
Abstract
Background
Insulin prescribing and administration errors are consistently high with respect to hospital in-patients. There is no straightforward solution to the problem as there are multiple causative factors and system failures. We describe the implementation of a multi-system approach which looks at changes across the board to avoid the risk of serious harm in a teaching hospital setting.
Methods
Organizational level changes included addressing the development of a culture of safety and promoting management buy in. Clinical level changes relate to the labelling and storage of insulin and the provision of accessible information for clinical staff in several different formats. Patient level changes were directed at improving the prescription charts with their own specific insulin section as well as empowering patients to retain the control of their own insulin administration.
Results
Following the initial phase of the project the number of clinical incidents relating to insulin administration and prescribing increased by 18%.
Discussion
The surprising initial outcome was felt to reflect an increased awareness of the issues surrounding insulin problems and the fact that they were previously under-reported. The project has had strong support and good feedback from a wide array of healthcare professionals within the hospital trust. The national diabetes in-patient audit will allow an opportunity for further analysis and a longer time frame for the multi-system changes to bed in.
Introduction
Insulin prescriptions constitute a high number of medication errors within hospitals nationally and have the potential to cause significant adverse effects (according to clinical incident/DATIX data and Diabetes team spot audits).
Research on the safe use of insulin in hospitals has mainly focused on changing protocols and guidelines, but it is important to recognize that a multi-system approach is preferable in line with the NPSA's latest guidance on reducing harm from high risk medications. 1–3
This involves:
- Organizational level changes - Clinical area changes - Patient level changes dosage errors, illegibility, incomplete prescriptions, errors in dosing interval, incorrect insulin formulations, misunderstandings of the mealtime – insulin administration relationship, failure to change insulin prescriptions in the face of severe dietary restrictions eg. NBM, parenteral feeding drug interactions, transcriptions errors.
At the most basic level of prescribing and administration, the commonest causes of insulin drug errors are caused by:
4
As well as the common mistake of ‘U’ being written for units and being mistaken for an extra 0, (12U read as 120) leading to ten times drug errors.
It is therefore sensible to acknowledge that ‘trying harder’, more training, or new protocols alone will not overcome these systems errors. We should recognize that human errors will occur and design around this fact.
Below is a summary of recommendations for changes to clinical and organizational practice which are designed to overcome the perceived, relatively ‘simple’ problem of insulin prescribing and administration errors. They are based on best practice guidelines and the latest literature and have been adapted for in-patient hospital wide use. 5–8
