
Abstract

Introduction
Blood clots occurring in the deep veins of the legs (DVTs) are often symptomless and may resolve without medical intervention. However, sometimes they can cause painful swelling of the leg and more seriously can travel through the body's blood vessels eventually getting lodged in the lung (pulmonary embolism [PE]), which can be fatal. Venous thromboembolism (VTE) is also associated with long-term morbidity for a proportion of patients, known as post-thrombotic syndrome.
Major surgery is one of the biggest risk factors for VTE. Factors include venous stasis due to compression of veins during surgery, increased coagulability of the blood, and periods of immobility, both in the operating theatre and subsequently during recovery. Surgery on the hip and knee seems particularly prone to VTE.
There are a number of types of prophylaxis that can be used to prevent VTE. They include:
Mechanical prophylaxis (including foot impulse device and compression stockings); Drug prophylaxis (including low-molecular weight heparins or fondaparinux); Combination prophylaxis (i.e. both a mechanical method and a drug used concurrently).
Drug prophylaxis is more efficacious than mechanical at reducing VTE but is associated with increased bleeding. A key question is do the benefits from reducing VTEs outweigh the costs of increased bleeding. Economic evaluation seeks to answer this question by carefully quantifying each of the consequences of different prophylaxis strategies.
Health economic evaluation
Health economic evaluation can be defined as the comparative analysis of costs and health outcomes between two or more alternative intervention. 1 There are two key elements: (1) there must be alternatives compared; and (2) health outcomes must be accounted for in some way, as well as the financial costs of resources. The purpose of any health economic evaluation is to inform decision-makers about the relative cost-effectiveness (value for money) of healthcare interventions compared with other interventions elsewhere in the health sector. No health service has enough resources to conduct every clinically effective intervention therefore some clinically effective interventions need to be prioritized and others avoided. For a health service with a fixed budget, to maximize population health, it will have to prioritize those interventions that yield a high health gain per pound/dollar/euro spent over those that are less cost-effective.
