to provide anything other than the most basic interventional procedures in-hours. Consequently many treatments are not offered and others are so badly funded that not all the equipment to provide safe practice is available. An example would be the absence of expensive stent grafts as stock items, which is vital to treat the complication of a ruptured artery during angioplasty and was highlighted by an NCEPOD report.
Correctly funded Service Level Agreements are not in the interest of trust finance departments as there is no real mechanism for transferring budgets from one specialty to another. Where they exist they are based on a small fee per Korner Unit and generally have a maximum (and grossly inadequate) recharge of £90.
All this is compounded by the high-cost low-income penalties for treating patients from other trusts as the funding stream for interventional work does not come back to the radiology department. There are three reasons for this: one is an absence of appropriate coding, a second is an absence of any formal contract to provide service and a third is the diversion of any funding to the bed-holder.
Possible solution
The creation of posts in IR, occupied by individuals committed to a career in this discipline would seem an obvious solution. Eventually, these posts should be occupied by specialist registrars (SpRs) undertaking dedicated subspecialty training in IR, which should include formal instruction in procedures and equipment as well as clinical training. The Royal College of Radiologists is exploring ways of addressing this issue. The creation of designated posts in IR can be effected immediately. If such posts were created, more SpRs would train in this subject and the number of Fellowships in IR would increase.
Designated IR posts need to be distinct for those in radiology departments, necessitating the setting-up of separate units of IR, with access to short-stay beds. The job plans of interventional radiologists should formally include ward rounds and outpatient clinics. IR units should have clear and distinct lines of funding, enabling the hospital to enter into contracts with Primary Care Trusts for the provision of interventional radiological services. This would remove the current disincentives for the provision of IR services by radiology departments and would encourage appropriate pre-and post-procedure care.
The creation of designated IR posts would also enable manpower planning. The number of ‘interventional radiologists’ in the UK is currently unknown because there is no clear definition of the term. An interventional radiologist may be a person carrying out a few straightforward procedures on an occasional basis or complex interventions every day. IR should be treated as a ‘small specialty’, in which staffing should be determined by the on-call requirement. Approximately six interventional radiologists should be appointed in most large hospitals. Of course, they would undertake some diagnostic imaging in areas relevant to their interventional work. They should be supported by appropriately trained nurses and radiographers; this is a related issue, with patient safety implications of its own. It is often thought that the routine workload in IR would not justify these appointments but this is an illusion: experience has shown repeatedly that the demand for routine IR services is (inadvertently) kept down simply by not offering them. Where they have been offered, the demand has increased substantially. The greater clinical involvement would also contribute towards job planning. In addition, there are specialties like neurosurgery and vascular surgery where the numbers are based on the emergency rather than the elective requirement.
A ‘hub and spoke’ approach should be used, enabling those in designated IR posts in large hospitals to work together with colleagues in smaller units to provide a comprehensive IR service.
Once a clearer career pathway is created then training will have to adapt to meet the requirements. In anticipation of this the Royal College of Radiologists has instructed its Specialist Advisory Committee to develop a new curriculum from the existing updated syllabus. Training in IR should be reformed to ensure that those undertaking IR work receive formal instruction in the clinical IR as well as procedures and techniques. This is an essential requirement for patient safety. The very different training requirements for IR compared to diagnostic radiology may require in the future an approach to PMETB for subspecialty status but that would be evolutionary rather than revolutionary.
Summary
Interventional radiology is now a mainstream discipline, making an important contribution to the health service. However, inadequate arrangements in relation to its structure and funding are preventing its further development and result in poor provision of service and unsatisfactory arrangements, which can endanger patients. The best way to address this issue is to create designated posts in IR, funded separately from posts in radiology departments. These posts should operate side-by-side with posts in radiology the occupants of which undertake limited IR work. The job plans of such posts should include ward rounds and outpatient clinics. All this will require radical changes to the existing curriculum. The funding structure should be separate from the budgets of departments of radiology, to allow direct contracting for IR services. Subspecialty status for IR is very firmly on the agenda but until the requirements above are met this cannot be achieved.