
Abstract
Introduction
Reporting of adverse events in medicine is an important concept. It is widely accepted that a key element of any healthcare service is the approach that is adopted towards reporting adverse events. Government legislation and the increased number of patient safety initiatives with widespread discussion within the medical literature marks adverse event reporting as an important topic for analysis.
Methods
The Clinical Indemnity Scheme (CIS) provides risk advisory services to state authorities in Ireland. This study will focus on 42,094 adverse events reported across all surgical specialties to the CIS via a confidential weblink (STARSWeb) since 2004. The most common features of each adverse event and closed medicolegal claims processed by the CIS were reviewed as part of this study.
Results
The majority of reported adverse events occur in orthopaedic and general surgery (73% of all cases). Slips/trips/falls are the most common adverse event reported. Doctors report only 4% of the total number of adverse events. The month of October records the highest number of adverse events with the highest frequency of adverse events taking place before 13:00 each day. The most common incident type which resulted in a claim being closed by the CIS was the perioperative/periprocedure incident (50% of all cases).
Conclusions
The CIS report a significant number of adverse events across a range of surgical specialties. A pattern of adverse events being reported during ‘daylight’ hours gives a clear indication that routine surgical operations and procedures carry with them a risk for injury to the patient. Particular months of the year and time of the day are more likely to be associated with reported adverse events. This pattern of events should be highlighted in an attempt to promote safer surgical practice within hospitals during particular times of the day, month or year.
Introduction
Surgical care and healthcare in general is provided in a high-risk environment. Clinical incidents, adverse events and hospital death may occur following the provision of hospital treatment. Between 3.7–16.6% of patients admitted to hospital potentially suffer an adverse event. 1,2 The Institute of Medicine in the United States report from 1999 states that at least 44,000 and perhaps as many as 98,000 die in hospitals each year in America as a result of medical errors. 3 Based on this report it has been estimated that between 500–1500 people may die each year due to iatrogenic injury in Ireland. 4
Definitions of adverse events vary. The Clinical Indemnity Scheme (CIS) defines a clinical incident as ‘an event arising as a consequence of, provision of, or failure to provide clinical care that results in injury, disease, disability, death or prolonged hospital stay for the patient’. 5 The World Alliance for Patient Safety of the World Health Organization 2007, proposes an international classification for patient safety in which a patient incident is defined as ‘an event or circumstance which could have resulted, or did result, in unnecessary harm to a patient’ and an adverse event as ‘an incident which results in harm to a patient’. 6 For the purposes of this review I will refer to adverse events as a general term for the clinical incidents that occur to patients.
A confidential web-based reporting system connecting each reporting hospital to the CIS (STARSWeb), was established in 2004. Public hospitals and health services in the Republic of Ireland, which are managed by the HSE, are indemnified by the CIS. The health services covered by the CIS have a statutory obligation or mandatory requirement to notify the CIS of adverse events as soon as possible. There are no sanctions for a failure to report an adverse event.
There are a number of guidelines published to guide medical professionals on how best to deal with adverse events. The principles of the Hippocratic Oath are often referred to as the first statement of a moral code of conduct for the medical profession. 7 These principles complement those required of all doctors by the Irish Medical Council (IMC) in terms of patient care and patient information in relation to the reporting of adverse events. 8 The Irish Commission on Patient Safety and Quality Assurance recommend that professional regulatory bodies should include mandatory reporting within their codes of professional practice. 9 The Irish Government has also passed two Health Acts in 2007 10,11 which will offer medical practitioners protection in terms of ‘whistle-blowing’ and oblige medical practitioners to participate in peer review and clinical audit.
