
Abstract
This paper discusses how we have improved patient handover by implementing an electronic system for weekend handover. We discuss the process of changing handover methods and the results of an audit comparing our old paper based book versus our new ‘e-handover’ system.
Introduction
The European Working Time Directive (EWTD) has led to the introduction of new shift systems as junior doctors' hours are reduced to 48 hours a week. This has reduced the continuity of care of patients who will see multiple doctors during their admission. For example, one study demonstrated that medical patients see an average of six doctors during their stay. 1 There is, therefore, concern that the reduced continuity of care associated with the new shift systems may lead to a reduction in the quality of care for patients. Thus handover has become a vital tool in the attempt to preserve continuity of care. However, recent studies suggest that the quality of handover is usually poor; it is rarely standardized and there is little teaching on handover for junior doctors. 2,3 Poor handover has led to medical errors in areas including prescribing and follow-up. 4–6 Inadequate handover can also result in increased laboratory testing of patients and longer patient stays. 7 A study performed in the USA showed that a lack of information at handover including information on clinical conditions and tasks required resulted in delays in diagnosis for patients and adverse clinical events including an intensive care admission. 3
It has been suggested that by formalizing the structure of handover the quality of the information handed over improves. 8 A study looking at types of handover demonstrated that only 2.5% of information was retained using a verbal handover. However, this improved to 85.5% with note taking and 99% with a formal printed handover. 9 These results are supported by other studies that show increased data transfer using a structured handover. 10,11
The World Health Organization is among several bodies which have supported the use of structured handover on the basis of evidence such as cited above. It has included effective handover as one of its ‘Nine patient safety solutions’. 12 The BMA has also produced guidance (safe handover: safe patients) which promotes the use of a structured handover including the use of IT tools. 13 The Royal College of Physicians Health Informatics Unit (HIU) has developed certain standards for the structure and content of handover including handover out of hours. 14
New Cross Hospital in Wolverhampton is a large district general hospital in the Black Country with a 700-bed capacity. The weekend medical handover had previously consisted of medical teams from each of 13 wards inserting handwritten entries in a dedicated book for the on-call team to review at the weekend. This was a simple blank notebook in which junior medical staff freely entered patient information in an often unstructured manner. The quality of this written handover information varied and, in particular, many junior doctors felt the entries lacked important patient information. This raised concerns regarding the effectiveness and, therefore, safety of this system of handover.
This paper describes our attempt to improve medical handover through the involvement of our medical colleagues in the use of a specifically designed electronic platform. Audit was performed to assess the benefits of the new electronic handover system.
The e-handover tool
