
Abstract
The concept of the expert patient and self-management has a key role to play in improving patient safety. Empowered health literate patients are more likely to ask questions, to check medication, and accurately report on side-effects and adverse reactions. In addition they are likely to be proactive in their own care and managing their home environment to reduce risk of harm. Greater benefit could be gained by input into the design of patient education and rehabilitation programmes from those responsible in NHS trusts and other bodies for managing risk.
Background
Over the last decade the emphasis for the NHS has increasingly been about putting the patient at the centre of their own healthcare. Expert patients, self-management, health literacy and self-care support are all initiatives that support a patient-centred NHS and are aimed at improving people's ability to manage their health condition more effectively and engage with the healthcare system.
The Expert Patient Programme (available in colour online)
For some, the term ‘expert patient’ conjures up an image of a patient who has spent hours on the Internet reading about the latest treatments and research and then going to their GP demanding that the NHS provides this.
This is not what is meant here by an ‘expert patient’. A more appropriate term may be the engaged patient or health literate patient.
In fact, a key feature of the health literate or expert patient is a willingness to ask appropriate questions, to actively report on side-effects and non-adherence, to report on the trend of the illness and other factors that may affect treatment, such as use of over-the-counter medications and complementary treatments such as herbal remedies.
The underpinning ideas of the expert patient were that:
1
The view of many healthcare professionals is that ‘my patient understands their disease better than I do’; The knowledge and expertise of the patient is an untapped resource; Patients should be more than just a recipient of care – they should have an active role in their healthcare; Self-management or Expert Patient Programmes (EPP) are not simply about educating or instructing patients about their conditions; they are based on developing the confidence and motivation of patients to use their own skills and knowledge to take effective control over life with a chronic illness.
The importance of the role of self-care in improving health and reducing emergency admissions was clearly stated in a NHS strategy document
2
published with the new operating framework.
3
As the Wanless Report of 2002 4 showed, ‘the dividend created by an NHS that promotes health, self-care and early intervention, and that integrates services around patients, is potentially sizeable, amounting to billions of pounds’. The paper goes on to say that ‘Compared with other countries, for example, we have high rates of emergency admissions to hospital for those with diabetes and asthma. Better management of these conditions and better support for self-care and family carers could avoid such distressing experiences, leading to care that is more effective, a better experience and more productive.’
What is the Expert Patient Programme?
The Expert Patient Programme was launched in 2002, initially as a three-year research project.
At the centre of the evaluation was a self-management course originally developed at Stanford University and adapted for use in the UK.
The majority of courses are run over six weekly sessions of 2.5 hours to groups of up to 16 people by tutors and specially trained volunteers with their own experience of living with a long-term health condition(s).
The course's primary objective is to help people to develop the skills and confidence needed to manage their health condition better on a daily basis, making them less dependent on health and social care services and have greater engagement in the management of their treatment (Figure 1).
The course content focuses on five core self-management skills: problem-solving; decision-making; resource utilization; developing effective partnerships with healthcare providers; and taking action.
Topics covered include: making informed treatment decisions; understanding medications and treatment; communication with healthcare teams; as well as diet, fatigue, sleep, pain, anger and depression.
Since the original pilot the programme has been extensively expanded to include disease specific programmes, clinician training and a focus on shared decision-making and care planning.
What effect does the programme have?
The Department of Health published the results of a six-month longitudinal study from 963 participants.
The key outcomes (all statistically significant) involving NHS services are shown in Table 1. 5
Key outcomes involving NHS services
A key piece of feedback is that participants feel that their relationship with their healthcare team is improved. Many feel more confident about their consultations and often write down any questions or concerns in advance so they can use their time productively. Many participants have also reported a reduction in unscheduled visits to their GP as they feel they are effectively managing their condition through other techniques taught on the course.
‘Before I didn't know what my medicines were for and felt stupid asking my doctor. Since completing my EPP course, I feel more confident to discuss my medication and treatment.’
What is also significant is the increase in use of pharmacists. Course participants are actively encouraged to review their medication and ask constructive questions about their treatment. Interviews carried out by EPP CIC with course participants showed that many were not fully aware of the purpose of some of their medications and were often not taking them as prescribed. Many actively sought the help of pharmacists in explaining the different medications. This meant that they were more likely to question changes in medication.
The engaged patient is a key part of reducing risk.
‘After finishing the EPP course, I realized that I was not managing my diabetes very well, so I went to talk to my nurse and asked her to change my treatment plan. I was also keen to find out and discuss new treatment plans. My unscheduled visits to my GP have gone down to nil and now I go after three months just for my scheduled visits.’
‘I learnt how to make an action plan which helps me to take medication regularly. Before EPP, I used to forget to take it so now my action plan helps me to take my medicine when I should, and I feel much better.’
To better understand some of the process at work, patients were asked to take part in a number of in-depth interviews and focus groups sessions.
Summary of findings from the focus group sessions
Better attendance of scheduled visits.
Reduction in Did Not Attend (DNA) rate.
Reduction in unscheduled visits.
Improvement in taking control of treatment plans.
Better communication with healthcare professionals.
Better and regular use of medication to control health condition.
Better self-management skills
Transformation from a patient to a person who can play an active role in society.
Reduction in time off work due to sickness.
The health literate patient as monitor of safety
The process being triggered by self-management interventions is a shift from a pattern of passivity and unconscious non-adherence to one of active engagement, positive adherence and concordance with treatment (Table 2).
