
Abstract

Safety is a relative word, especially in medicine where the risks of any therapy must be balanced against the perceived potential of benefit for the individual patient. Diagnostic imaging tests are no different to any other medical endeavour in this respect with even chest radiographs carrying with them a small but quantifiable risk from the application of X-ray ionizing radiation. Modern cross-sectional imaging makes extensive use of intravascular injections of contrast yet these have been so safe as to not generally require written patient informed consent prior to their use. The potential side-effects of iodine contrast media as used almost throughout the history of radiology have been extensively studied and modern formulations have a low incidence of both minor and major reactions in terms of severity. These reactions are classified as either of unpredictable idiosyncratic type (e.g. anaphylactoid) or predictable non-idiosyncratic reactions. These predictable reactions have been the most extensively studied, specifically the problems of contrast-induced nephrotoxicity (CIN) which appear to have some relation to contrast medium formulation but more especially to patient features, with pre-existing renal impairment (particularly diabetic nephropathy) and dehydration being especially important though other factors such as increasing age, heart failure and concomitant administration of nephrotoxic drugs have a bearing. These risks are greater when factors are combined and the degree of pre-existing renal impairment has a particular relevance with the incidence of CIN increasing dramatically as a function of pre-existing renal dysfunction.
Gadolinium-based contrast agents
Gadolinium-based contrast agents (GBCA) are chelates designed to bind the potentially toxic gadolinium cation in a stable compound that can be injected intravascularly without toxicity for human magnetic resonance imaging (MRI). Why use gadolinium? While this rare earth metal is toxic in its native state, it is highly paramagnetic with seven unpaired electrons and hence produces marked effects on MR images where only small amounts create readily detectable changes in magnetic field that can be easily imaged. The use of a chelate binds the gadolinium in a stable form with low toxicity and these agents generally have similar pharmacokinetics being predominantly excreted unchanged in the urine by glomerular filtration. The exceptions are gadobenate dimelumine (Multihance), gadofosveset trisodium (Vasovist) and gadoxetic acid disodium (Primovist/Eovist) which also undergo approximately 4%, 9% and 50% hepatobiliary excretion, respectively, the latter agent being exclusively used for liver imaging. As with the iodine-based contrast media then gadolinium-based agents may cause similar idiosyncratic and non-idiosyncratic adverse reactions, again classed as either minor or major. Until recently gadolinium contrast agents have been regarded as extremely safe since the rate of adverse reactions recorded in post-marketing surveillance have been even lower than for iodinated contrast media. For example, the rate of fatal, unpredictable idiosyncratic anaphylactic reactions is estimated at approximately 1:100,000 administrations compared to 1:40,000 for iodinated contrast media. Minor reactions are also few and far between although instances of vomiting after injection can obviously be troublesome when they occur in the limited confines of a MRI scanner.
What is the purpose of GBCAs? In the early days of MRI the exquisite soft tissue contrasts achievable compared to CT and other modalities led some to believe that exogenously administered contrast would not be required. However, following the development of GBCAs with research and clinical deployment their clinical usefulness has become obvious. For example, in neurological imaging of the central nervous system including the spine, the ability to enhance lesions where there has been a breakdown in the integrity of the blood-brain barrier (e.g. in areas of inflammation or in neoplasia) has made them invaluable. This was the first area in which GBCAs were used and the first agent became commercially available in 1988. Similarly, the administration of GBCAs in other body regions has been shown to help depict neovascularity (e.g. breast cancer imaging and rheumatological disease). GBCAs are also used to assess organ perfusion such as myocardial perfusion in ischaemic heart disease, brain perfusion in acute stroke and prostate perfusion in evaluation of suspected prostate cancer. GBCAs can also help in the evaluation of organ damage such as determination of myocardial viability/scar and evaluate tumour perfusion response to chemotherapy. All these applications have importantly aided diagnosis in many conditions and body systems and helped contribute to the rise of MRI as a clinically indispensable tool in modern medicine during the 1990s and into this century. Indeed the added value that these agents bring has led to their use becoming the ‘standard of care’ for a variety of MRI studies and in some surveys up to approximately 45% of MRI examinations involve the use of GBCAs (Figures 1 and 2).

