
Abstract
Acute sinusitis is one of the most common conditions that can present to a wide variety of clinicians ranging from general practitioners, Accident and Emergency, physicians, ophthalmologists and otolaryngologists to intensivists and even neurosurgeons. Delayed diagnosis with failure to recognize and manage (albeit rare) complications can be devastating for patients, potentially resulting in blindness or even death. Management of the condition itself can lead to complications. This article reviews the current guidelines for diagnosis and management of acute sinusitis with emphasis on medicolegal aspects. Adverse events affecting patients with acute sinusitis are also presented illustrating the challenges in the assessment and management of this condition.
Introduction
Inflammation of one or all of the paranasal sinuses is often referred to as sinusitis (be it infectious or non-infectious in aetiology) but otolaryngologists prefer the term rhinosinusitis as there is almost universally concurrent rhinitis too. Sinusitis can be categorized as acute (less than 4 weeks in duration), subacute or acute-on-chronic (more than 4 weeks but less than 12 weeks), and chronic (more than 12 weeks). The vast majority of infectious causes are acute, self-limited viral infections, also known as ‘the common cold’ (acute viral rhinosinusitis) or viral upper respiratory tract infection (URTI).
Less than 2% of URTIs progress to the potentially more serious bacterial sinusitis but the incidence of URTI itself is very high, estimated to be 2–5% per year for adults and 7–10% per year for children. The exact prevalence of acute sinusitis is not known due to variations in defining the condition (and recording) but in Europe, 1–5% of adults are diagnosed with acute sinusitis each year by their general practitioner. Extrapolated to the British population, this is estimated to cost 6 million working days per year and is one of the most common reasons for an antibiotic being prescribed. The most common organisms responsible for acute bacterial sinusitis include Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis.
The official European Position Paper on Rhinosinusitis (2007) definition of bacterial rhinosinusitis is as an increase of symptoms after five days or persistent symptoms after 10 days after a sudden onset of two or more of the following symptoms:
nasal obstruction/congestion; anterior discharge/postnasal drip; facial pain/pressure; reduction/loss of smell.
1
The diagnosis of acute sinusitis is essentially one based on clinical history and examination but due to differing criteria (such as some papers using imaging or bacterial cultures), prevalence varies within the literature. Use of imaging to diagnose the condition or indeed other investigations such as bacteriology are not sufficiently sensitive or specific and, therefore, not recommended.
2
Pathogenesis of sinusitis
To understand the pathogenesis of acute sinusitis it is important to understand the anatomy and physiology of the paranasal sinuses. Briefly, the majority of the sinuses drain mucous secretions (and obtain aeration) through a common pathway, called the osteomeatal complex, into the nasal cavity (Figure 1).

Coronal CT scan showing normal right maxillary and ethmoidal sinuses and patent osteomeatal complex (OMC). On the left there is obstruction of the OMC with evidence of maxillary and ethmoidal sinusitis
Mucus (which traps particulate matter and bacteria) is produced by the mucosa (lining) of the sinuses and is transported by the action of beating cilia through the ostia (opening) of the sinus into the nose. During an URTI the mucosa of the sinuses becomes congested with the ostia also becoming narrowed or even blocked. The increased mucus production during an URTI adds to the inadequate clearance of sinuses with subsequent stasis, increased bacterial load, exacerbating inflammation (and swelling) of the mucosa with further increased mucus production. Increasing stasis of mucus secretions leads to reduced aeration and function of the cilia with even further reduction of mucus clearance resulting in a vicious cycle leading to acute sinusitis.
Complications of sinusitis
Due to the close proximity of the brain, cranial nerves, cavernous sinus and orbit (Figure 1), infection/inflammation of the sinuses can cause loss of vision and/or intracranial complications possibly leading to death if untreated. Hence, early recognition and treatment is crucial.
Complications of sinusitis are categorized as orbital, intracranial and osseous. The ethmoidal sinuses are separated from the orbit (containing the eye and optic nerve) by a paper-thin bone called the lamina papyracea which can be deficient (Figure 2). There can either be direct or vascular spread of sinus infection leading to orbital cellulitis, subperiosteal/orbital abscess with subsequent reduced ocular mobility and reduction of vision, leading to blindness. Any patient with diplopia, orbital pain or eyelid erythema, oedema, opthalmoplegia or proptosis has suspected orbital cellulitis and needs urgent referral to an otolaryngologist in addition to imaging (Figure 3) and assessment by an ophthalmologist.