The World Health Organization (WHO) has also focused on the area of surgical safety in recent years. It states that the main purpose of adverse event reporting systems is to learn from experience. The WHO also believe that individuals who report incidents must not be punished or suffer other consequences. 6 The most recent initiative aimed at addressing surgical safety commenced in January 2007 with the WHO's Second Global Patient Safety Challenge. 12 Key objectives outlined by the WHO now form the basis of a one-page Surgical Safety Checklist (Figure 1) used by healthcare workers to ensure that safety standards are met. The Checklist has been shown to benefit patients in terms of reduced morbidity and mortality. 13
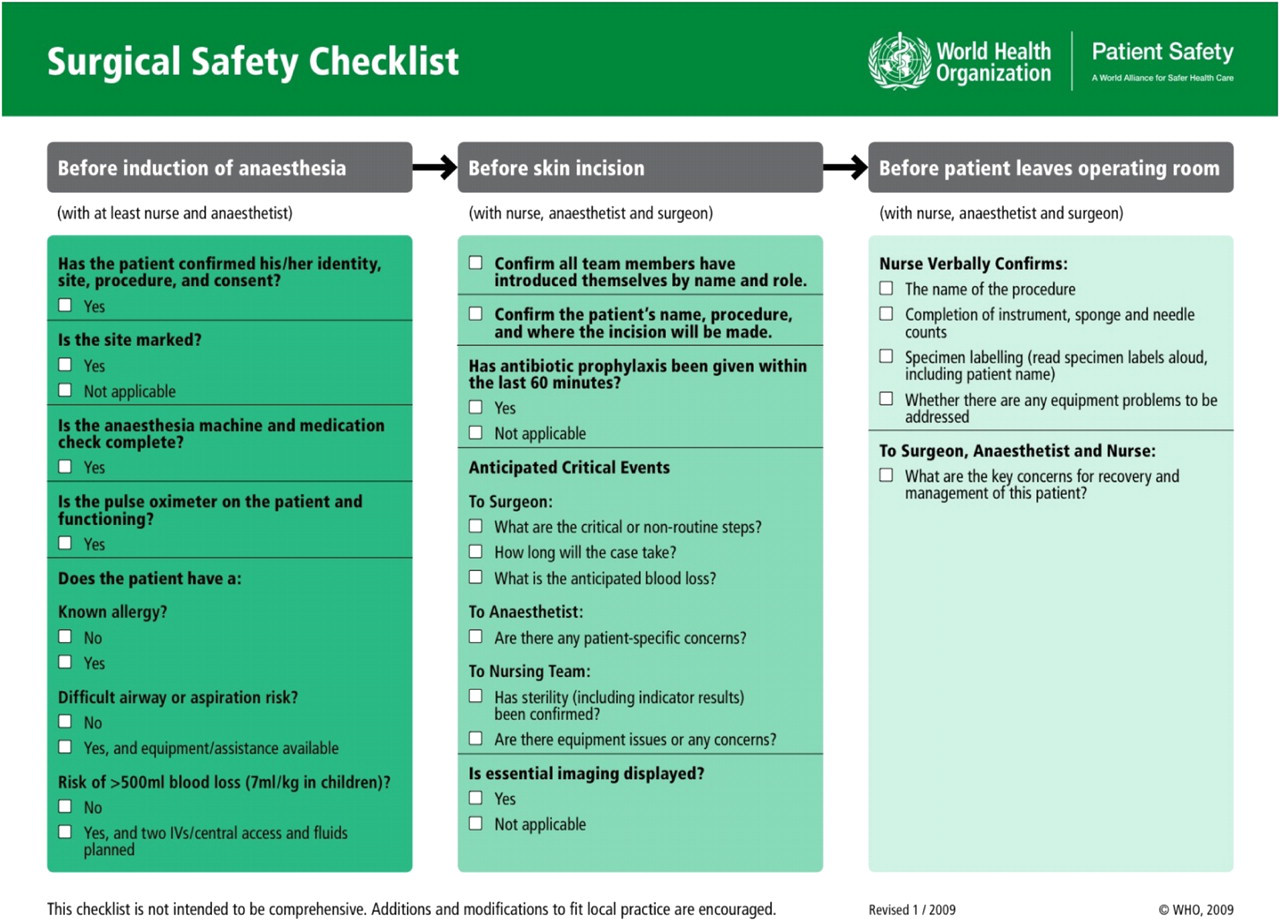
WHO Surgical Safety Checklist (in colour online)
Professional development and training of doctors does encourage open disclosure of adverse events, however, the published literature on the topic indicates that disclosure does not always take place. Wu et al. found that only 24% of house officers who had been involved in a mistake reported discussing the mistake with the patient. 14 Gallagher et al. suggest that patients do not wish to know about error as it may diminish the trust they have in their doctor. 15 Leape et al. highlight fear and a lack of belief that reporting actually results in improvement as the principle reasons for non-reporting of incidents within healthcare organizations. 3 It has also been found that poor disclosure policies in US hospitals are primarily related to fear of malpractice litigation. 16 Many doctors feel that they are poorly trained in how to deal with adverse errors and cite this as a reason for not disclosing errors to patients. 17 A focus on the individual in a blame and shame culture leads to the concealment of errors. 18 Quick et al. argue that the traditional secretive culture within medicine means that errors remain hidden. The author advocates that the investigation of error should be broadened from the narrow focus of the individual, towards the more complex workings of institutions, environments and cultures. 19
It has been estimated that under-reporting of adverse errors can range anywhere from 50–96% annually. 18 In 2006 Freestone claimed that under-reporting is still the rule rather than the exception and that reliable critical incident reporting is therefore hard to achieve. 20 Evans et al. highlight the fact that clinicians are not motivated to report if they believe that there is insufficient feedback on these reports. 21 The authors are critical of lengthy feedback forms and also maintain that many doctors believe that some incidents are too trivial to report.