Sagittal T1w image of the lumbar spine pre (A) and post (B) gadolinium contrast enhancement in a patient with infective discitis and osteomyelitis at L 4/5. The extent of bony involvement is only really appreciated on the enhanced image
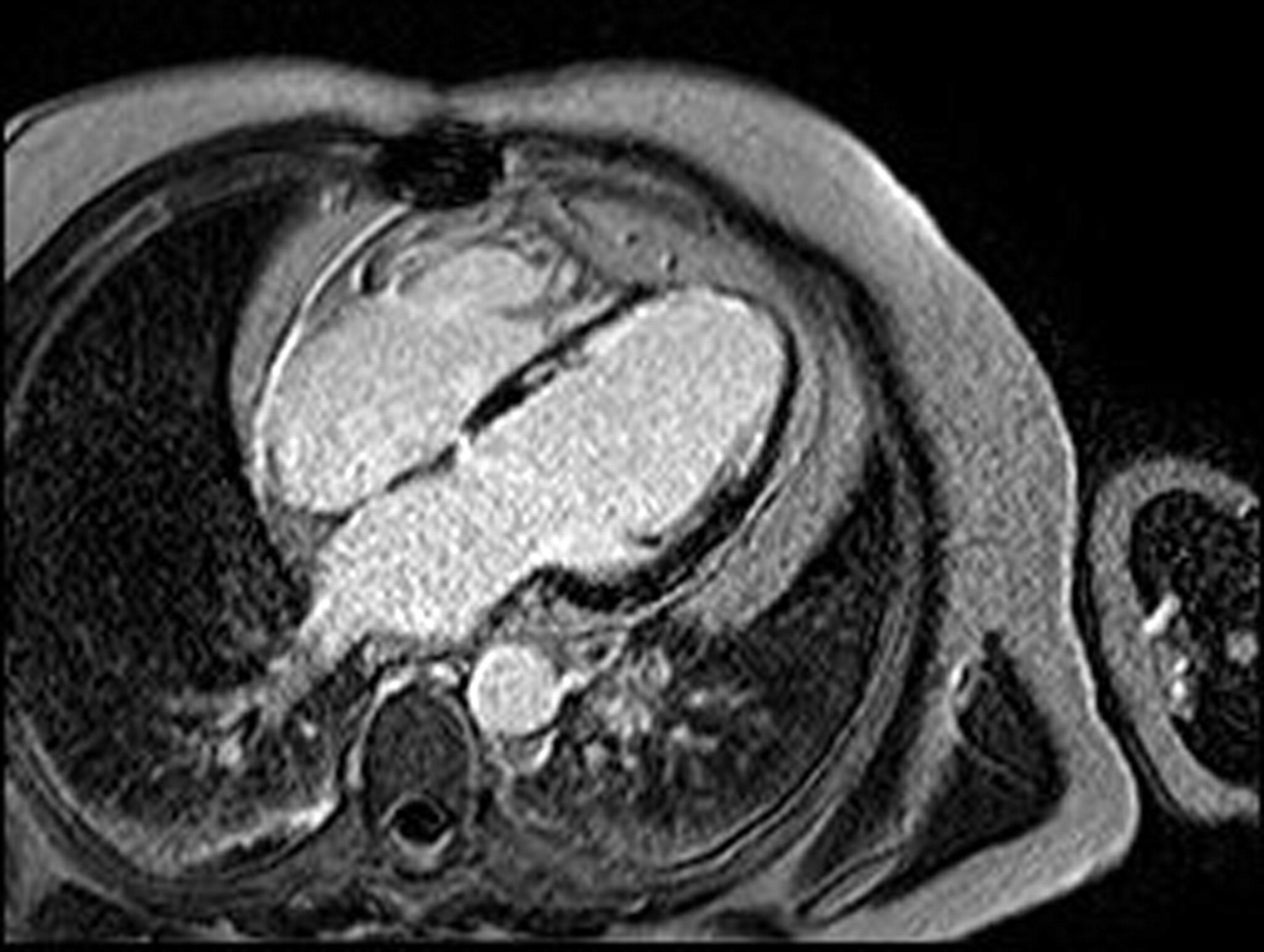
4 Chamber orientation late gadolinium enhancement image of the heart in a patient with ischaemic heart disease and developing left ventricular aneurysm, normal myocardium is dark while bright enhanced scar shows up clearly with subendocardial damage appreciated extending up septum and LV lateral wall
In vascular imaging the early non-contrast enhanced magnetic resonance angiography (MRA) techniques were often hampered (particularly in body imaging) by long acquisition times and artifacts. In this respect the advent of contrast enhanced MRA (CE-MRA) was a real advance as CE-MRA allows repeatable and dynamic non-invasive assessment of the vasculature on an outpatient basis without the need for exposure to ionizing radiation and with contrast agents that are less nephrotoxic in the doses required than conventional iodine-based media. This despite the fact that for successful CE-MRA examinations then relatively increased contrast doses have been required to provide optimum vascular visualization though not to the amounts of iodine-based media needed for CT or conventional angiography. This requirement for relatively increased doses in CE-MRA has recently been reduced by the advances in MRI