A structured electronic handover system was designed and developed by a consultant physician in conjunction with the IT department of New Cross Hospital. Termed the ‘e-handover’ it is a secure, password protected system available on the trust intranet. This database is viewed as a list of patients with their relevant demographic details that also provides direct links to their medical conditions and required tasks. The urgency of each task and the grade of doctor needed for its completion are also recorded. One particularly useful feature is the linking of this database with the hospital patient administration system which allows for the real-time location of patients, some of whom may be transferred up to three times within the first 24 hours.
When logging on to the e-handover system the patient list can be filtered according to the following (Figure 1):
Date Status of task Task type Ward (patient location) Grade of doctor required to do task Specialty
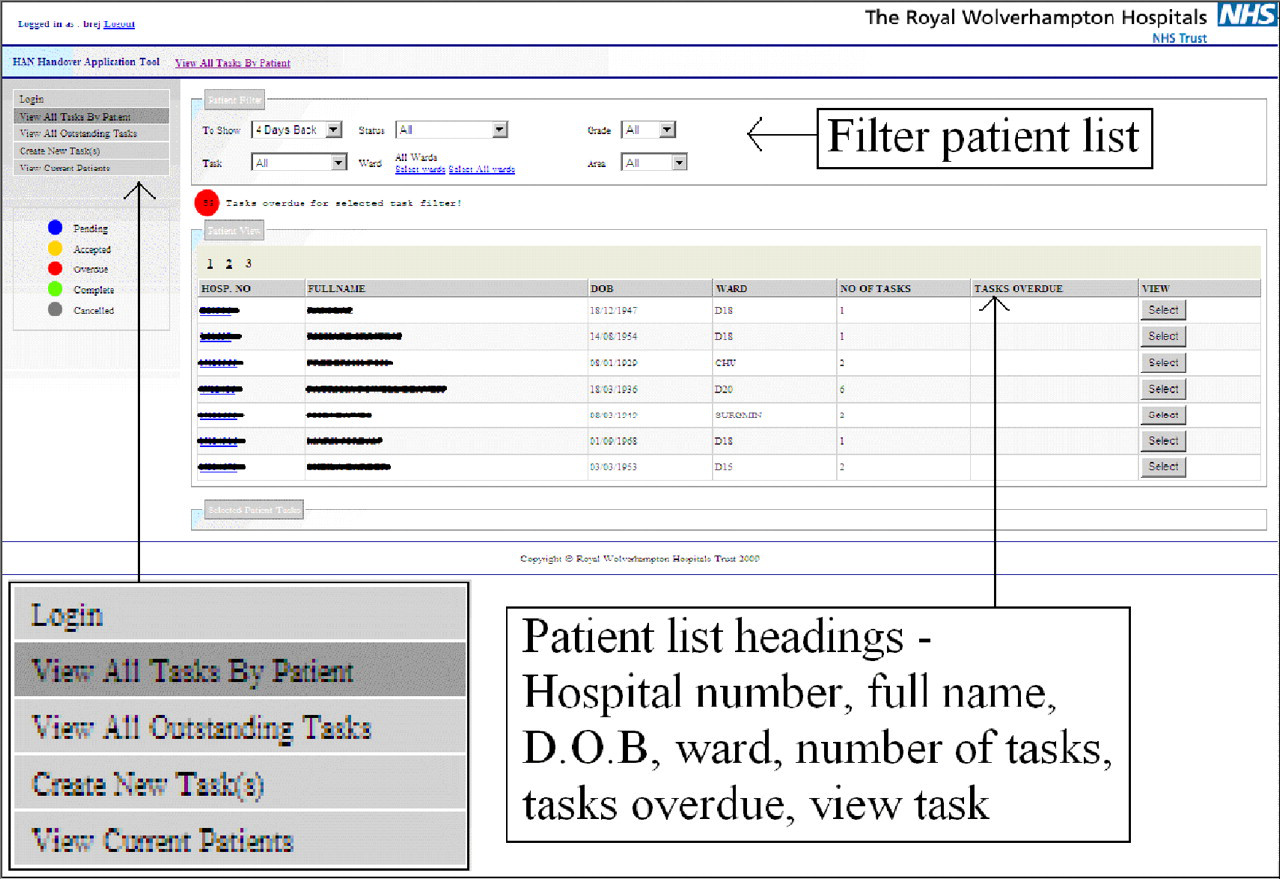
e-handover screen shot – filtering patient list (in colour online)
After searching for a patient using their hospital number or name, a new task can be created by filling in appropriate information (Figure 2). Once uploaded the status of the task can then be updated by the on-call team (Figure 3).

e-handover screen shot – uploading task

e-handover screen shot – task uploaded (in colour online)
The e-handover enables the automatic recording of the details of the doctors accessing the system thus providing information vital to the governance of handover.
Colleague involvement
We identified a need to change the process of handover and doing this required a change of culture. Our challenge was to embed the new electronic handover system into the routine clinical practice of the junior medical staff. Initial informal discussions with junior medical colleagues made us rapidly realize that their adoption of a new system for handover would have its difficulties. These were primarily related to a reluctance to change per se. Changing established behavior of any kind is challenging and, therefore, we utilized the NICE guidance on ‘how to change practice’ to give us a varied approach. 17
As acceptance and beliefs of individuals greatly affects their ability to adopt new behaviours, 17 we used a questionnaire to explore their beliefs and attitudes towards handover. The questionnaire consisted of six statements to which the respondents had to circle an option of strongly disagree, disagree, indifferent, agree, or strongly agree. Example questions included ‘The handover book is an adequate method of weekend handover’, ‘When handing over patients for the weekend I am confident tasks will be done’. Opinion was mixed with 53.3% feeling that the handover book was an adequate method for weekend handover. However, paradoxically, the majority of respondents felt that the quantity of information given about the patients was inadequate. The questionnaire confirmed our initial finding that there was an anxiety among the junior doctors as to whether an electronic system would work and whether it would be used. Despite the reservations and reluctance of some of our colleagues, the lack of adequate handover information, which was apparent to the majority, enabled us to persuade them to agree to training in the use of the e-handover. Formal lunchtime training sessions were delivered and for those doctors who could not attend these, one to one sessions were provided. Once we were happy that everybody had been trained and had the skills to use the system, it was implemented. However, it was necessary to remove the handover book to enforce the use of e-handover as a significant minority of trained junior medical staff persisted in using the paper-based method.