Study aims and objectives
The aims of this study are three-fold. The primary aim is to identify the current overall trends in Ireland, with regard to reporting adverse events in the surgical specialties. Secondly I will identify the conditions surrounding an adverse error which have made it more likely for an adverse event to occur. Thirdly I will examine the factors which are associated with medicolegal claims processed by the CIS. The relevance of this approach to the study is to create awareness for surgical teams of the conditions more likely to create an adverse event in their service. This awareness can create caution and and a subsequent improvement in patient safety.
Methods
This study is a retrospective review of information in relation to a cohort of patients who have had an adverse event reported regarding their care while a surgical patient in Ireland. The timeframe under review in this study is from 1 January 2004 to 30 May 2010. The sample size in this study is 42,094 cases of adverse events that were reported to the CIS during this period. Data in relation to 2010 (1 January 2010 and 31 May 2010) were excluded during the analysis of which month adverse event were most frequently reported. The data were reviewed using the Stata statistics and Microsoft Excel programmes. There are seven different endpoints outlined in Table 1, which form the basis for further analysis.
Table of endpoints
The final part of my analysis involves assessing the medicolegal claims processed by the CIS. This analysis is done using the endpoints listed in Table 1.
Results
The results provided here are based on 42,094 adverse events that occurred in Irish Surgical Specialties reported to the CIS between the dates 1 January 2004 and 31 May 2010.
General surgery accounts for 46% of cases and orthopaedic surgery accounts for 27% of all cases (Table 2). Figure 2 illustrates that there has been a year-on-year increase in the number of adverse events reported to the CIS. The full data on 2010 was not available at time of study.

