
Abstract
Following a Never Event in our Trust which involved misinterpretation of a radiograph by a junior doctor, we set out to reduce the risk of recurrence by creating Vital Radiology. Vital Radiology is a new scheme designed to teach junior doctors about important radiological diagnoses that, if missed at the bedside, can have devastating consequences for patients. Although in its infancy, the scheme is receiving positive feedback both from the participants and senior clinicians. Ultimately we aim to extend the scheme throughout our trust and beyond, with the intention to improve junior doctors' confidence in interpreting images and, more importantly, to reduce risk to patients.
Background
Radiology plays a critical role in the management of most patients admitted to hospital. Junior doctors are often called upon as the first line, to interpret x-rays that lead to important decisions about patient care. A wrong diagnosis at the bedside can lead to potentially life threatening consequences. A “Never Event” 1 occurred in our hospital involving misinterpretation of a radiograph by a Junior Doctor. Never Events are defined by the National Patient Safety Agency as “serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented”. The purpose of recognising and analysing a “Never Event” is, ultimately, to prevent their reoccurrence and to promote patient safety.
During analysis of this Never Event, it became clear that if one junior doctor could misinterpret an important radiological investigation, it could occur again within the trust. We felt this was an extremely important issue both for Junior Doctors' training and, most importantly, patient safety.
Initially, as a patient safety measure, the response to the event analysis was to ensure that the specific type of radiograph was only interpreted by a specialist trainee level 3 (ST3) doctor or above. Although this appeared a reasonable short term measure, we felt that this did not attempt to solve the underlying problem – that our Junior Doctors may lack skills in interpreting the radiographs they request for their patients. As well as the initial shorter term safety measures and without attaching blame to the individuals concerned, we, as a group of doctors in our Trust, set out to devise a positive solution to the problem by attempting to improve the radiology interpretation skills of our Junior Doctors.
Methods
Developing the teaching material
Lack of Radiology knowledge is a problem that can have an impact on many clinical specialities, and, as such, we felt it should be approached from a multidisciplinary perspective, rather than simply a Radiological one. We set up a committee which consists of three radiology trainees, one consultant radiologist, two foundation programme doctors and one medical registrar. We have also had input from our Director of Medical Education and Medical Director.
We set out to create a teaching programme based on Radiological diagnoses that, if missed, can have devastating consequences for the patient. We selected 11 diagnoses which were based on the Committee's varied clinical experience and diagnoses in the suggested curriculum in “Must See” Diagnoses from the Alliance of Medical Student Educators in Radiology.
2,3
The diagnoses and general themes are also in keeping with the Recommended Framework for Curriculum Design, published by the Education Board of the Faculty of Clinical Radiology.
4
The included diagnoses are:
Pneumothorax; Tension pneumothorax; Pneumonia; Pulmonary oedema; Misplaced lines and tubes; Pneumoperitoneum; Sigmoid volvulus; Small and large bowel obstruction; Surgical emphysema; Cervical spine fracture; Neck of femur fracture.
With the diagnoses determined, we then began to develop the teaching programme. We decided to use case-based teaching, so that the Junior Doctors would approach the radiographs as they might in their clinical practice. The case-based sessions were created in Microsoft PowerPoint with the intention that they could be viewed by the participants online, or delivered as a teaching session. We used several teaching resources whilst developing the session content, including Radiology textbooks, Radiology teaching websites, medical textbooks and relevant journals.
3,5–17
All the images were original radiographs provided and anonymised by our Consultant Radiologist, and all of the online teaching sessions were edited by the Consultant Radiologist before being published on the Mersey School of Radiology Website.
18
Example images from our teaching programme can be seen in Figures 1 (a-f) and 2(a-g).
