
Abstract

Introduction
Fibrinolysis can be defined as the breakdown of stable fibrin strands by plasmin. It is an important physiological regulatory mechanism within the coagulation cascade and is a dynamic, often localized, response. It is controlled by the interaction of stimulators and inhibitors released from vascular endothelial cells, smooth muscle and platelets. Although it is a normal physiological process, in certain clinical scenarios it can be a cause of excessive bleeding. Pathological over-activity of the fibrinolytic system, so-called primary hyperfibrinolysis leads to accelerated clot breakdown and potential haemorrhage. Secondary or ‘reactive’ hyperfibrinolysis is an increased activation of the fibrinolytic system in response to increased activity of the coagulation cascade such as is seen in disseminated intravascular coagulation. Hyperfibrinolysis during or following surgery will be the main focus of this article.
Fibrinolysis pathway
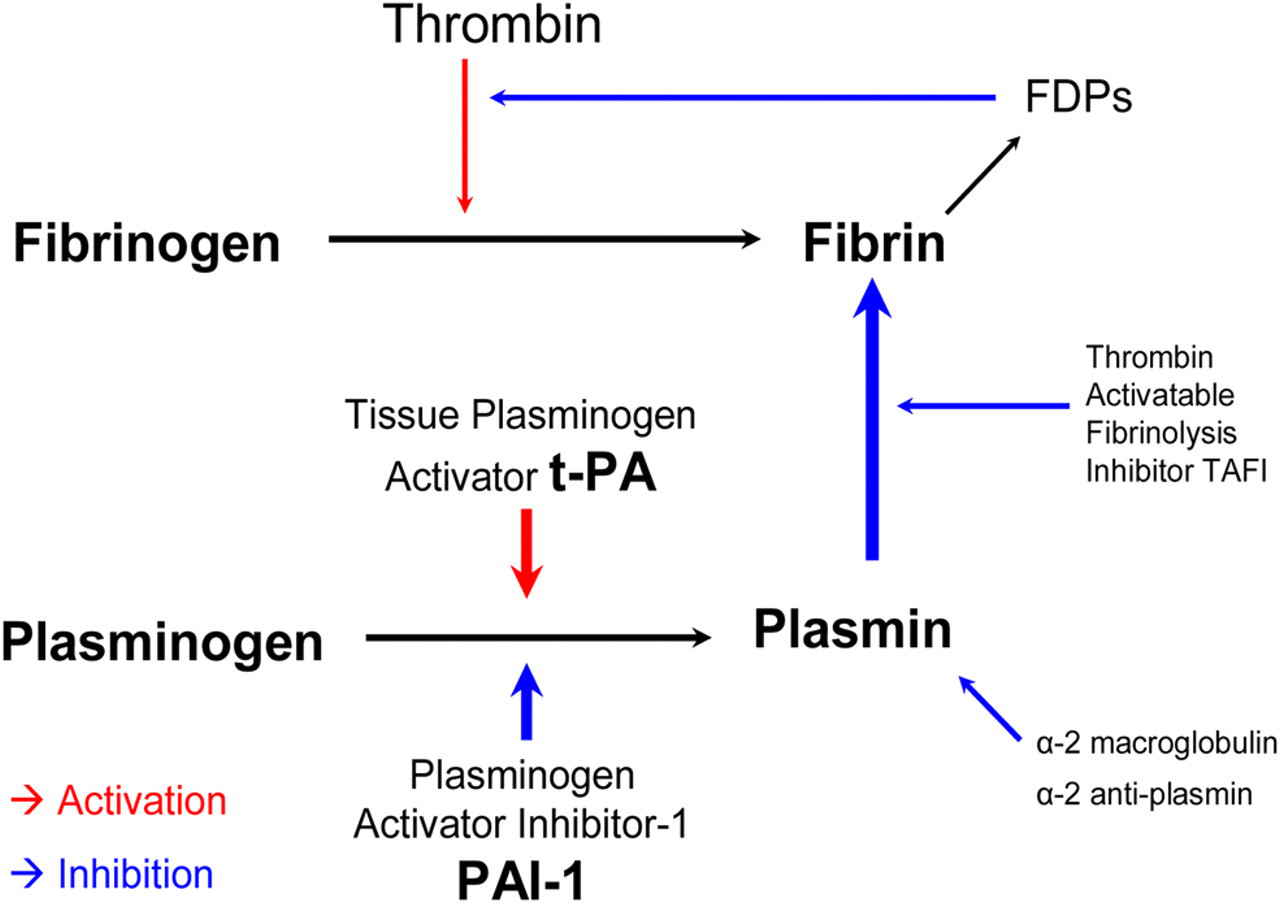
Plasminogen, an inactive precursor synthesized in the liver, circulates in the plasma and is incorporated into clot during clot formation. It is cleaved to the active molecule plasmin by the action of tissue plasminogen activator (t-PA). Plasmin then causes the degradation of fibrin and clot lysis (Figure 1). T-PA is a proteolytic enzyme released by the endothelium in response to trauma, exercise, endotoxin and ischaemia. It is metabolized in the liver and has a short half-life due to a high rate of first pass metabolism. The concentration of active t-PA in the region of the thrombus controls the rate of fibrinolysis. The action of t-PA is inhibited by plasminogen activator inhibitor-1 (PAI-1) and the action of plasmin itself is inhibited by ά-2 anti-plasmin and ά-2 macroglobulin. 1
Fibrinolysis pathway
Disturbances of the delicate balance of clot formation and clot breakdown in patients presenting with thrombotic conditions such as acute myocardial infarction will be familiar to most clinicians. Manipulation of the fibrinolytic pathways for therapeutic intervention (thrombolysis) has saved the lives of many of these patients. 2 However, over activity of the fibrinolytic system is less well recognized. Systemic activation of fibrinolysis due to excessive production, release or activation of t-PA or a reduction of PAI-1, ά-2 anti-plasmin and ά-2 macroglobulin leads to an increased action of plasmin, increased clot breakdown and clinically significant haemorrhage – so-called primary hyperfibrinolysis.
Incidence of hyperfibrinolysis