Annual incidence of adverse events (in colour online)
Incidence of adverse events in surgery
Figure 3 illustrates the breakdown of incident type that occurs during the timeframe of reporting. Is it clear from the graph that the category of slips/trips/falls is a significant incident type reported in these data. It accounts for 32% of all cases reported. The next highest reported incident type was medication error, with perioperative incidents the third highest.
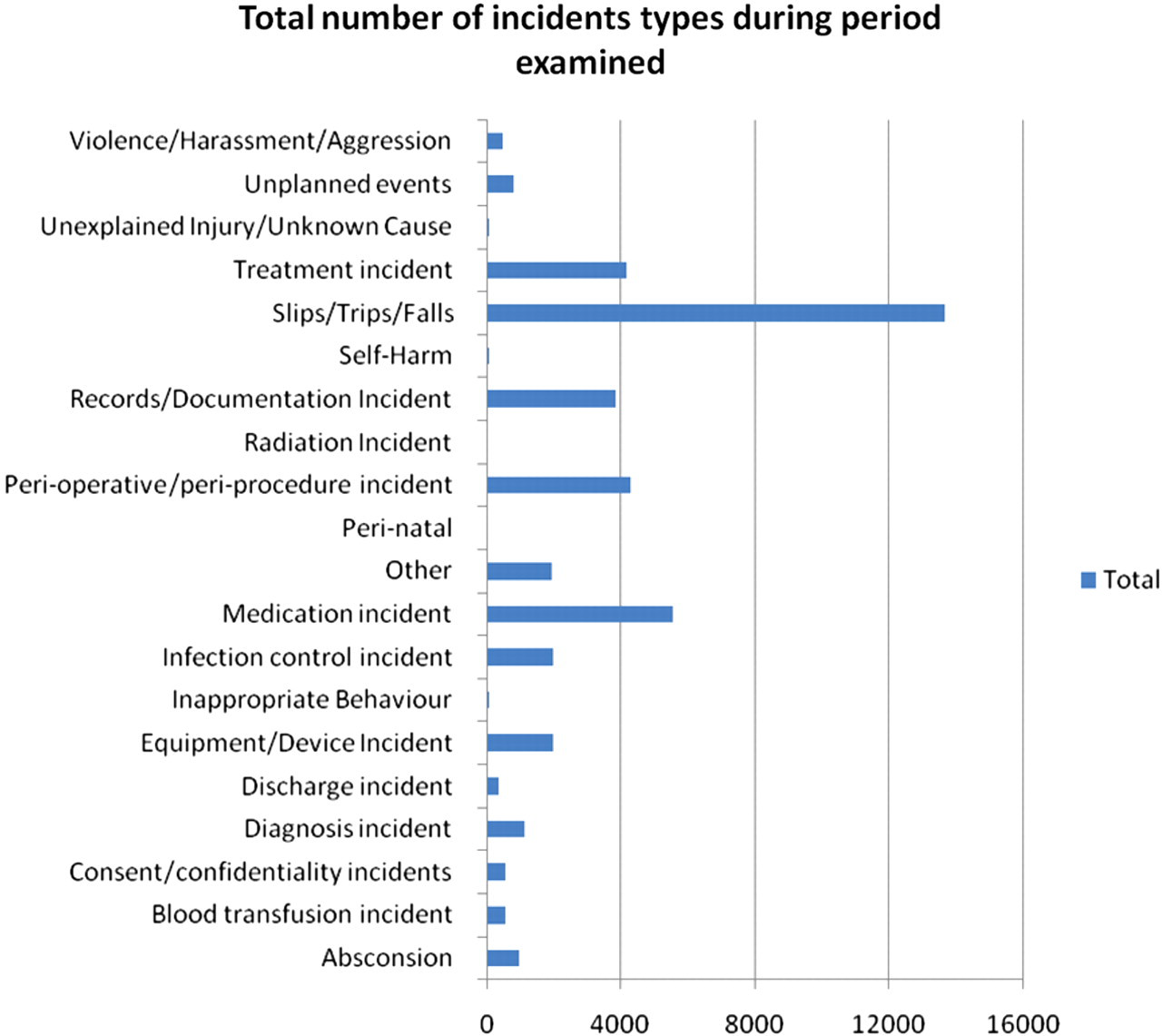
Incident type of adverse event (in colour online)
Nursing/midwifery reported 85% of all adverse events during the study period. Medical staff, which would include surgeons, account for only 4% of the total. Table 3 outlines the most common type of outcome listed for all the adverse events reported. The most common outcome type is ‘No apparent injury/reaction’ (80%).
Outcome of adverse events
Twenty-four separate hourly bands are available for time description as outlined in Figure 4. The time of occurrence of each adverse event has not been routinely entered. A total of 28,996 time of adverse events has been included, which is 69% of all adverse events. There is an increase noted in the morning time from 08:00 and which reduces in time from 14:00. The earliest time for adverse events being reported is 05:00.
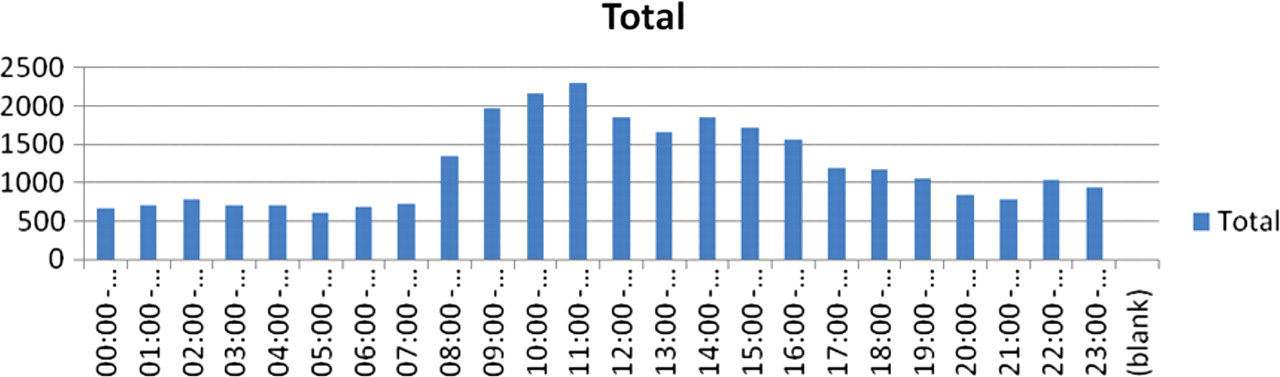
Time of occurrence of adverse event (in colour online)
When the time of ocurrence of slips/trips/falls is compared to perioperative/periprocedure incidents, there is an increase of both in the morning from 08:00 (Figure 5). The amount of slips/trips/falls stays at a higher level for the rest of day. There is drop in the slips/trips/falls at 13:00. The levels of perioperative/periprocedure reduce in number from 16:00 onwards.