As a result of the resistance to our proposed change by a minority of our colleagues we felt it necessary to improve the awareness and knowledge of why and how handover needed to change. We needed to clearly communicate the proposed changes and the reasons underlying these as many of our colleagues may not have felt improvement was needed. Thus, we introduced our plan to consultants and junior medical staff at a lunchtime educational meeting. This enabled us to gain feedback from them regarding our strategy and how changes should be made. We felt it was important to gain consultant involvement with the changes we were making as leading from the ‘top down’ would highlight the importance of patient handover to junior doctors.
Once the system was established we included a section on patient handover into the programme for junior doctor induction. This involved a visual demonstration as well as printed educational material for reference.
Audit of handover: paper based system versus e-handover system
We performed an audit comparing the paper based handover book versus the e-handover system to determine whether the process of handover had been improved. The Health Informatics Unit (HIU) of the Royal College of Physicians has established national standards for the structure and content of handover documentation. 14 Using the headings advised for weekend handover, we retrospectively audited the content of 53 consecutive entries from our paper-based handover book over a fixed period of three weekends. Following the implementation of our e-handover system we audited 50 electronic handover entries. In addition we looked at whether the seniority of the doctor required to do the task was specified. The results were then analysed using a Fisher's exact test.
Audit results
The e-handover system automatically logs the time and date of the handover as well as all patient details therefore, 100% of this information was recorded. This was significantly better than the information documented in the paper book in terms of time, date of birth and hospital number (Table 1). Other areas of information that were significantly better recorded in the e-handover system included aims and limitations of treatment (86% vs. 28%), the name of the doctor writing handover (100% vs. 0%) and the seniority of the doctor required to perform the task (100% vs. 43%). No significant difference was found between the two handover systems in recording responsible consultant, diagnosis, discharge over the weekend, reason for handover, tasks to be done and the bleep number of the doctor writing handover. Responsible consultant was recorded poorly in both handover systems (2% in the paper handover and none in e-handover). Discharge over the weekend was only recorded in 2% of both handover systems. Also, neither handover system recorded doctors' bleep numbers.
Audit results
Conclusions
Principal finding
The audit confirmed that the paper-based handover book was an inadequate method for handover as key information was often omitted. It was our experience that by implementing an electronic handover system to facilitate our weekend handover, that we significantly improved the amount of information passed to the on-call teams. Our results support the findings of other studies suggesting that electronic handover may provide better continuity of care than paper-based handover. 15,16
Developing an electronic handover system
The involvement of clinicians is essential to developing a sustainable electronic handover system. 18 During the initial months following implementation we continued to seek feedback to find ways to improve the system. Feedback was gained via our Junior Doctors Forum which encouraged people to report any problems or concerns. Subtle changes to the system were made to deal with the issues that were raised. For example we realized that many of the tasks were not being updated on the system as having being completed. To solve this problem a reminder message was added which appeared when users logged on to the system.
By looking at the standardized headings advised by the Royal College of Physicians we have also identified ways in which our e-handover system could be improved further. For example, including mandatory fields for ‘Responsible Consultant’ and ‘Bleep number/Contact details’ which are not currently recorded.
Additional benefits of e-handover
We identified a number of benefits to using an electronic system:
Avoidance of breeches in patient confidentiality caused by lists being lost or left lying around the hospital; Handover ‘moves with the patient’; Litigation and governance – clear demonstration of accountability, archive of evidence of what has been handed over and whether or not the tasks were completed; Avoidance of the problem of illegible handwriting.
Audit limitations
We have identified some potential limitations to our audit. The data was collected over two separate time periods before and after the implementation of the e-handover system. There were, therefore, two separate cohorts of doctors working for the trust at these times which may have biased the results. Results at other times of year and in other trusts may also differ. Part of changing our handover process involved training sessions and presentations to our colleagues. This reinforced the importance of a good quality handover which may have also had an impact on how effectively information was handed over, irrespective of the handover method. We accept that we only analysed a relatively small proportion of patient handover information so these results may not be representative of overall weekend handover.
Summary
Clinician involvement is essential to both the development and implementation of an electronic handover system. Our audit has demonstrated that electronic handover improves the quantity of information passed between on-call medical teams.
Medical information technology is a rapidly developing field and the move to electronic patient records is an inevitable goal. However, having an electronic system does not change the basic concepts of a good patient handover including designated time for a handover meeting within the working day but is a good platform on which to base the information passed between medical professionals. We are now in the process of expanding our e-handover system to incorporate the night and midweek morning handover given its success so far.
We believe that further research and evaluation are needed to establish gold standards of patient handover in the era of the European Working Time Directive and the effectiveness of introducing electronic handover systems.
Footnotes
Acknowledgement
The authors would like to thank David Gray and IT department of New Cross Hospital.