hardware (such as dedicated array coils) and software (parallel imaging, time resolved/echo sharing, etc.) that have been developed for vascular applications. In patients with renal disease, contrast enhanced examinations have been quite widely used as part of the investigation of the cause of renal impairment, especially in evaluating for potentially correctable renal arterial disease. In patients with more established renal failure, the diagnosis of the vascular complications of renal disease (such as lower limb ischaemia) is important and furthermore contrast enhanced MR venography (MRV) techniques have proven extremely useful for the assessment of the venous stenoses and thromboses occurring as complications of central venous access for haemodialysis. Indeed, CE-MRV provided exquisite detail of venous disease in these patients in a way difficult to achieve by more conventional means (Figures 3–6).

Normal renal function imaging of renal vasculature, (A) hypertensive patient with intimal fibroplasia tight right renal artery stenosis and (B) normotensive volunteer for potential renal donation shown to have bilateral fibromuscular hyperplasia
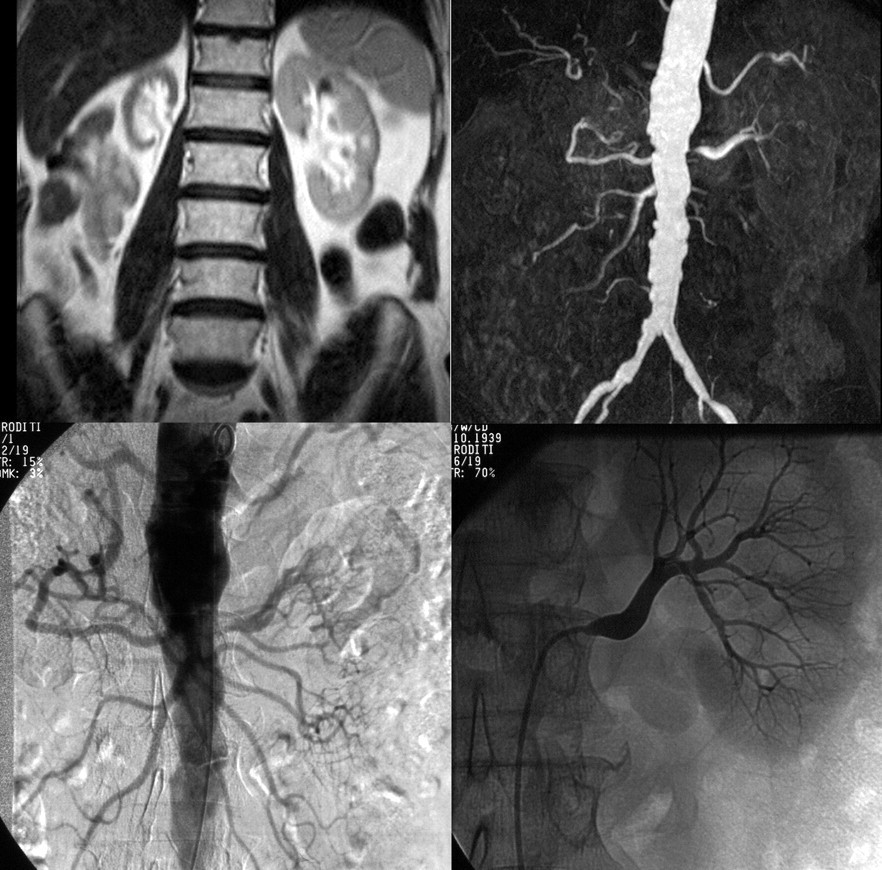
Patient with hypertension and impaired renal function – MRI imaging (upper row) showing atrophic right kidney due to renal artery occlusion and normal size left kidney supplied by tightly stenosed artery. Conventional angiography (bottom row) flush aortic and selective injections at time of revascularization confirm MRI findings
