
Abstract
In the current era of consumerism, patient assessments of care are increasingly being considered an important dimension of quality of care. Good communication with patient or relatives is an important element in General Medical Council's (GMC) guidance on ‘Good medical practice’. Providing proper parent communication may help in improving parental satisfaction with overall care provided in the neonatal unit.
The Patient Experience Tracker (PET) device is a small wireless electronic handset used to gather real time report on patient experience. The neonatal unit PET survey was started after discussion and agreement with all departmental staff. Initial resistances by some staff overcome by open and honest discussion. A good uptake and accurate response depends on the information provided to parents and family about the PET device and survey. The questions should be appropriate to the department conducting the PET survey. Staff should be prepared to respond to the PET survey findings to improve patient satisfaction and thereby patient care. Ongoing support from Hospital Management is essential to ensure the information is disseminated in a constructive manner to all concerned and appropriate actions are taken to improve overall patient experience. The PET system has the flexibility to decide on questions, and more importantly to track performance and improvement progress.
Introduction
Over eighty years ago, Peabody reported that ‘the secret of the care of the patient is in the caring of the patient’. 1 In neonatal units (NNU), there is promising evidence that improved communication and involvement of parents in the care of babies is of benefit and welcomed by parents. It promotes positive parent-child interaction and wellbeing. 2 We have shown previously that providing proper communication may help in improving parental satisfaction with overall care. 3 Regrettably, on occasions, health care professionals fail to communicate effectively with patients and parents of children admitted to hospital. 4 Poor communication results in patient dissatisfaction, increased complaints and increased litigation. 5 Patients' views and satisfaction closely relate to the quality of care provided and are key features of Lord Darzi's report on ‘Our NHS Our Future’ and are amongst the indicators in commissioning for quality and innovation (CQUIN) payment framework. 6
Trust context
At the Homerton University Hospital NHS Foundation Trust we have struggled to obtain measureable feedback from our patients. Response rates to national in-patient surveys had consistently been amongst the lowest in the country. We believe one reason is that the national survey is 80 questions long, postal and only in English. We knew from local demographic reports that our communities felt ‘over surveyed’ so motivation to complete surveys was likely to be low. After exploring various options, the Trust chose to use the Dr. Foster Patient Experience Tracker system. This allowed us to decide which questions we wanted to focus on; but more importantly to relate performance and progress to specific teams and services, as each device was unique to a particular team. Therefore, staff knew that feedback represented the experience of patients within their service. Such data gave the Trust the ability to focus developments and to track and monitor progress.
Neonatal Unit
The NNU is a highly stressful environment, which can be a frightening and alien place for families, with equipment that frequently alarms and with professionals using a completely new language. It deals with extremely sick babies, such as those born prematurely from 23 weeks gestation, weighing as little as 500 g, who require full intensive care followed by a prolonged period of high dependency and special care (6 months or longer in some cases). Some babies born at term in poor condition also require intensive care, an even more shocking and upsetting time for parents as it is so unexpected.
The NNU also provide full palliative care support for babies and their families when a decision is made to withhold or withdraw life sustaining treatment, when continuing intensive care has no purpose or is leading to unbearable suffering. 7-8
Some babies are also admitted for a brief period or with minor problems, while; as a tertiary centre, Homerton provide intensive care support to babies transferred (in-utero or ex-utero) from neighboring districts, who will be transferred back to their local hospitals once they are stable. This, too, creates further anxiety to parents.
Patient Experience Tracker (PET) Device and Survey
The Patient Experience Tracker (PET) device (Figure 1) is a small wireless electronic handset used to gather information from patients, using a live interactive analysis, as described by Foster et al. 9

Patient Experience Tracker (PET) Device
The PET Survey is both a quality improvement and performance management tool. It is one way in which the Trust can encourage patients to be more actively engaged in their healthcare. Clinicians and managers identified key issues, from which five questions were proposed for patients to answer. The first question ‘Were staff courteous and sensitive to your needs?’ was given the most weight with four possible answers; always, most of the time, sometimes or seldom; while the other questions had yes or no options.