Primary hyperfibrinolysis has been most extensively described in cardiac surgery with the extracorporeal circuit of cardio-pulmonary bypass causing activation of an inflammatory response and increased fibrinolysis. 3 Plasminogen levels are demonstrated to be reduced and fibrinogen degradation products (FDPs) increased. 4 Many studies show a reduction in blood loss with the use of anti-fibrinolytic agents. Advances in ‘off pump’ coronary surgery and the use of biocompatible cardiopulmonary bypass circuits have been shown to reduce the hyperfibrinolysis effect. 5 Alterations to the fibrinolysis pathway are not confined to the perioperative period. It has been shown that following the initial perioperative reduction in PAI-1 causing hyperfibrinolysis in cardiac transplant patients PAI-1 levels are then significantly increased over the following 12 months post-transplant, possibly explaining features of transplant-related coronary artery disease. 6
The liver is the main site of synthesis and metabolism of the majority of stimulatory and inhibitory coagulation and fibrinolytic factors. For this reason liver disease and liver surgery are often associated with complex coagulopathies. Hyperfibrinolysis in these patients has been recognized for many years. 7 In this field most research has been done in liver transplantation and an incidence of hyperfibrinolysis up to 75% has been reported. 8 The unique situation of the anhepatic phase of surgery gives extra insight into the complex relationships of the whole cascade. Circulating t-PA levels have been shown to be increased at this stage secondary to a cessation of hepatic metabolism 9 along with a reduction in PAI-1 activity. 10 Following graft insertion reperfusion sees a surge of t-PA release 10 associated with increased FDPs and clinical coagulopathy. Recovery begins within 30–60 minutes and there is a return to baseline values at 2 hours post reperfusion. 11
The complex coagulopathy seen in trauma and major haemorrhage may also be due, in part, to hyperfibrinolysis. A study of 87 trauma patients found an incidence of hyperfibrinolysis of 6%. The patients in whom hyperfibrinolysis occurred were those who were most severely injured with a mean injury severity score of 25 in the control group and 75 in the hyperfibrinolysis group. 12 In a study of eight patients who developed coagulopathy undergoing surgery for ruptured AAA, Adam et al. 13 found five had evidence (increased t-PA activity) of hyperfibrinolysis.
Hyperfibrinolysis has also been reported in pregnant HIV positive women treated with anti-retroviral therapy at the time of delivery 14 and as a cause of excessive bleeding in patients with amyloidosis. 15 There are also reports that coagulopathy in anaphylaxis 16 and endotoxaemia 17 can be demonstrated to be due to fibrinolysis.