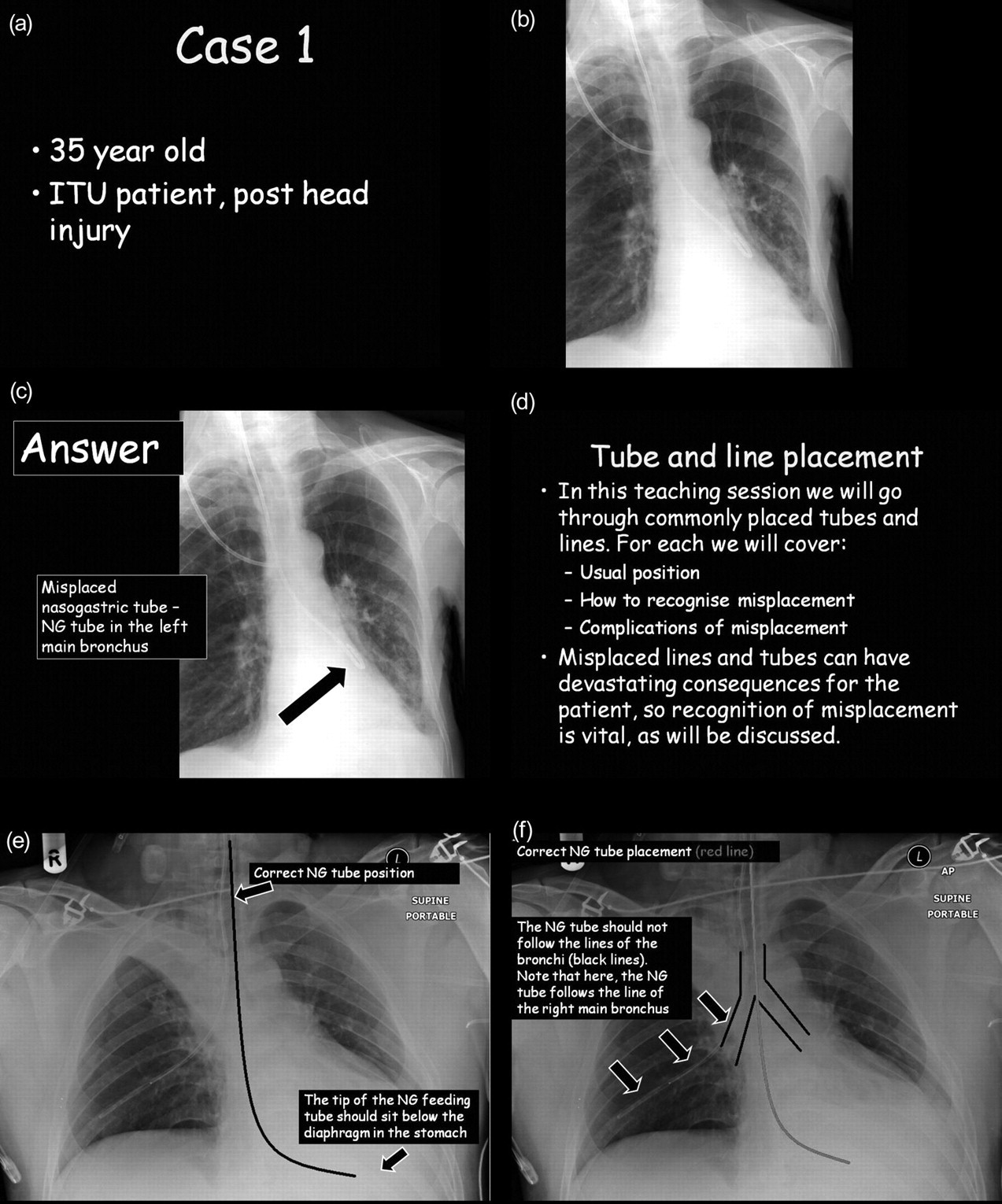
a–f; example images from teaching programme – Misplaced Lines and Tubes
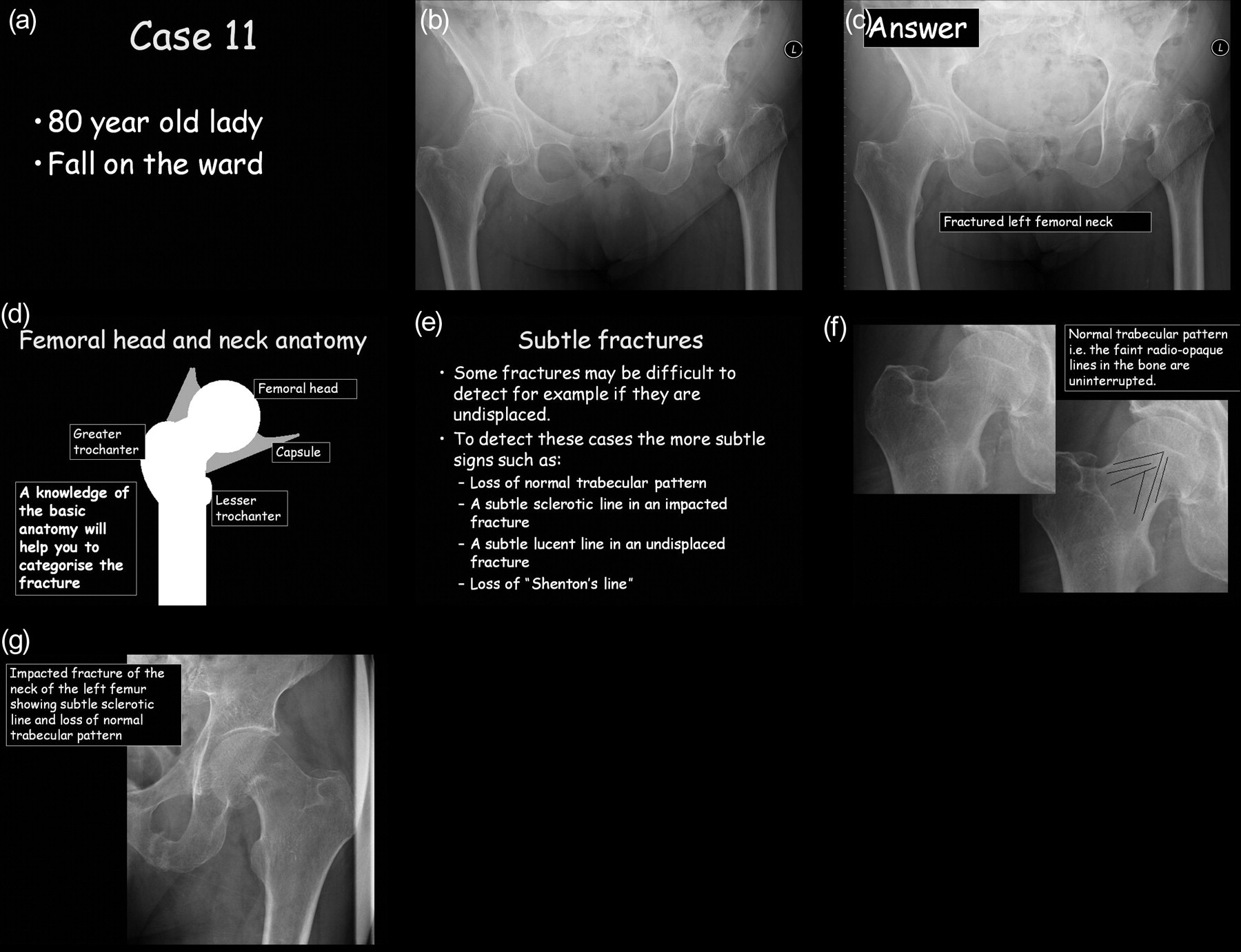
a–g; example images from teaching programme – Fractured Neck of the femur
Developing the examination
In order to prevent further Radiology interpretation incidents, we need to ensure that the doctors not only read the material, but that they understand and retain the knowledge of the important radiological signs they may encounter in their clinical practice. To do this, we also created an accompanying online examination programme.
The online examination was based on all the must see diagnoses, with some “normal” radiographs included. The participants view a radiograph, are given a choice of diagnoses and select the diagnosis they feel is correct. Before introducing the online examination, we asked six independent Junior Doctors to view the programme to ensure that it was user friendly and pitched at the correct level, so that it could be introduced to others.