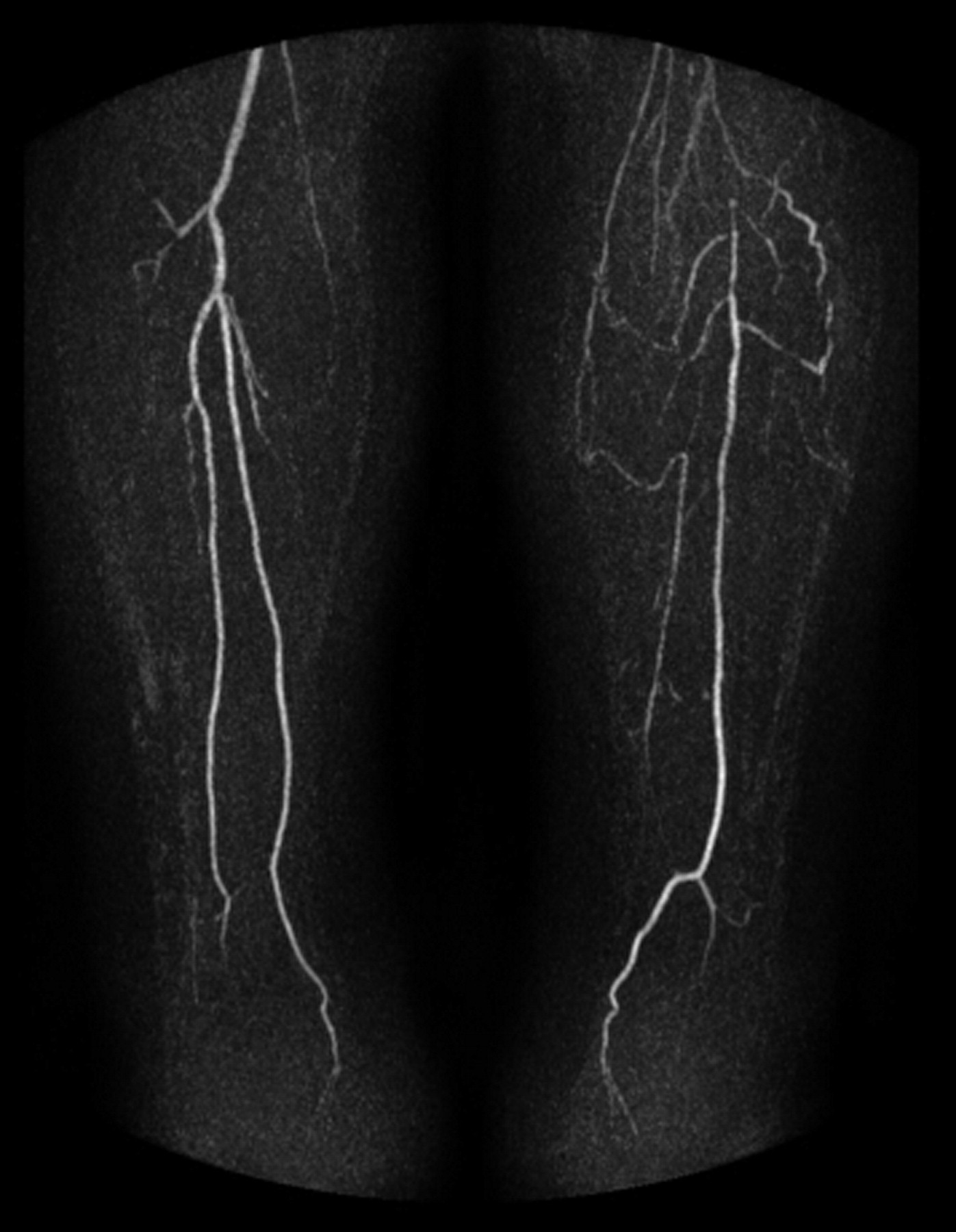
Lower limb contrast-enhanced MRA at calf level in patient with left critical lower limb ischaemia showing occlusive tibial artery disease

Thoracic great vessel imaging with (
Nephrotoxicity of GBCA
While commercial gadolinium chelates are more nephrotoxic than iodinated contrast media in equimolar amounts this has not been a clinical problem for MRI as they are used in much lower doses than in X-ray techniques such as CT scanning and invasive angiography. Several trials of gadolinium contrast agents specifically in patients with renal impairment found no adverse effects on renal function. While a few individual case reports of gadolinium contrast-induced nephropathy at clinical doses in patients with pre-existing renal insufficiency have been published the patients involved had the same risk factors as for CIN with iodinated contrast media suggesting similar mechanisms of toxicity rather than anything specific to the gadolinium itself. These cases were, however, very much the exception, and the incidence of CIN at clinical MRI doses appears to be very low. Indeed, there are several reported series of the use of gadolinium contrast agents in quite high doses as alternative X-ray attenuating compounds to iodinated contrast media in patients seen as high risk for CIN, with apparently no deleterious effects on renal function, though this practice is not generally recommended.
