
Abstract

Introduction
The effects of medical errors on patients' morbidity and mortality have been highlighted both in the United States and United Kingdom. 1,2 Studies have shown that some 10% of patients admitted to hospital experience an adverse event and when multiple adverse events are included, this figure rises to 11.8%. About half of these are judged preventable. 3 Medication errors alone account for between 10–20% of adverse events in patients admitted to hospital. 1,4
A number of studies have demonstrated that the majority of medical errors go unreported. Healthcare professionals, particularly doctors, have been shown to be reluctant to report adverse events although nurses are significantly more likely to report their own medical errors than doctors. 5–8
Over the last decade the development of clinical risk management in the UK has led to the establishment of local incident reporting systems in hospitals. It was hoped that the incident reporting system would provide a valuable insight into local problems and, in an ideal situation, be used to identify regional and national patterns of failure.
In the UK, the National Patient Safety Agency (NPSA) has been set up as a body for the collection of errors so that lessons, both at a national and local level, can be appreciated more easily. The NPSA defines a patient safety incident as any unintended or unexpected incident(s) that could have or did lead to harm to one or more persons receiving NHS-funded healthcare. 9 Although no firm figures exist, a number of studies have reported that as many as 10% of all patients admitted to hospitals experience an adverse event. 3
To date no study has assessed the incidence of medical errors in an emergency department. The Emergency Department at Mayday University Hospital adopted a comprehensive clinical governance programme in 2004 including monthly staff meetings aiming to disseminate information, including the importance of incident reporting, to all members of staff.
This study was carried out to assess the incident reporting process since the introduction of a clinical governance programme in 2004.
Method
A 12-month retrospective review of all completed patient safety incident forms in our department from 1 September 2006 until 31 August 2007 was carried out. The forms (IRIS) were not anonymized and were hand written with a carbon copy retained within the main folder.
With each form, data were extracted including the type of incident, where and when it occurred, the impact of the incident on the patient, details of who completed the form and whether or not the patient (or their next of kin) was informed of the incident. All extracted data were anonymized.
The NPSA uses a classification system for all patient safety incidents. We applied this same classification system to all of our reported incidents.
The collected data were analysed to see if the incident resulted in any harm to the patient, and if so whether the level of harm was low, moderate or severe, if it resulted directly in a patient's death and whether patients or relatives were informed of the error. The total number but not the breakdown of incident forms for the previous two years was also obtained.
Results
In the 12-month period a total of 112,957 patients attended our emergency department. In the same period, 179 incident reports were completed (0.16%). The number of completed incident reports for the previous 12 months was 164 and for the 12 months prior to that 189.
Of these 179 reports, only 115 (64%) actually fell within the NPSA definition of a patient safety incident. This amounted to just over 0.1% of all attendances. Only nine incident forms indicated that the patient or their relative had been informed of the incident.
Of the 64 incident reports not related to patients, 17 were reports of needle stick injuries sustained by staff and 28 were reports of verbal and physical abuse towards staff by non-patients (e.g. friends and relatives of patients). A further six reports were of injuries sustained by staff at work, not involving patients. The rest were due to a variety of incidents ranging from staff self-prescribing medications through to an electrical fault with the staff vending machine.
Of the 115 reports that could be classified as a patient safety incident, 102 (88.7%) were reported by nursing staff and 13 (11.3%) by clinicians. Eleven were reported by middle grades, one by a SHO and one report was completed by a consultant.
Four events were linked to the death of the patient. These were all reported by clinicians and included misinterpretation of ECGs in two patients and two biochemistry results. The remaining 111 incidents were due to a number of different reasons. These are shown in Figure 1. Of those that resulted in harm to the patient, none were deemed to have resulted in severe harm. In addition to the four events linked to patients' deaths, a further three, all missed fractures, were deemed to have resulted in moderate harm, and the remainder resulted in low harm or no harm. This group included delay in treatment or transfer, missing notes and missed fractures.