It could be easy to assume that all coagulopathy for which there is no obvious cause is due to fibrinolysis however a recent study in 49 patients undergoing radical prostatectomy found no evidence of hyperfibrinolysis despite the prostate gland being a recognized source of t-PA release. 18
Measurement
The degree of fibrinolysis can be assessed indirectly with fibrin degradation product (FDP) measurement however standard laboratory tests of coagulation cannot easily identify it. This poses a problem for the clinician suspecting hyperfibrinolysis as a cause of excessive bleeding during surgery. PT, APTT, platelet count and fibrinogen level can all be within normal limits despite the presence of severe fibrinolysis causing clinical effect. Euglobulin lysis time (ELT) provides a measure of the action of plasminogen activators and plasmin. Abnormally short lysis times (less than 2 hours) are diagnostic of hyperfibrinolysis however the time taken to perform these tests and the sometimes transient nature of hyperfibrinolysis in an often rapidly changing surgical scenario means this test is of little clinical use.
Thromboelastography
Thromboelastography is a quick, simple, point-of-care method of assessing global clot function. It can give a clear visual and quantifiable measure of fibrinolysis as well as indicating other abnormalities of coagulation via a graphical display. It was developed in 1948 with first clinical use in 1966 and is widely used and validated in both cardiac and liver surgery. 19
A sample of whole blood is placed into a heated measuring cup into which a pin connected to a transducer is suspended. The cup rotates in either direction every 4.5 seconds. Transfer of the rotational forces of the cup to the pin occurs only after fibrin-platelet bonding has linked the cup and the pin together. Increasing clot strength increases the magnitude of pin movement with the cup this is reflected in an increase in amplitude seen on the graph. If no clot is present the pin does not move and a straight line is seen.