One feature of some of the GBCAs is interference with assays of blood for various analyses, particularly for serum calcium. This has been most often observed with gadodiamide (Omniscan). Even in patients with normal renal function, assays for serum calcium on blood samples taken immediately after gadodiamide administration can falsely indicate hypocalcaemia. This effect is more pronounced and prolonged in patients with renal impairment but the patients exhibit no clinical features of hypocalcaemia and the effect is temporary.
Overall, it was thought that gadolinium-based contrast agents for MRI were essentially safe in patients with renal impairment. On this background with the advent of CE-MRA techniques in particular the use of gadolinium contrast in patients with chronic kidney disease expanded as these patients are not only at high risk from invasive angiography for a variety of reasons, but for those not yet on dialysis CIN must be avoided as every mL/min of renal function that can preserved is vital to improving prognosis.
Nephrogenic systemic fibrosis
In 2006 reports were published linking the use of GBCAs with a hitherto little-known condition, nephrogenic systemic fibrosis (NSF) that had first been described by Dr Shawn Cowper in 2000 as a scleromyxoedema-like skin thickening in patients on dialysis that the authors termed nephrogenic fibrosing dermopathy. The cause, however, remained obscure despite intensive investigation and various theories such as a potential link to the use of erythropoietin were proposed but never proven. The condition was renamed nephrogenic systemic fibrosis once it was determined that the fibrosis not only affects the skin (where adjacent to joints it can lead to contractures and hence impaired mobility) but also internal organs such as muscles including the diaphragm and heart. In some patients localized non-progressive skin thickening and induration may be the only manifestation though this can be particularly problematic if this interferes with dialysis shunt access. In other patients (a minority) the disease is relentlessly progressive and can be fatal, usually through the development of a hypostatic pneumonia. As yet there are no effective treatments though in some cases regression has followed improvement in renal function, particularly after transplantation and recently there was a report that the use of Imatinib mesilate (Gleevec), a tyrosine kinase inhibitor, can be beneficial.
The link to GBCAs was first proposed by Thomas Grobner (an Austrian nephrologist) when he observed that a cohort of his patients with NSF had all recently had contrast-enhanced MRI studies. In the paper making this link he stated that the contrast used was ‘gadolinium DTPA’. However, after later consultation with the radiologists involved this was retracted and a correction published as the agent implicated was gadolinium DTPA-BMA (gadodiamide). Since then other groups have corroborated this association finding an incidence of up to 5% in patients in severe renal failure administered gadolinium-based contrast agents subsequently developing NSF. The second report was that of Marckmann and Thomsen from Copenhagen following which the FDA issued a warning in June 2006.
After these initial published reports and the FDA warning we in the West of Scotland decided to investigate our own local experience. We did this by means of a large retrospective case control series as we were able to cross-reference the electronic patient records for the whole renal failure population for six years (between 1 January 2000 and 1 July 2006, n = 1826) with the radiology electronic records to determine GBCA-enhanced MRI examinations performed in the whole group (577 examinations in 425 patients) and their GBCA dose exposure. We presented our findings at the 2007 ECR in Vienna and this work was later published in Radiology. We found a NSF incidence of 0.77% in all patients on dialysis and 3.1% of the subgroup of these patients who had undergone gadolinium contrast-enhanced MRI. Interestingly, one patient with NSF had not had any gadolinium contrast despite an intensive search of all records. We also found a positive association between the total cumulative dose received and the development of NSF – indicating a form of dose–response relationship, i.e. those patients exposed to higher doses or repeat examinations were more likely to develop NSF. However, it should also be noted that of course this means that nearly 97% of these patients on renal replacement therapy did not develop clinical features of NSF and as such a clear causation was not proven, rather a strong association.