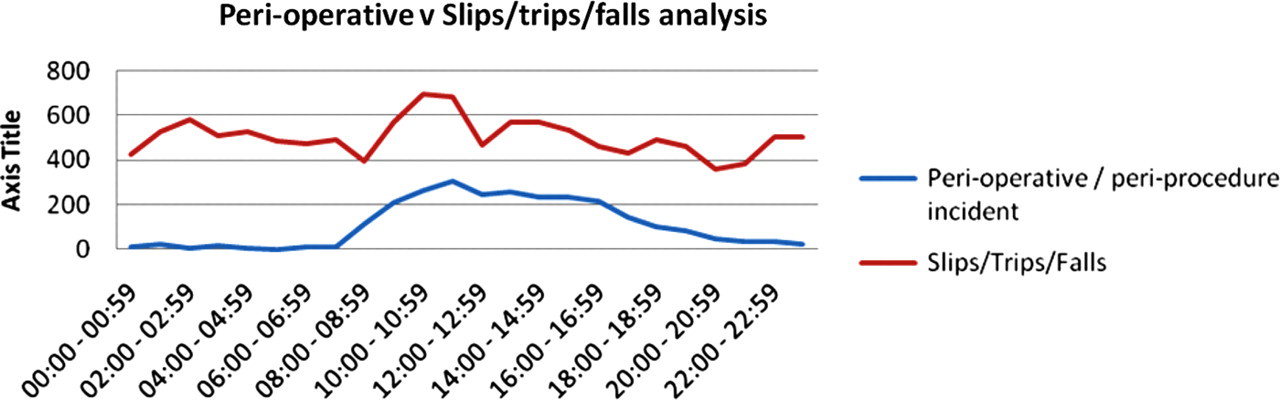
Time of occurrence of perioperative adverse events in comparison to time of occurrence of slips/trips/falls (in colour online)
A date was entered correctly for all the adverse events reported to the CIS during this period (Figure 6). The highest frequency of adverse events is reported in October. There is also a small increase noted in the month of July relative to June in relation to adverse events.
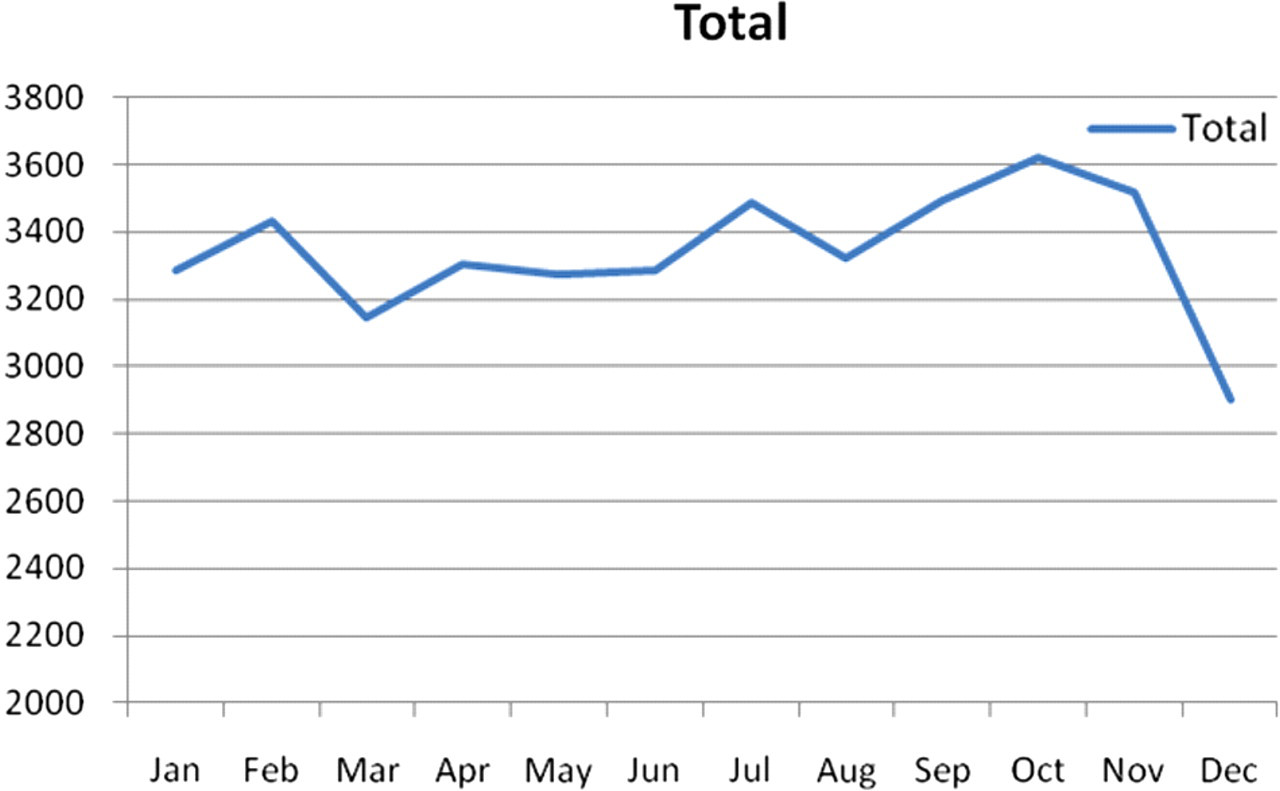