Native samples can be tested at the point of care if the blood can be transferred to the measuring cup within 4 minutes of sampling. Alternatively a citrated specimen can be sent to the laboratory where it is reactivated with calcium and then tested. A second sample cup containing heparinase may be tested simultaneously (allowing assessment of heparin effect on any abnormal result). Kaolin or other activator of coagulation may be added to the sample to reduce the time taken for clot formation and give meaningful results within 15 minutes.
Rotational thromboelastography (ROTEM®) is an updated computerized model of the thromboelastograph (rotation is detected by an optical detector). It is more robust and is less susceptible to interference from mechanical shocks and vibrations. It has been validated for use in a clinical setting 17 and allows addition of different reagents to give an in vitro assessment of treatment options, e.g. Aprotinin in fibrinolysis, Cytochalisin D in platelet inhibition.
Information gained from TEG and the expected findings seen in a patient with fibrinolysis are outlined in Table 1. Figure 2 shows a TEG trace from a patient with a normal coagulation-fibrinolysis profile. Figure 3 shows a TEG trace from a patient with hyperfibrinolysis.
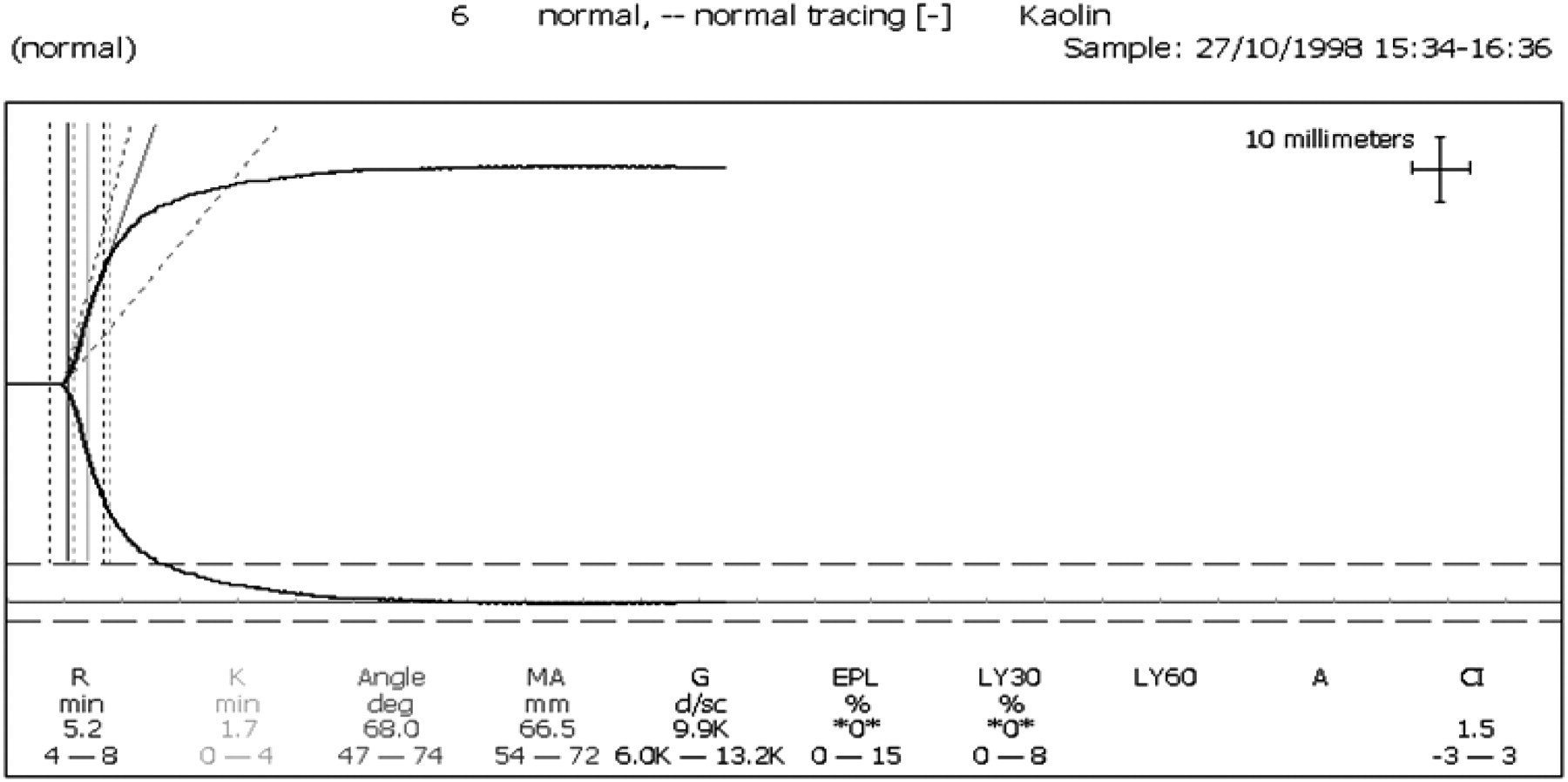
Thromboelastograph showing a normal trace
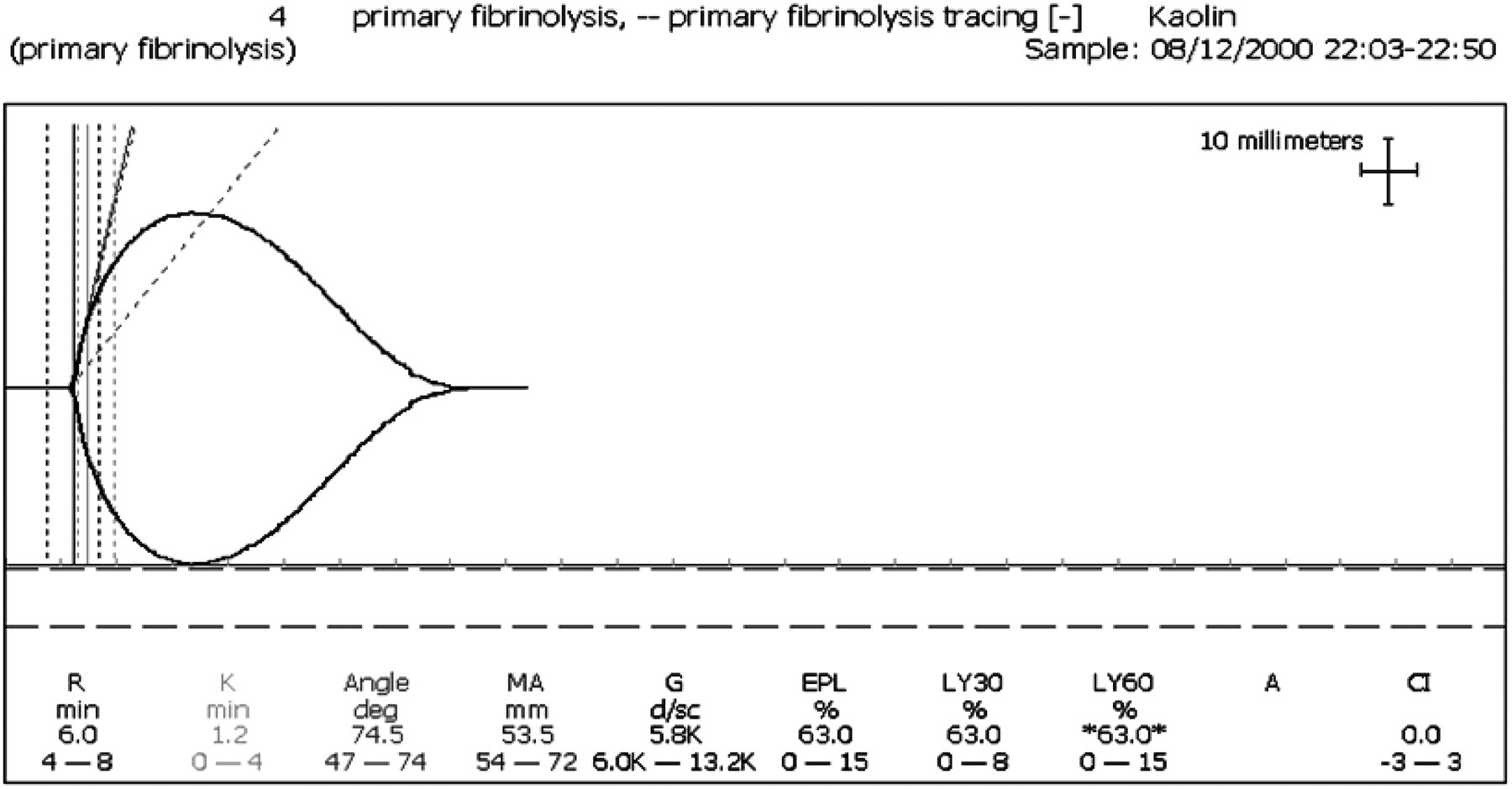
Thromboelastograph in Fibrinolysis showing increased LY30%
Information derived from thromboelastography
Rapid detection of fibrinolysis in the setting of haemorrhage allows clinicians to decide on the appropriate treatment option. The rapidity of results and ease of use of point of care testing allows treatment to be guided by repeated TEG analysis. There is evidence to show that blood product and fluid administration can be reduced by up to one-third by using TEG guided therapy. 11