Over the last two years there have been several other studies with similar findings, and further work indicating a role for gadolinium is the finding of gadolinium retained in the skin biopsy specimens from NSF patients even many months after contrast exposure. Currently the most commonly-held theory is that transmetallation is occurring with the gadolinium cation (Gd+++) being exchanged from the chelate for other cations (e.g. zinc or iron), this occurring perhaps related to disturbed acid-base balance in these patients along with the very prolonged time that these agents remain in the body with their primary route of elimination disrupted. Although the term ‘free’ gadolinium is often used, it is in fact never actually free but would be immediately bound to a suitable anion such as phosphate. How the gadolinium then mediates the development of NSF is not clear but it is thought that somehow there is stimulation of circulating fibrocytes (originally from the bone marrow) that migrate to the extravascular space and initiate inappropriate collagen deposition resulting in the clinically manifest disease process. However, clearly the majority of patients in renal failure who have had GBCAs administered have not developed NSF and as yet the other factors that determine the development of this disease have yet to be elucidated.
In the meantime there are many questions as to what we can do in order help prevent this condition occurring with our currently fairly limited knowledge.
Renal failure
Renal failure is a requirement for the manifestation of this condition, but at just what level of renal impairment does the risk become a clinical problem? From the published investigations so far it would seem that the vast majority of cases have occurred in patients with stage 5 chronic kidney disease (CKD) (i.e. effectively those at the stage of requiring dialysis or established on dialysis). This equates with an estimated glomerular filtration rate (eGFR) of less than 15 mL/min. While there have been a few cases with estimated GFRs greater than this they have all been in the context of acute renal injury where estimation of GFR using the formulae designed for chronic renal disease markedly underestimates the actual degree of renal impairment. Investigations looking into the occurrence of NSF in patients with stable less severe renal disease (CKD stage 3 moderate, eGFR of 30–59 mL/min/1.73 m2 and CKD stage 4 severe 15–29 mL/min/1.73 m2 have confirmed that this is a disease limited to those with established renal failure (CKD stage 5) and acute kidney injury scenarios.
Dialysis
If renal failure and prolonged contrast agent presence in the body are at the root of the problem then does dialysis immediately after contrast administration for MRI help? Currently the role of immediate post-MRI dialysis is uncertain, while there is little positive evidence that it can help to avert NSF it is theoretically attractive and the current ACR guidelines recommend its use. However, it is likely this dialysis really does need to be immediate, as NSF has certainly occurred in patients despite same-day dialysis post-MRI. This is clearly only practicable where patients already have dialysis access in place prior to the MRI scan. Perhaps equally or more important is to have had the patient adequately dialysed prior to the administration of GBCAs as there certainly seems to be increasing evidence that poor dialysis prior to GBCA enhanced MRI is a risk factor.
Dose of contrast agent
At what dose of gadolinium contrast agent is there more likely to be a problem? The doses associated with NSF have mainly been in the 0.2–0.3 mmol/kg range (i.e. double and triple ‘standard’ dose) as has been often used for CE-MRA and cardiac studies with few reports of NSF following single/standard dose administration. This correlates with the increasing use of these types of examination in the timeframe in which NSF has been observed.