Month of occurrence of adverse events (in colour online)
Closed claims managed by the CIS between January 2004 and May 2010
The CIS closed 478 claims between January 2004 and May 2010. Table 4 indicates the number of claims made per specialty.
Closed claims by surgical specialty
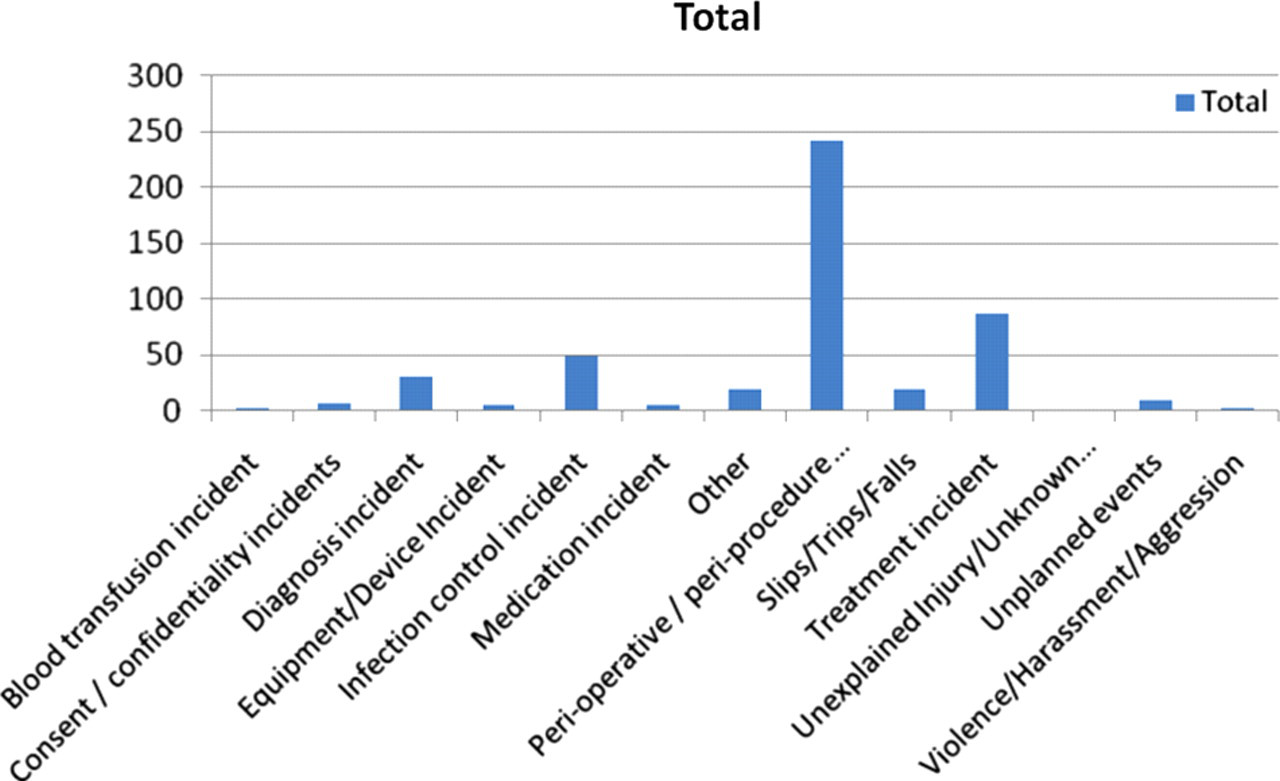
The most common incident type to result in a closed claim was the perioperative/periprocedure incident, which accounted for 50% (242) of all cases as outlined in Figure 7.