Treatment of fibrinolysis
The most well-recognized anti-fibrinolytic agent Aprotinin (a serine protease inhibitor) has recently had its licence withdrawn following the publication of several large trials demonstrating evidence of increased mortality 20 and increased risk of renal failure 21 following its use. In the BART study group, 20 2331 high-risk cardiac surgery patients were randomized to receive Aprotinin, Tranexamic Acid or E-Amino-Caproic Acid (EACA) as prophylaxis against fibrinolysis. The trial was terminated early due to a higher 30-day mortality rate in the Aprotinin group relative to both alternate agents.
E-Amino-Caproic Acid and Tranexamic acid have been shown to be safe and effective treatments for fibrinolysis significantly reducing blood loss when compared to control in elective coronary artery grafting. 21 They are both lysine analogues and bind reversibly to plasminogen preventing cleavage to plasmin. Tranexamic acid is used in the UK but is not licensed in the US. The recommended dosing schedule is 0.5–1 gm slow IV bolus 8-hourly, it can also be given as a continuous infusion or orally. The BART study used a bolus dose of 30 mg/kg in 500 mLs of 0.9% saline (after negative test dose) followed by 16 mg/kg/hour until 2 hours post op. Side-effects include hypotension with rapid infusion.
Conclusions
Hyperfibrinolysis is an important, often unrecognized, cause of coagulopathy. It is difficult to detect with standard studies of coagulation and clinical suspicion is required if it is to be recognized. Thromboelastography is a useful diagnostic tool allowing both rapid detection and assessment of response to treatment. Antifibrinolytics can be used as prophylaxis when hyperfibrinolysis is predicted (e.g. cardiac surgery) or in other clinical situations if it is detected.