One form of economic evaluation that is quite commonly used in decision-making is cost–utility analysis. This is where health outcomes are measured in terms of quality-adjusted life-years (QALYs). The QALY incorporates both life expectancy and health-related quality of life by weighting each year by the level of quality of life measured on a 0 to 1 scale (where 1 is the best quality of life imaginable and 0 is equivalent to death). A year in full health is equal to 1 QALY and a year in 50% health is equal to half a QALY. Figure 1 illustrates the QALYs for a patient with a rather poor prognosis, it shows that under Intervention A, this group has a life expectancy of 1 year and has declining quality of life over that time. The QALYs are equal to the area under the ‘Intervention A’ line. With Intervention B the life expectancy for this group is increased and quality of life is better for the whole time. The QALYs gained from Intervention B compared with A is indicated by the area in between the two curves.
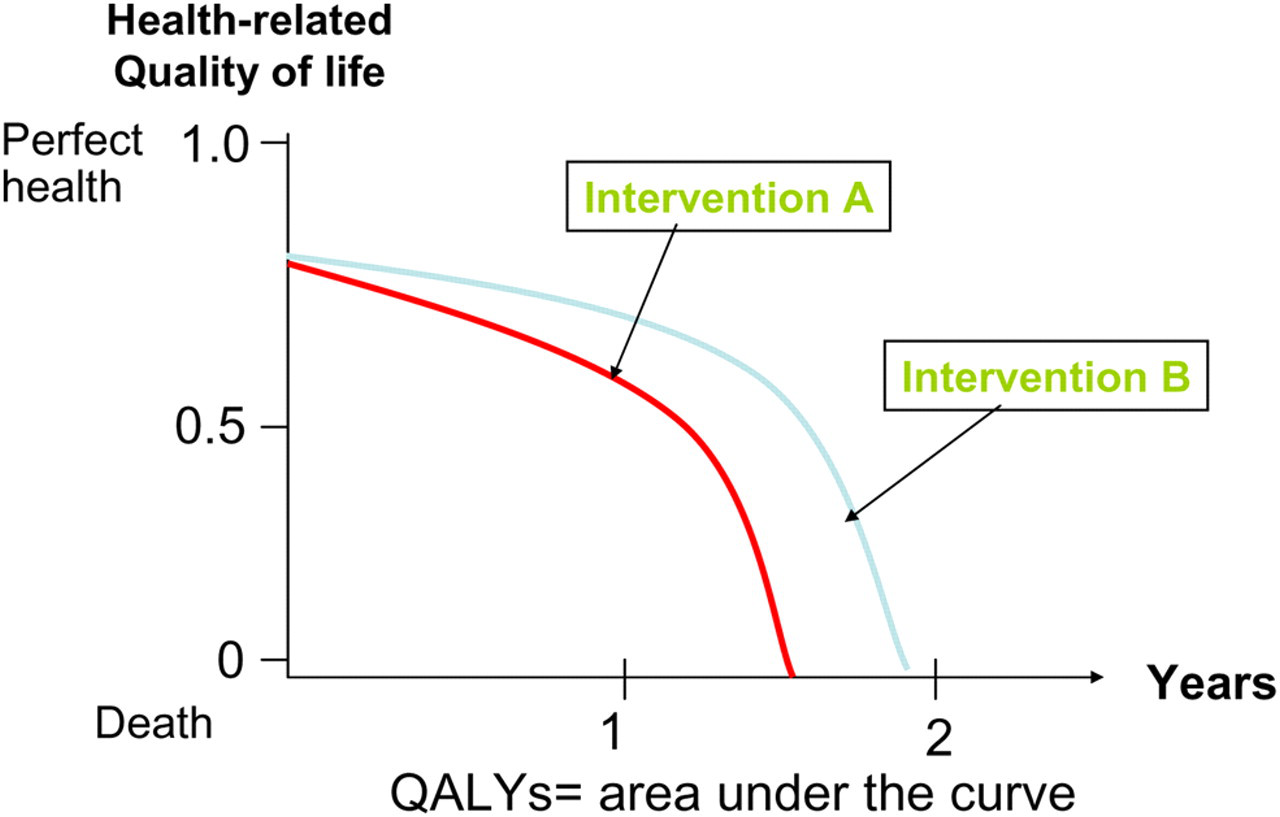
The quality-adjusted life-year (QALY)
To assess whether Intervention B is good value we need to know also the difference in costs between the two interventions. In economic evaluation we included not only the cost of the drugs or devices involved but also the subsequent treatment costs and cost savings. In the case of VTE prophylaxis we include the costs of treating bleeding and the cost savings from having to treat fewer VTEs.
If Intervention B was less costly than A then the decision is quite simple: we go with B because it both increases health (QALYs) and it decreases cost – in this case we say that B ‘dominates’ A. Often we find that one strategy is both more effective at increasing QALYs but it increases cost. In this case we calculate the incremental cost-effectiveness ratio:
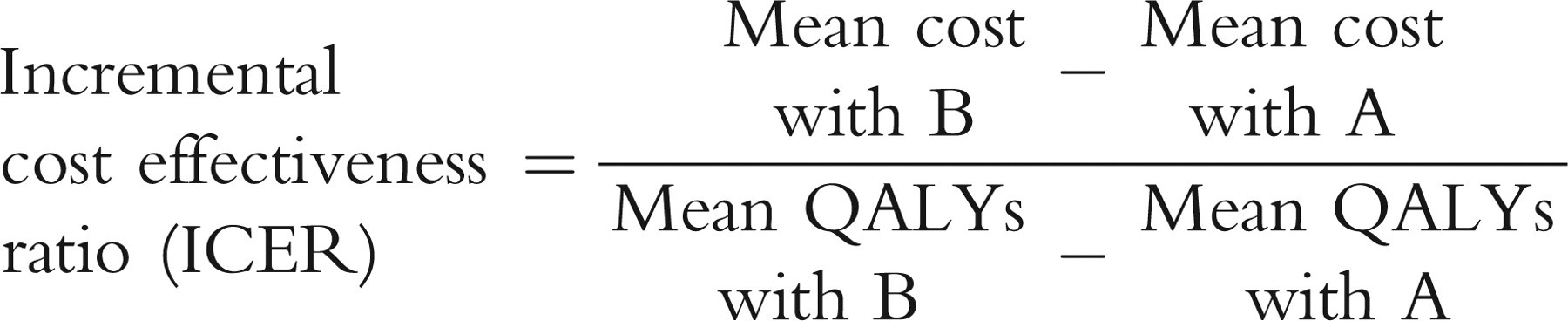
The higher this figure is the more we have to pay for each QALY gained and the less cost-effective is Intervention B. But how high does it have to be for us not to recommend B? Well it depends on the price of healthcare inputs and the budget of the health service and therefore it will vary from country to country. It is a bit of a grey area since to know this cost-effectiveness threshold precisely one would need to have the costs and QALYs associated with every possible intervention across the whole health service. The National Institute for Health and Clinical Excellence (NICE) has suggested that below an incremental cost-effectiveness of £20,000 per QALY gained interventions should be considered cost-effective and between £20,000 and £30,000 additional justifications are required. 2 These benchmarks are used by the NHS in England and Wales.