The Neonatal Unit PET Survey
A neonatal consultant (NA), neonatal sister (JB) and the NNU operational manager (JF) were involved at the conception stage of this project. The core neonatal PET Survey team (NA, JB and JF) had initial meetings among themselves and with the Trust lead for PET (JN).
Next the project was discussed with the senior medical and nursing team, followed by further discussions with junior nursing and medical staff, ward clerks, health care assistants, housekeepers and others through meetings and emails. The neonatal staff unanimously agreed to adopt the PET survey, which was also approved by the Trust lead for PET and corporate team.
Preparing questions to be asked
We decided to include five questions, in line with the rest of the hospital. (Table 1).
Questions asked with answers to select
PET device – Placement
Parents and relatives were informed about the device and survey by NNU staff as well as through signs and posters. It was initially placed in the parents' waiting room but uptake and entry on the device proved minimal, often with reports that no data were getting to the office or that the device was disabled. We found it was sometimes switched off, on one occasion plucked out at the wall and, worse still, visitors were draping their coats over it. Staff were asked to inform parents about the device and how to use it but; this did not improve matters.
We moved it to a position in front of the nursing desk, where the ward clerk, nurses and doctors frequently congregate. Uptake and inputting dropped further. We were concerned that this might be because parents felt very conspicuous when answering the questions in front of staff, so moved it further down the corridor. This move initially appeared to be working, but subsequqntly data were failing to reach the PET office. On checking the device, it was found to be broken or the electrical lead had been split. We surmised that this occurred as it was plugged-in next to larger equipment such as the X-ray machine, ultrasound scanner and incubators that are in constant use (Figure 2).

PET device surrounded by larger equipment
After repair, we replaced it in the parents' waiting room, with an adjacent. information poster bearing the caption ‘Let us know how we can improve our services’ (Figure 3).
Information on PET device and survey
Information to Parents and staff on NNU PET Survey
The device (Figures 1 and 3), enables parents to express their views of the service provided. The data generated provide instant feedback from patients to help us identify potential improvements and review progress. This feedback, in the form of graphs and pie charts, is sent via email fortnightly, with the information being distributed from the directorate to clinical areas and public display. This feedback is displayed on posters that are updated on a monthly basis, giving the headline messages and scores (Figure 4).
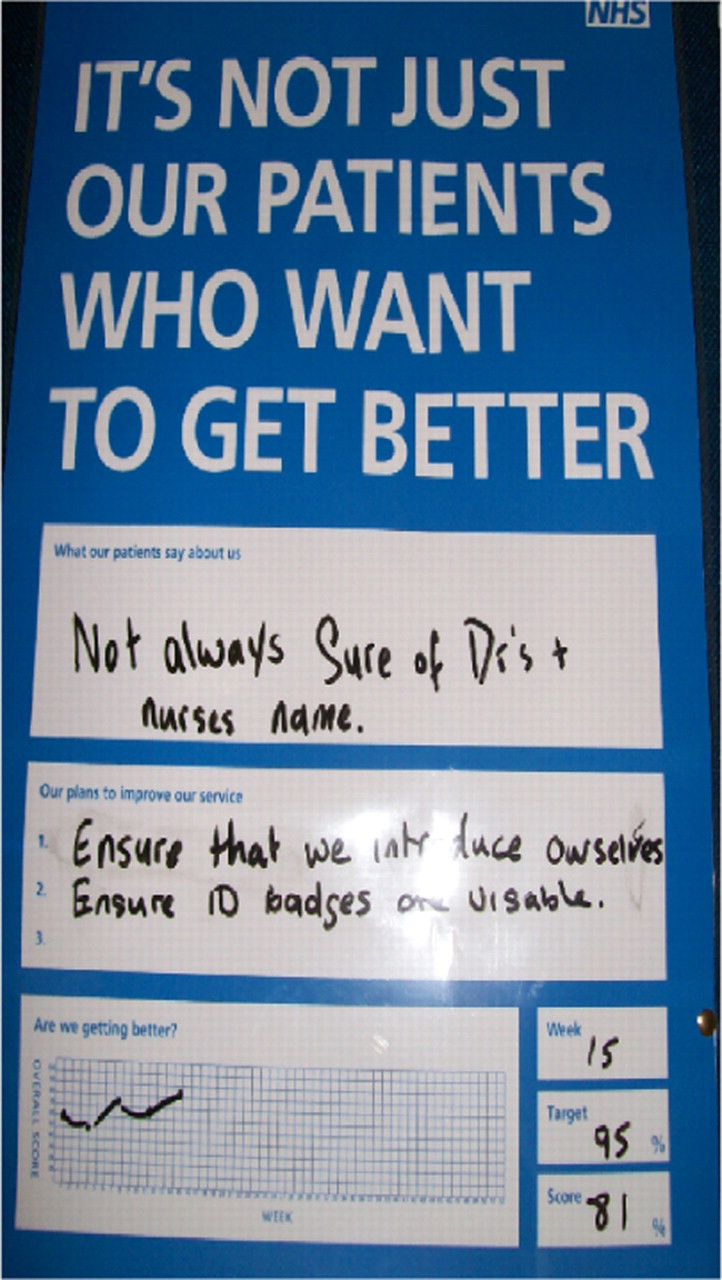
Display of patient feedback and action to improve
Actions to improve overall performance
Despite all our efforts the overall PET score did not improve significantly, remaining below the Trust target of a 95% satisfaction rate.