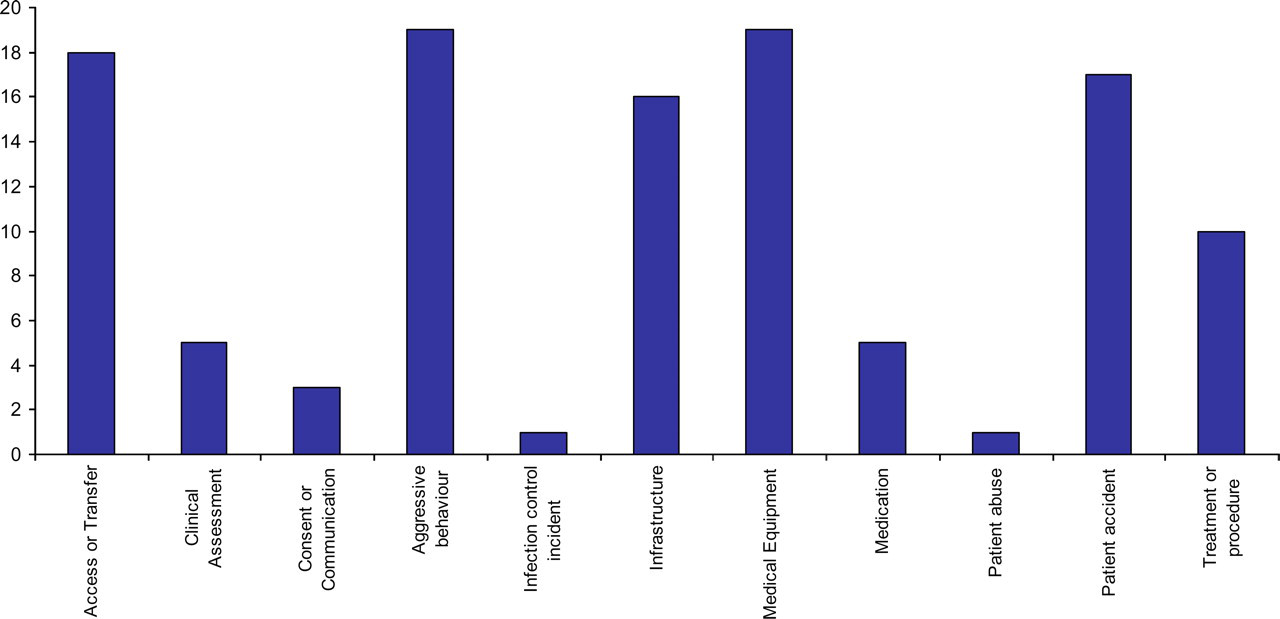
Classification of all reported patient safety incidents
There were 17 reported patient accidents, 19 reports of patient aggression and 19 episodes of medical equipment failure. Only five (4%) involved errors in medication. Sixteen incidents involved hospitals' infrastructure problems (e.g. staffing issues, lack of hospital beds, etc.).
Discussion
To date no study has accurately assessed the incidence of medical errors in an emergency department. Tighe et al. 10 found 174 reported incidents over a 13-month period at a busy emergency department of a London teaching hospital, a reporting rate similar to our own. We see no reason as to why medical errors should be less frequent in emergency departments and it is possible that a recent paper from Thomas and Mackway-Jones 11 may underestimate the size of this problem even though it reflects a higher rate of incident reporting as compared to our study.
Our survey supports the finding by others that healthcare professionals, especially doctors are reluctant to report adverse events. Adverse events however are a serious problem in the NHS. The estimated cost in extra bed-days alone in the UK is thought to be around £1 billion a year. 3
Although there is still a need for further research into better understanding of why a certain group of healthcare workers do not contribute to the reporting system, ‘incident reporting’ should become an integral part of induction programme for nurses and in particular doctors. The programme should address specifically the type of incidents to be reported and the procedures to submit them.
Incident report forms should also be made more accessible, better designed and user-friendly for reporting of incidents. The mechanism needed to report errors should be easily accessible and require only a small amount of time; electronic formats are preferable and, as this is about to be introduced in our hospital, it would be interesting to see if this measure which also provides for a degree of anonymity will improve incident reporting specially by doctors. Any system in operation should also make sure that healthcare professionals receive regular feedback both of the type and frequencies of errors that are reported, along with information about specific examples of system changes being made in response to the identified sources of medical errors.
Senior clinicians can set an example by reporting errors and near-misses which may help towards changing the culture around incident reporting helping the process to become an essential element in the provision of optimal patient care.