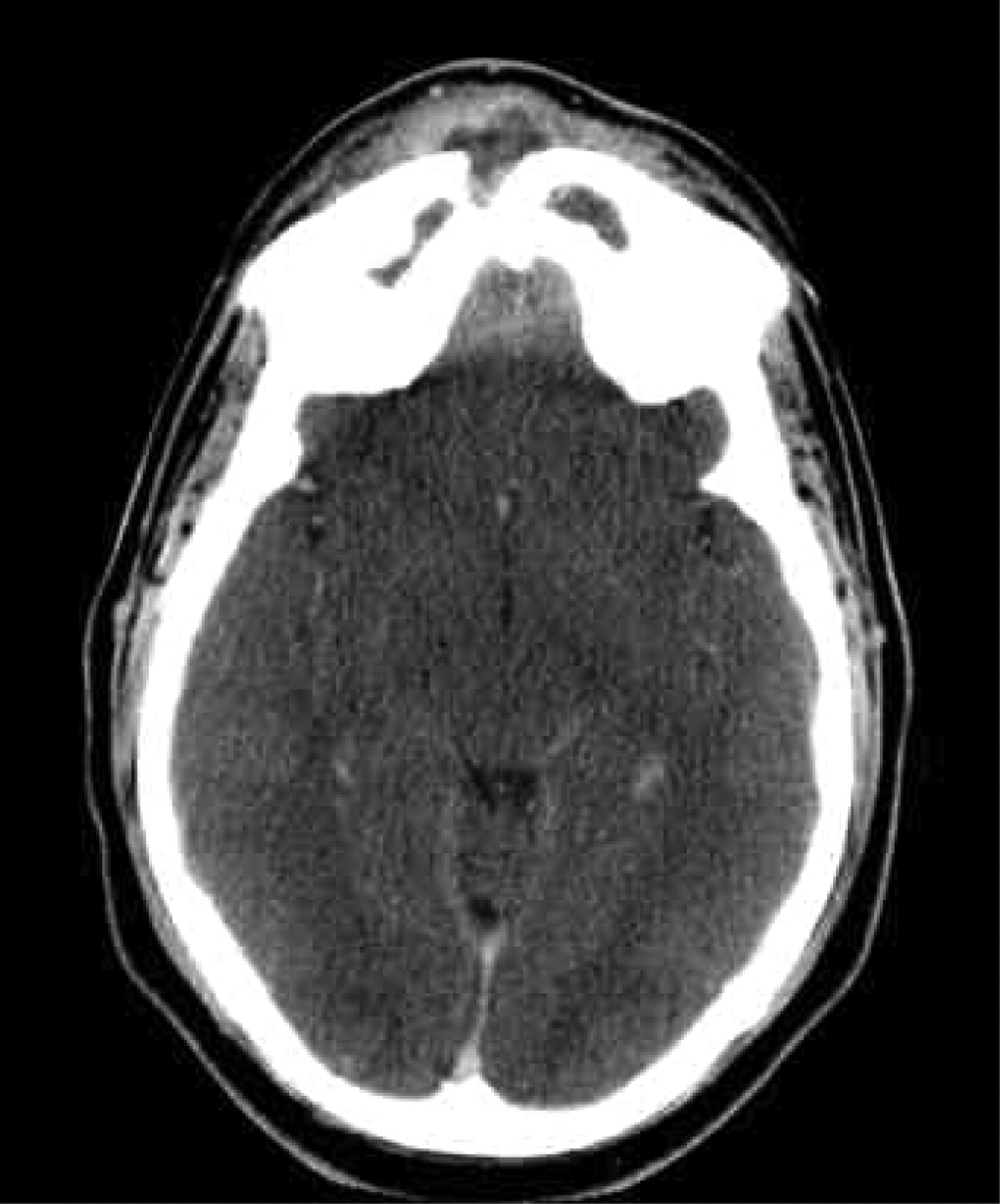
Axial CT scan of normal sinuses. Note the close proximity of the orbital contents to the ethmoidal sinuses (including the orbital apex through which the orbital nerve runs) and the brain to the sphenoid sinuses
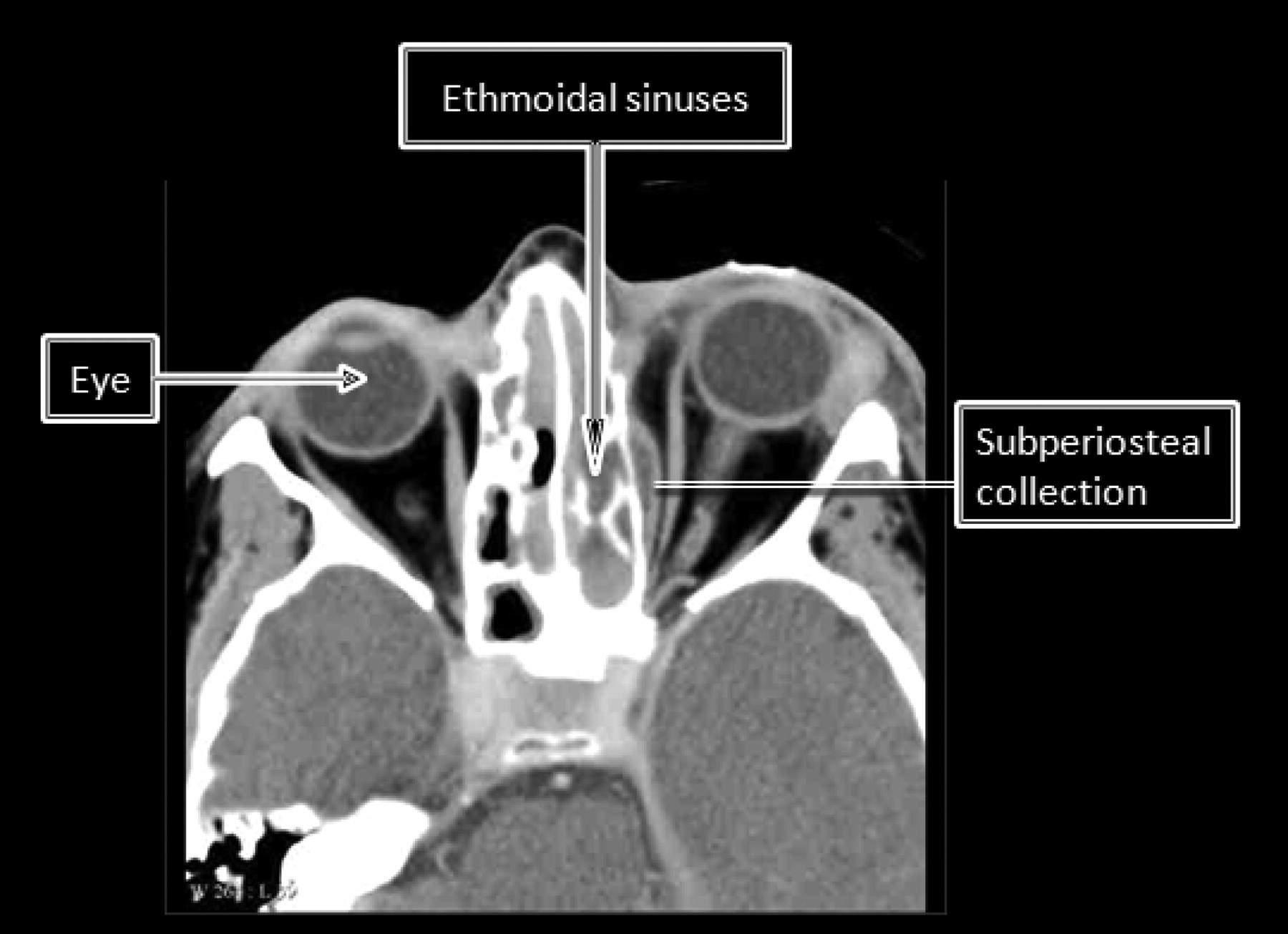
Axial CT scan of a patient with left ethmoidal sinusitis complicated by a subperiosteal abscess requiring urgent surgical intervention. The ophthalmic nerve is visible on the left extending from the orbital apex to the eye. Note the bowing of the medial rectus caused by the collection with oedema of the periorbital soft tissue
Spreading infection from the orbit (via thrombophlebitis) can lead to cavernous sinus thrombosis. Multiple cranial nerve palsies may result (III, IV, ophthalmic and maxillary branches of V and VI) with patients becoming blind in both eyes and developing meningitis. With a mortality of 30% and morbidity of 60%, this complication is the nightmare scenario and immediate referral should be made in any patient with bilateral signs of orbital cellulitis or retro-orbital deep pain with spiking temperatures.