Closed claim by event type (in colour online)
The most common specific incident type reported (48%) was unexpected complications following the operation, followed by unexpected complications during the operation (10%). The full list of incidents can be seen in Table 5.
Closed claims and specific incident type
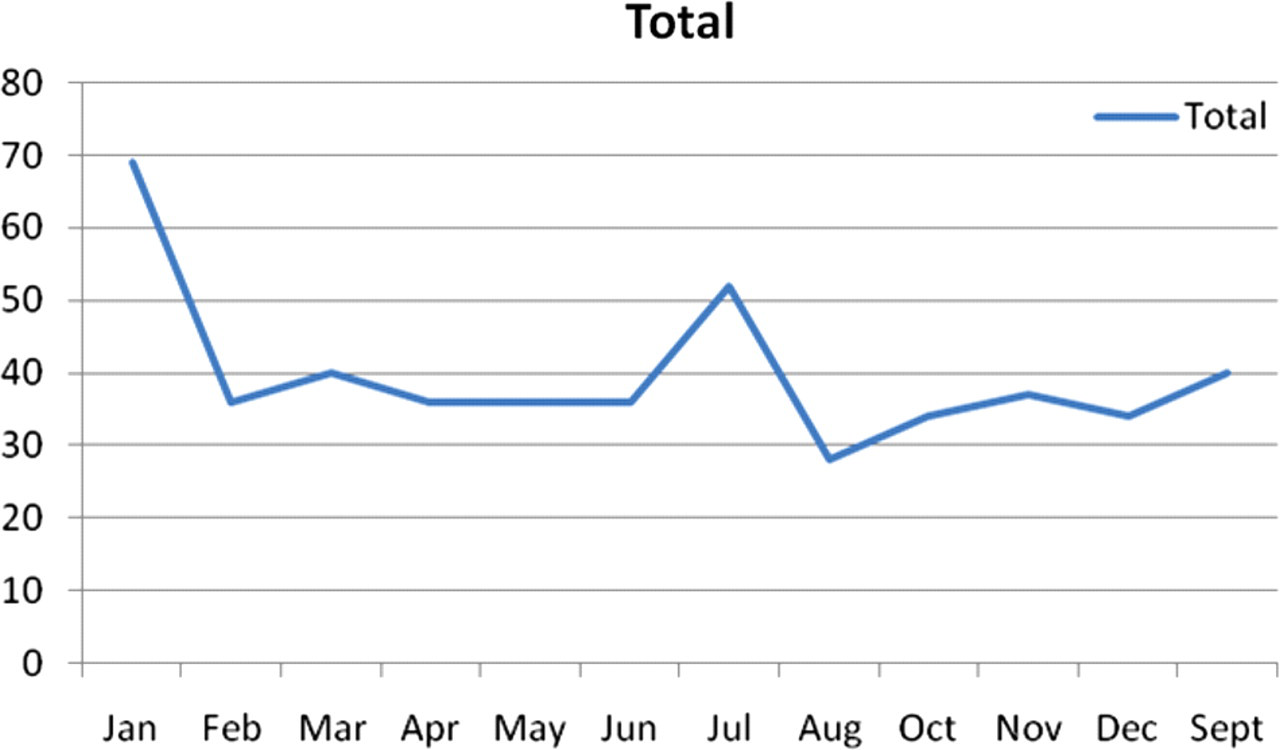
The highest month of occurrence for incidents which results in closed claims was in January (Figure 8). Sixty-nine claims occurred in this month which is 14% of all claims. There is a significant increase in the number of closed claims related to the month of July, the second highest month for recorded claims. It accounts for 10% of all closed claims.