Before/after attending an Expert Patient Programme (EPP)
This shift is fundamental to engaging the patient as a monitor of safety. Increased self-confidence and improved communication means that they are more likely to report adverse effects accurately, as well simple things, such as always taking a full list of medications whenever they are seen by the healthcare team.
Improving patient's self-management skills, though, goes further than just affecting medicine management.
If we look at the frail elderly living in the community, falls are a significant issue. A paper published in 2002 showed that: ‘Rate of falls among frail elderly people living in the community is very high and frequently correlates with potentially reversible factors’. 6 One of the key factors the authors cited was depression as well as the immediate environment, such as steps and loose carpets, and general mobility.
One of the main behaviour change methods used on courses is goal-setting.
Participants will often set goals that involve making changes to the home environment, securing additional support and improving mobility. All of these can help reduce risks to the patient in the community.
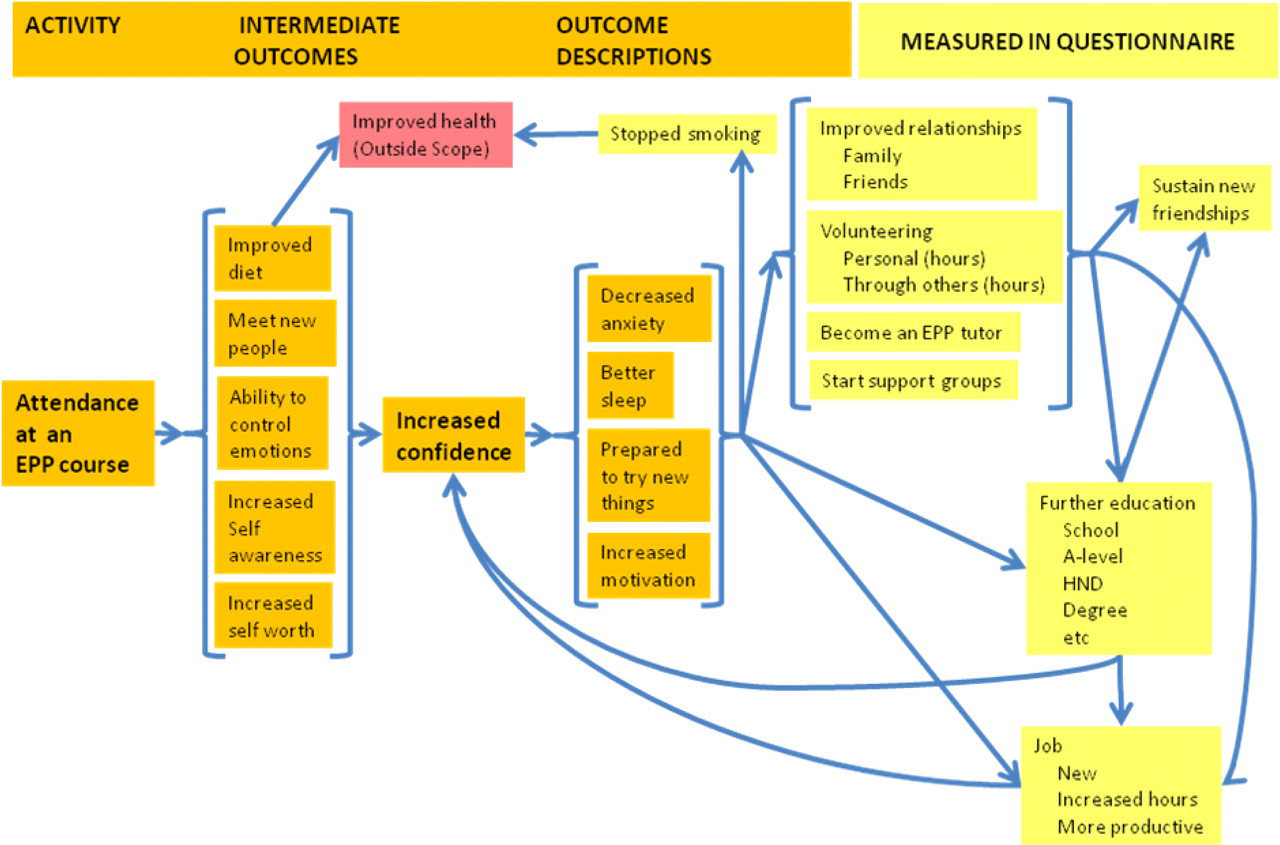
This cycle of setting goals and making small changes leads to an increase in self-confidence that helps reduce anxiety and depression. This, in turn, leads to the person trying out further new activities.
This is fully illustrated in the theory of change model in the diagram below.
It is a reasonable hypothesis to put forward that patients involved in this positive re-enforcement cycle are likely to have fewer adverse incidents.
It is clear that the concept of the engaged or ‘expert patient’ has a role in patient safety, they are more likely to ask questions, to have the confidence to question clinicians and more likely to take greater care of themselves in general.
There is a potential to make these benefits more explicit through developing closer working relationships between those responsible for patient safety in NHS trusts and people who are developing self-management programmes.
Lastly, consideration needs to be given to the training of clinicians to enable them to work with patients in a collaborative way through the development of care plans and using decision-making tools when guiding the patient in making decisions about their treatment.