To complete the programme, the participant reads the teaching material online and then completes the online care-based examination. The pass mark is 100%, as all the diagnoses are critical to patient safety, and failure to recognise any of them could have devastating consequences for the patient in clinical practice.
Our Junior Doctors currently undergo a mandatory Induction Programme when starting their employment in the Trust. As this is an established and well recognised form of training, we are developing our teaching programme to run alongside the current Induction Programme.
We advertised our teaching programme to all the Junior Doctors in our hospital via E-mail and through a Grand Round demonstration. The teaching programme is designed to be used by participants on their own computer, or taught in an interactive teaching session. So far, we have delivered teaching sessions to Foundation Year Doctors, Final Year Medical Students and Core Medical Trainees, all well received.
Expected benefits
Vital Radiology was developed with two aims: to keep Radiology related critical incidents amongst Junior Doctors to a minimum and to ensure all participating doctors feel adequately equipped to recognise the radiological appearances of life threatening pathologies, that may affect their patients.
Ultimately our long term aim is to prevent any further critical incidents related to Radiological interpretation of our “Vital Radiology” diagnoses. This is a difficult outcome to measure in the short term and, as such, we are also looking at short term outcomes to ensure that our programme is beginning to have the desired effect. The evaluation tools we are using to assess the short term outcomes of the scheme are:
An audit of the satisfaction of the participants with the programme – evaluated with a formal online feedback form, which is to be completed after the examination; An online record of participants and their results of the examination. Any doctor who fails the examination will undergo further compulsory training in the Radiology department.
Outcomes
We have initially introduced the scheme to a small group – the Foundation Year doctors in our hospital. Thus far 27 participants have attempted the online examination, with 48% passing the module.
Through our early participant satisfaction audit, we have received positive feedback about the scheme in general and about the teaching material from the Junior Doctors. Our feedback for the teaching sessions and Grand Round presentation has also been very encouraging.
We have, however, received negative feedback that many have had difficulty in accessing and using the examination. This may be partly responsible for the 48% pass-rate, as in order to pass, the user has to be able to use the online examination correctly. It has become apparent that some of our participants were simply not able to use the module properly, which lead to them “failing” the examination. Our next focus of work, therefore, is how to improve the module. We aim to make it more user-friendly and will use a different software programme that can be accessed more easily. Furthermore, we shall increase the size of the radiographs that the participants are asked to interpret during the examination.
There may be additional reasons why our first participants achieved a low pass rate, other than technical difficulties. This may reflect a general lack of radiology training, both at medical school and junior doctor level. One way to improve this, may be to introduce the scheme earlier in training – at medical school – to give the junior doctors a better grounding in Radiology before they embark on their medical school careers.
The future
Using the feedback allows us to make improvements to ensure maximum compliance and satisfaction with the programme. Our aim is that as many Junior Doctors as possible may benefit from the scheme and we plan to have Vital Radiology fully integrated into the Induction Programme in our hospital by August 2011, so that each Junior Doctor starting in the trust will participate.
Furthermore, when fully established in our hospital, we aim to introduce Vital Radiology to other hospitals and medical schools in our region and beyond. We feel this reflects the Royal College of Radiologists' message that, as radiology is such an important part of many patients' healthcare, a good knowledge of radiology is an important skill for today's junior doctors. We recognise that, if this problem can occur in our Trust, it could occur at others and they too could benefit from Vital Radiology.
Conclusions
Critical incidents, such as Never Events, can be devastating for patients, their families and the clinical team involved. Instead of simply attaching blame, the committee in our Trust developed Vital Radiology to make a positive change by educating Junior Doctors about important radiological diagnoses. Although in its infancy, Vital Radiology is so far well received and we are learning from any negative feedback to make continuous improvements to the scheme.
We hope our experience will demonstrate that positive improvements can be made as a result of tragic incidents and that junior doctors welcome additional training in radiology. Ultimately we aim to involve all Junior Doctors in our region in this scheme, to improve their knowledge and confidence in Radiology and, most importantly, to improve patient safety.