Closed claims and month of occurrence (in colour online)
Discussion
The two most common surgical specialities that reported adverse events were orthopaedic surgery and general surgery (73% of all cases). There has been an increase in year-on-year in terms of adverse events that have been reported to the CIS.
The data discussed in this study relate only to information provided to by the CIS. No information relating to events that may occur for example in hospitals in the private sector is included. The private medical sector in Ireland, in particular in surgery, is expanding. Therefore there is potentially a significant amount of data that is not available for this study.
The data indicate that slips/trips/falls are a common adverse event occurring in surgical patients. This is common among other branches of medicine where up to one-third of cases are also in the category of slips/trips/falls. 22,23 This category of incident is unlikely to be directly related to the surgical care provided to the patient. In a review of slips/trips/falls in relation to showers and showering performed by the CIS in May 2010, is it interesting to note that orthopaedic surgery is the sixth most common subspecialty in which these falls occur and the highest rank surgical specialty. 24
Nursing staff/midwifery reported 85% of events while medical staff, which would include surgeons, account for only 4% of the total. This figure of 4% is extremely disappointing but is not unusual in terms of the international literature. 20 There are obviously a number of factors that influence the level of reporting among medical staff. 19 Nursing staff have adopted a different attitude towards reporting error. The low figure of reporting of adverse events among medical staff is concerning in particular when the guidelines in relation dealing with error from the RCSI and the IMC are reviewed. 8,12 It is reasonable to suggest, based on the figures from the CIS, that surgical error is not being addressed in an open and transparent way as is hoped for in these guidelines.
The timing of adverse events have been included for review in this study. There is an increase noted in the morning time from 08:00 and which reduces in time from 14:00. The earliest time for adverse events being reported is 05:00. These figures would inidicate that most adverse events take place during daylight hours when most surgery now takes place. Intiatives such as the Safe Surgery Checklist are designed to reduce the number of errors that occur in relation to surgery and have been shown to have beneficial effects. 13 The most common period of the day for a reported adverse event to take place is the morning time rather than the afternoon. It is also noted that slips/trips/falls are more common during daylight hours.
A monthly trend analysis indicates that the highest frequency of adverse events is reported in October. There is also a small increase noted in the month of July in comparison to June, in relation to adverse events. The months of January and July are interesting during the clinical year. There is a significant amount of staff turnover between and within hospitals during these months. Significant changes in staff employed in surgical teams can also be seen in hospitals during October but the numbers are smaller. There is a high drop-off in the figures in relation to the month of December. This may be explained by reduced surgical output due to annual leave ward and theatre closures.
General surgery accounts for 31% and orthopaedic surgery accounts for 25% of all claims closed by the CIS. The percentage of adverse events reported, however, for each specialty was general surgery with 46% of cases and orthopaedic surgery accounting for 27% of all cases. There is a significant drop of 15% in comparative terms for adverse events and closed claims in general surgery. The most common incident type which resulted in a closed claim was the perioperative/periprocedure incident. This incident type accounted for 50% (242) of all cases. A detailed analysis of this figure reveals that the most common specific incident type reported (48%) was unexpected complications following the operation, followed by unexpected complications during the operation (10%).
The highest month of occurrence for incidents which resulted in closed claims was in January. Sixty-nine claims occurred in this month, which is 14% of all claims. The second highest month for recorded claims was July, which accounts for 10% of all closed claims. The months of January and July are noted previously to be months which reported high incidents of adverse event reporting. These months are also noted to be months of high staff turnover in hospitals.
Conclusion
A high number of adverse events (42,094) were reported to the CIS during the period of this study. The number of claims closed during this period was much less at 478. The figure of 42,094 has been used as the total figure of adverse events during this period but the published literature would argue that adverse events and critical incidents, in general, are significantly under-reported. 18 The reporting of adverse events is evident across a range of surgical specialties. The high output specialties of general and orthopaedic surgery account for the highest number of both events and claims. Surgeons in Ireland do not routinely report error as part of a formal reporting system. In order for the surgical community to learn from its mistakes it is imperative that we have a robust reporting structure in place. This study indicates that new initiatives need to be put in place to highlight the importance of dealing with error among surgeons. This is particularly important when considered against the backdrop of new ethical and legislative requirements for surgeons. Surgeons must also be assisted in dealing with the personal factors that prevent them from reporting error. Training programmes must continue to incorporate modules in relation to adverse events in surgery.