Methods
NICE commissioned the National Collaborating Centre for Acute Care to produce cost-effective recommendations for venous thromboembolism (VTE) prophylaxis for all surgical patients. A systematic review of clinical evidence and a cost-effectiveness analysis were conducted. Detailed reporting of the methods can be found in the full guideline. 3 NICE sets certain standards for conducting economic evaluations so that all interventions are considered by the same benchmark. We followed the NICE ‘reference case’, which meant that only health service costs were included and future costs and QALYs were discounted at 3%. 4
General model structure and parameters
A cost–utility analysis was conducted. It compared mechanical prophylaxis with different types of drug prophylaxis and combination (drug and mechanical) prophylaxis.
Figure 2 represents the structure of the model for a strategy. For each strategy the mean QALYs and mean costs are determined by the number of VTE events (subdivided in to symptomatic DVT, fatal PE and non-fatal symptomatic PE) and the number of bleeding events. We assigned QALYs and treatment costs to each outcome. The probability of each outcome varies between strategies.

Simplified representation of decision tree
The effectiveness of the different strategies at reducing DVTs was derived from a network meta-analysis 5 of surgical thromboprophylaxis randomized controlled trials (RCTs). The relative risk (RR) reduction of each prophylaxis strategy was pooled together from the results of RCTs from all surgical categories. Not every study collected PE data and given the rarity of the event, relative risks are imprecise, so in the model we assumed that the RR reduction for DVTs could also be applied to PE. So if a drug is observed to reduce DVTs by say 60% then it will also reduce episodes of both fatal and non-fatal PE by 60%.
Another network meta-analysis was conducted for major bleeding events, again using data from RCTs. We assumed that the RR increase in fatal bleeds and strokes would be exactly the same as for major bleeding overall.
For our base case analysis, we did not include long-term outcomes such as post-thrombotic syndrome.
Incorporating the consequences of bleeding
Definition of major bleeding varies greatly between trials. We chose to accept the definition of each trial included in our systematic review (selecting a specific definition would have ruled out most of the evidence). Given the difficulties in defining bleeding, it was decided not to extract data on minor bleeding. Hence minor bleeding was not used in the model.
The RR increase in major bleeding was estimated for each drug prophylaxis strategy from the network meta-analysis (e.g. LMWH vs placebo: RR = 1.5; fondaparinux vs placebo: RR = 2.2). Mechanical prophylaxis is not known to increase bleeding.
The baseline risk of major bleeding (that is the risk without prophylaxis) was taken from the placebo arms of the trials in the network meta-analysis. It was found to be about 2% for both general surgery and total hip replacement.
The number of major bleeding events for a particular prophylaxis strategy is defined as the baseline risk multiplied by the relative risk. So in the case of LMWH use in general surgery the 2% × 1.5% =3% of patients would incur major bleeding.
The cost of treating bleeding is as variable as the definitions of major bleeding. To estimate the initial treatment cost we estimated the average cost using NHS Reference Costs 6 (this is a database of every hospital admission in England): the average cost of treating a gastro-intestinal bleed was £1000 or £2100 for complicated procedures. For some patients the bleeding would have longer-term implications – we have labelled this group as stroke since an intra-cranial bleed would be one such case. For the small group of major bleeds that are intra-cranial we added the cost of stroke care (£7700 in the first year 7 ).
In addition to the treatment cost associated with bleeding we attempted to estimate the impact on QALYs. A systematic review 8 of bleeding in surgical thromboprophylaxis trials showed that only about 1% of major bleeds are fatal. For these patients, we assume that in the absence of the bleed they would have had the same life expectancy as the rest of the patients undergoing that type of surgery. For general surgery patients the cost of a fatal bleed would be in the region of 22 years per death, based on population mortality data.