Contrast agent type
A crucial question is whether the various different GBCAs are more or less likely to predispose to the development of NSF? The question as to whether any particular agent is ‘safer’ than any other is as yet difficult to be certain about but there is increasing evidence of differences between the compounds. The large majority of reported cases have been with gadodiamide with fewer involving gadoversetamide and gadopentate dimeglumine – all linear chelates. There are none confirmed following sole administration of gadobenate dimeglumine (one of the linear chelates with higher stability indices and some hepatobiliary excretion) and none to date with sole administration of any of the cyclic chelates gadoteridol, gadoterate meglumine or gadobutrol. If transmetallation is an important step in the pathogensis of NSF then there are theoretical reasons why some of these agents may be more stable and resistant to this process and hence safer as they are less likely to allow gadolinium to become unbound. In general the cyclic chelates are more stable than linear ones having higher thermodynamic, conditional and kinetic stability constants. Within these classes, the ionic chelates are felt to be more chemically stable than the non-ionic compounds. Hence the non-ionic linear chelates (such as gadodiamide) are held to be the least stable and most likely to allow release of gadolinium; this is borne out in in vitro and small animal studies. The potential for hepatobiliary excretion of some of the agents may be a theoretical advantage for administration in patients with renal failure (but preserved hepatic function) though as yet there is no clinical evidence to support this supposition.
Other factors
Given that most patients in renal failure administered GBCAs do not develop NSF, other factors must contribute to NSF development, but what are they? The studies evaluating patients so far have of necessity been retrospective and therefore uncontrolled. Investigators have searched for other linking factors in these groups such as the nature of the underlying renal disorder, HLA type, degree of acidosis at the time of contrast administration, type of dialysis, erythropoietin treatment, iron levels, phosphate-binding therapies, etc. So far none of these other features has been conclusively confirmed as being related to NSF development though there are suspicions regarding erythropoietin as this is a bone marrow stimulator which may invoke circulating free fibroblasts. High phosphate levels in end-stage renal disease may promote transmetallation – a recent study of chelate stability in plasma found reduced stability when non-ionic linear chelate GBCAs were incubated with phosphate enriched plasma. The converse of this question is of course what factors in these patients are protective against the development of NSF – this is also yet to be answered but could be equally important if ascertained that this is modifiable. Protection could then be given to allow safer GBCA enhanced MRI studies where required.
Practical considerations
In practice the implications are that radiologists and radiographers have to know more about their patients prior to MRI scanning than previously. There is now a requirement to know about renal functional status at the time of scan request prior to scheduling, particularly for examinations mandating GBCA administration and this requires education of the referrer. We also need to ask additional questions directly of patients as part of the safety questionnaire prior to MRI scanning in the same way that we screen for pacemakers, metallic ocular foreign bodies, et cetera. A simple question such as ‘Do you have diabetes, high blood pressure, heart failure or any kidney problems, kidney failure or have you ever had dialysis?’ can be used to exclude renal impairment with high accuracy and in those patients in whom renal dysfunction is not excluded by this then knowledge of eGFR is required.
To prevent the possibility of CIN we should ensure that our patients are definitely not dehydrated and if renal function is mildly or moderately impaired consideration should be given to actively ensuring good hydration by preparation with intravenous fluids as we do for iodinated contrast media.
Where patients with severe renal impairment are considered for MRI with contrast, a judgement needs to be made as to whether the risks of GBCA use as we currently perceive them outweigh the risks of alternative imaging techniques such as those for vascular imaging, the hazards of conventional arteriography with arterial puncture, ionizing radiation and iodinated contrast media. If GBCA are to be used then the lowest dose feasible is currently advocated (such as half the usual dose) and here GBCAs with increased specific relaxivity could be advantageous. The formulation of the GBCA used also appears to be important with the cyclic chelates having highest stability constants, indeed there are currently no unconfounded cases of NSF published in the peer-reviewed literature in association with any of the cyclic agents. When the scan is planned close liaison with the patient's renal physician is clearly important, particularly in order to optimize the patient's milieu interieur with dialysis both prior to the study and also to schedule dialysis immediately post-procedure where this is practicable.
Conclusion
GBCAs remain extremely safe for the vast majority of patients and examinations notwithstanding the recent links to NSF in patients with established severe renal failure. The finding of a potential connection between GBCAs and the development of NSF in patients with severe renal failure is a reminder that as radiologists we must remain vigilant to the safety of all the procedures that we perform. The state of our knowledge regarding NSF and GBCAs continues to evolve and as it does guidelines and practice will clearly develop and radiologists involved in MRI will have to keep abreast of these changes. I believe that the re-assessment of the safety of these agents will lead to a better understanding of them by the radiology community. The necessary update in education of all healthcare professionals involved in the care of patients undergoing MRI and the increased attention paid to the patient as a whole can only ultimately be for the good.