Again we reminded staff about the Trust's objective of assessing parents' experiences via the PET survey and of achieving a 95% satisfaction rate. The survey results and planned action were discussed regularly at medical and nursing handovers, at multi-disciplinary NNU meetings and at directorate meetings. As these measures did not produce a noticeable change in uptake or result, we addressed this issue with our user group, and concluded that the survey was not asking the right questions. Two main issues were raised concerning staff introducing themselves or greeting parents.
Identifying clinical staff: as the unit was very busy and divided into several rooms of 6 beds with nurses allocated to each room, it was impossible and impractical to expect all staff members to introduce themselves to parents on arrival. The unit has a large team of nurses, junior doctors and housekeepers whose uniforms make it difficult to readily identify clinical staff from support staff. Adding to the uncertainty, consultants, microbiologists, domestics, porters and radiographers may be present, wearing mufti or in their own uniform.
Greeting on entering the unit: Staff opening the door to let parents into the unit, often acknowledge them but then carry on with whatever they were doing. Many of our user group members did not feel this was an adequate greeting. In consequence, we modified the questions to be asked (Table 2).
Questions modified to suit Neonatal Unit
Difficulties faced
Initial resistance from some staff: we needed to ensure the majority of staff were consulted to give them ownership of the change. This prolonged the process but reduced resistance.
Frequent breakdown of the device: often we were unaware of this until 2 weeks later, when informed by the data office.
Lack of an ideal place to keep the device.
Initial failure of live updating of the data: this was, due to interference of the wireless system for live updates. For a few months we manually connected the device to an external telephone line and downloaded data weekly.
Selection of appropriate questions: it was felt that the original questions were too general for the NNU as many members of the team were not easily identified or differentiated by parents.
Conclusion
NNU staff can improve parents' and family experiences by understanding how individuals cope with stress, thus alleviating anxiety and fear. This can only be achieved by actively listening to their experiences and reacting promptly and appropriately.
It is essential that all staff take responsibility and ownership of the PET survey. High uptake and accurate response depends on the information provided to families about the device and survey. The questions should be appropriate to the department conducting the PET survey.
Staff should not feel defensive about the findings but should be prepared to respond by working to increase patient satisfaction, so improving patient care.
Corporate support is essential to ensure information is disseminated in a constructive manner to all concerned.
Footnotes
Acknowledgement
We would like to thank Johnette Brown Neonatal Sister and Jenny Frost – Neonatal Unit Operational Manager, and Neonatal Unit staff, Homerton University Hospital, London for their support to the PET Survey.