For those patients with an intra-cranial bleed quality of life was reduced by 50% in the first year. 9
Results
Detailed results are reported in the full guideline. 3 Here we present only an overview.
Base case analysis
Mechanical prophylaxis was found to be highly cost-effective at most risk levels and the guideline group considered that this should be the first line of prophylaxis. We then posed the question at what risk level would it be cost-effective to add a drug.
Figure 3a shows the base case results, presented for different risk levels. The blue cells indicate where combination (drug and mechanical) prophylaxis was cost-effective and the yellow where mechanical-only was optimal. Given our estimates of baseline risk of VTE and major bleeding, it seems that combination prophylaxis is cost-effective for total hip replacement but not cost-effective for general surgery. Since general surgery is near to the threshold, it would seem likely that combination prophylaxis would be cost-effective for subgroups with additional risk factors.
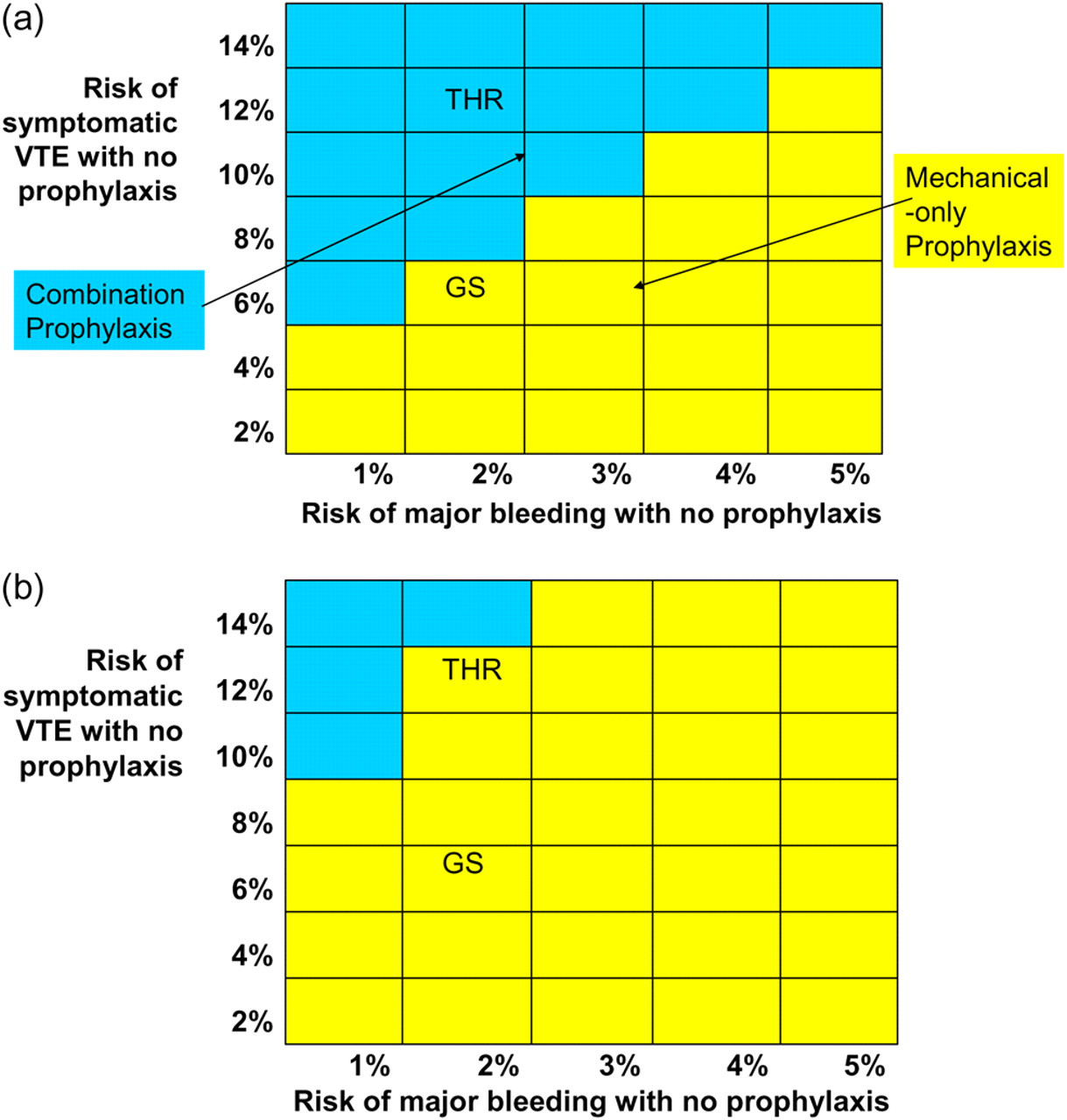
Results by baseline risk level. a) Base case results; b) Sensitivity analysis: 5% of major bleeding events are fatal GS = general surgery; THR = total hip replacement
Sensitivity analysis
The results are sensitive (therefore less robust) to the consequences of bleeding. A fatal bleed is associated with a considerable loss of QALYs and therefore the results were sensitive to the fatality rate from major bleeding. So if we assume that 5% of major bleeds are fatal (instead of 1%) then combination prophylaxis becomes much less cost-effective and may not be cost-effective even for total hip replacement (Figure 3b).