Meningitis is the most common intracranial complication but others include extradural, subdural, intracerebral abscesses and cerebritis. In patients with sinusitis, any patient with signs of meningism, raised intracranial pressure or fever and persisting frontal (or retro-orbital) headache, altered mental status or focal neurological deficits needs immediate referral to a neurosurgeon. Even when aggressively treated, these complications can lead to varying degrees of permanent loss of function for patients with morbidity of 50% and a 5–10% mortality rate. 3
Osseous complications result from osteomyelitis secondary to sinusitis. The patient usually has symptoms of frontal sinusitis with development of osteomyelitis of the anterior and posterior table (which separates it from the frontal lobe), manifesting to clinicians as a Pott's puffy tumour. Clinically this presents as ‘doughy’ oedema of the skin over the frontal bone (anterior table of the sinus) producing a mass (Figure 4). Crucially, if not treated aggressively (with early referral to otolaryngology) osteomyelitis of the posterior table of the frontal sinus can lead to the above mentioned intracranial complications.
Pott's puffy tumour. Note the erosion of the anterior table of the frontal sinus and enhancement of part of the frontal lobe
Medical negligence in acute sinusitis
Failure to diagnose sinusitis and recognize complications
The first key issue relates to the potential delay in diagnosis. By definition, an URTI cannot be called an URTI if symptoms worsen after five days or persist beyond 10 days – it has to be diagnosed as acute bacterial sinusitis and managed accordingly. Being one of the commonest conditions encountered in medicine, it may present to a wide range of clinicians – from general practitioners to accident and emergency, physicians, otolaryngologists, and even intensivists and neurosurgeons (when severe complications occur). Furthermore, apart from an URTI, acute sinusitis can be mistaken for a number of other conditions causing headaches and facial pain. Complications of sinusitis may develop insidiously and the signs can be subtle (especially with intracranial complications), with the added confounding masking effect of antibiotics.
Below are actual medicolegal cases that the authors have been involved in, highlighting medical negligence in the diagnosis of sinusitis and complications:
A 34-year-old man was admitted in the evening to a teaching hospital with acute sinusitis under the maxillofacial on-call team after GP referral due to failure of oral antibiotics over three weeks. He was found to have bilateral eyelid swelling by the admitting middle grade and instead of assuming bilateral orbital cellulitis with cavernous sinus thrombosis (till proven otherwise), the patient was started on intravenous antibiotics to treat sinusitis. A cursory check of visual acuity (as the patient could not fully open his eyes) revealed no loss on admission but throughout the night the patient complained to the nurse that he was ‘going blind’ in one eye but medical staff were not informed. On the morning ward round, the decision was made to order an urgent CT scan and refer to infectious diseases as the patient did not appear to be responding to treatment but was deteriorating. By the time the infectious diseases consultant attended and referred, the CT scan had confirmed pansinusitis and significant bilateral orbital cellulitis and on examination the patient had lost all vision in one eye and was rapidly losing vision in the other. The otoloaryngology team were immediately contacted and the patient was taken to theatre within 45 minutes to decompress the orbits to salvage what vision was left. MRI confirmed cavernous sinus thrombosis and aggressive management resulted in recovery of vision in one eye but he remained blind in the other. In this case, the GP should have referred to otolaryngology (the more appropriate specialty) and especially as soon as the patient developed unilateral eyelid swelling instead of waiting for bilateral signs. The maxillofacial team should have got an immediate ENT and ophthalmology opinion in addition to a CT scan on admission, which would have led to earlier intervention and potentially less disability for the patient. A male patient self-presented to Accident and Emergency with a swelling on the forehead. He had been swimming three weeks earlier on holiday in Spain and developed sinusitis for which he was on repeated courses of oral antibiotics. Having been referred to the general surgeons he was commenced on intravenous antibiotics. This continued for three days during which he developed increasing headache and then vomiting. Nothing else was done until he dropped his consciousness level (Glasgow Coma Scale 10/15) triggering a referral to neurosurgery and otolaryngology. Despite urgent surgical drainage of the frontal abscess and curettage of the Pott's puffy tumour the patient subsequently died of cerebritis. The patient should have been referred earlier by the GP when the sinusitis was not responding to oral antibiotics and especially when the forehead swelling developed. The patient was then inappropriately referred to general surgery further delaying potentially life-saving management and this complication of sinusitis was not recognized until it was too late.