The results were also sensitive to some of the other assumptions used to populate the model. For example, when post-thrombotic syndrome was assumed to be prevented by prophylaxis then combination prophylaxis was much more cost-effective and became optimal for general surgery patients.
Discussion
Cost–utility analysis suggests that some form of thromboprophylaxis in surgical patients is highly cost-effective (good value) and this conclusion was robust to sensitivity analysis. In some patients mechanical-only prophylaxis may be optimal but as bleeding risk decreases or as VTE risk increases, adding a drug to the prophylaxis strategy becomes more cost-effective. Hence the prophylaxis strategy offered to patients should vary according to the type of surgery they are having and individual risk factors. Exactly what is optimal for different groups is still highly uncertain for the following reasons:
The baseline risk of major bleeding and of PE is difficult to determine for specific patient groups; The effects of prophylaxis on mortality are uncertain. Our model predicts that drug prophylaxis increases life expectancy for general surgery and total hip replacement patients. This has not been proven in clinical trials and our model suggests that the cost-effectiveness of drug/combination prophylaxis is highly sensitive to the bleeding fatality rate; The effects of prophylaxis on long-term outcomes are uncertain. It seems likely that reducing VTE will also reduce the incidence of post-thrombotic syndrome and possibly recurrent VTE and chronic pulmonary hypertension. But quantifying the impact is difficult since trial follow-up has not been long enough; The consequences of bleeding used in this model need refining. For example, in orthopaedic surgery it is often argued that bleeding in the joint can cause infection, which can cause morbidity and lead to costly surgical revision. The costs of minor bleeding may need to be incorporated in addition to major surgery but the reporting of minor bleeding in trials is inconsistent.
The model reported in this paper is the result of 20 years of research. A recent review
10
identified 29 economic models evaluating thromboprophylaxis in orthopaedic surgery. The earliest studies did not include the consequences of bleeding at all. Later studies including this one have added bleeding. Few studies have estimated the impact on life expectancy and quality of life, and not all were based on a systematic review of the clinical evidence. This is the first study to introduce network meta-analysis to deal rigorously with indirect evidence comparisons. Future models will evaluate newer interventions and will ideally be based on more precise estimates of effects on mortality and long-term morbidity.
Economic evaluation can be useful in guiding clinical decisions about treatments that have bleeding complications because it explicitly weighs up the costs and health benefits. It makes decision-making more transparent by explicitly reporting assumptions and data and it can inform research by highlighting key areas of uncertainty.
Footnotes
Acknowledgements
Guideline Development Group: Tom Treasure (Chair), Nigel Acheson, Ricky Autar, Colin Baigent, Kim Carter, Simon Carter, David Farrell, David Goldhill, John Luckit, Robin Offord, Adam Thomas; NCC-AC staff: Enrico de Nigris, Jennifer Hill, Philippa Davies, Carlos Sharpin, Saoussen Ftouh, Peter Katz, Arash Rashidian.
This work was undertaken by the National Collaborating Centre for Acute Care which received funding from NICE. The views expressed in this publication are those of the authors and not necessarily those of the Institute.