Misdiagnosis and mimics of sinusitis
Conversely there have also been cases of more serious pathology, such as tumours being mistaken for sinusitis. Any unilateral signs or symptoms should be viewed with concern and early imaging (a CT scan) employed to verify the diagnosis is correct.
There have been litigation cases involving patients treated empirically for extended periods with antibiotics for sinusitis when in actual fact they had inverted papilloma (which subsequently was found to be malignant) and in another patient a neuroblastoma. Below is a litigation case as way of illustration, highlighting the difficulties in diagnosis:
A patient was diagnosed as having recurrent acute sinusitis as they would transiently respond to antibiotics only to present again to the GP soon after the course had finished. This cycle repeated itself for months until the patient was referred to the hospital and the patient was eventually taken to theatre to have a Caldwell-Luc surgical procedure to treat the ‘refractory maxillary sinusitis’. Despite this, the sinusitis recurred and although according to the history, no dental pathology was suspected, the purulent discharge from the sinus grew dental flora. Eventually, a year after the initial presentation, an OPG was ordered and the patient found to have apicitis and removal of the offending upper 6 tooth led to complete resolution of the ‘sinusitis’. Any patient with persisting or recurrent sinusitis should be referred for an ENT outpatient consultation for further investigation. It is important to understand that the roots of the upper teeth can project into the maxillary sinus and dental pathology can mimic sinusitis.
Complications of managing sinusitis
Surgical management of sinusitis and its complications can lead to patient morbidity and even mortality in rare cases. Endoscopic sinus surgery carries with it the risk of damage to orbital structures, with loss of vision and diplopia, in addition to breaching the cranial fossa leading to CSF leakage, meningitis or even brain damage. Open approaches to manage orbital cellulitis or access the frontal sinus can themselves lead to complications such as supraorbital, infraorbital or even supratrochlear nerve damage leading to double vision. Below are cases illustrating some complications of surgical intervention:
A patient failed to regain consciousness after endoscopic sinus surgery, and on arrival at the intensive care unit a piece of cerebral cortex was retrieved from the oropharynx. Subsequent imaging revealed not only an extensive resection of the anterior cranial fossa with brain herniation into the nose, but also instrumentation tracts within the cerebral cortex. The case was considered indefensible due to incompetent, surgical technique and settled early; A child underwent what was considered to be the relatively routine and safe antral washout procedure only to wake up with an infraorbital nerve palsy. It transpired that the trocar, instead of being inserted into the maxillary antrum had gone anterior into soft tissues of the cheek, damaging the nerve; A patient with complications of sinusitis underwent a frontal sinus trephine and woke up with diplopia and a supraorbital nerve palsy. When the Lynch-Howarth incision had been performed for access, it had been extended too far laterally with resulting transection of the supraorbital and supratrochlear nerves; After a Caldwell-Luc procedure, a patient woke up with a supraorbital nerve palsy. Although the infraorbital nerve is recognized to be at risk during this procedure, it became apparent that the cheek retractors resting against the supraorbital rim had caused a neuropraxia of the supraorbital nerve (an avoidable complication).
Most complications of surgery for sinusitis and complications of sinusitis are avoidable with diligent surgical technique. However, it is important to note that despite care being taken by the surgeon, complications of surgery still occur and do not automatically mean the surgical technique has been substandard.
Summary
Patients with symptoms of acute sinusitis present to a wide range of clinicians. It is important to remember the EPOS guideline definition of bacterial sinusitis and the fact that devastating complications can develop insidiously. All clinicians must have a high index of clinical suspicion and promptly refer cases refractory to therapy or anyone who may be developing complications of sinusitis or else face the consequences of potential litigation. Surgical management carries its own risks and although not each and every complication is avoidable or implies negligence, communication of risks (and its long-term consequences) to the patient prior to surgery is best practice.