This project was designed to utilize minimal resources and is specifically intended to avoid major changes in practice and the need for extra training of junior doctors, nurses and pharmacists. This also differs from the NHS Institute for Innovation's ‘THINK GLUCOSE’ programme, although we have adopted some of their better ideas.
Evaluation is built in, although it may be difficult to tease apart which of the raft of measures has the most impact. The point ultimately being that we need to do everything we can across the board to increase safety and reduce the high rate of errors associated with this common drug.
Methods
Organizational level changes


Clinical Area level changes
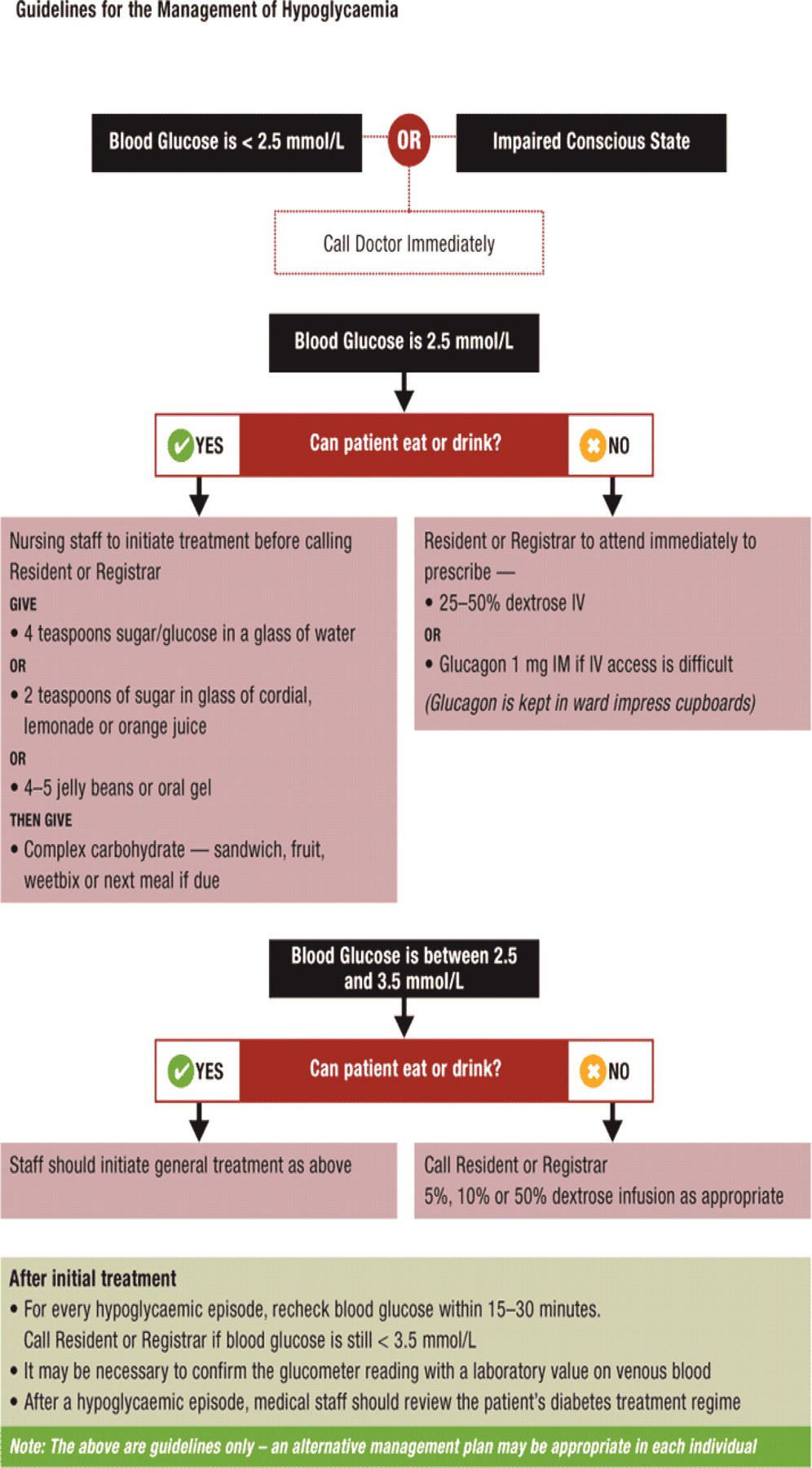
E.g. Treatment of Hypoglycaemia (this can be modified to fulfill local guidance)
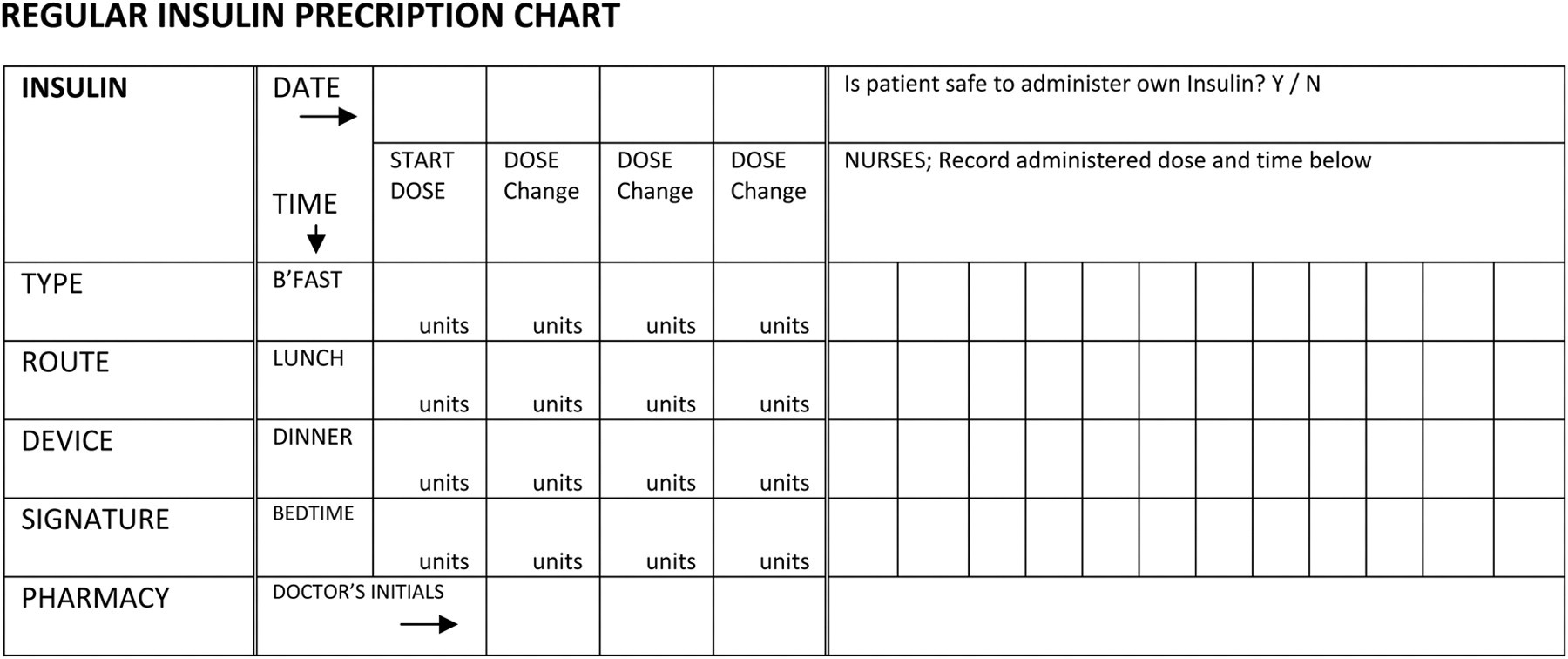
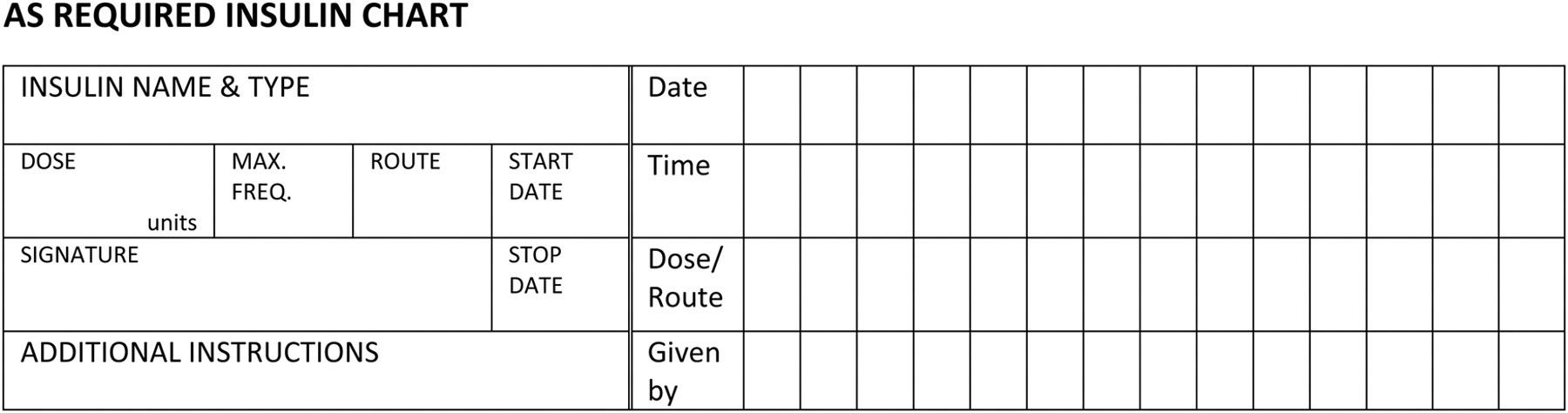
Patient level changes
E.g. New drug chart with specific Insulin section
E.g. Simplified capillary blood glucose monitoring chart.

Capillary blood glucose (CBG) should be monitored pre-meals and 2 hours post meals, at bedtime and 3am
If blood glucose > 10mmol/l give 5% of the total insulin dose prescribed from the previous 24 hours, as fast acting insulin
If blood glucose >15 mmol/l give 10% of the total insulin dose prescribed from the previous 24 hours, as fast acting insulin
If the patient needs repeated doses of supplemental insulin >48 hours, please contact the in-patient
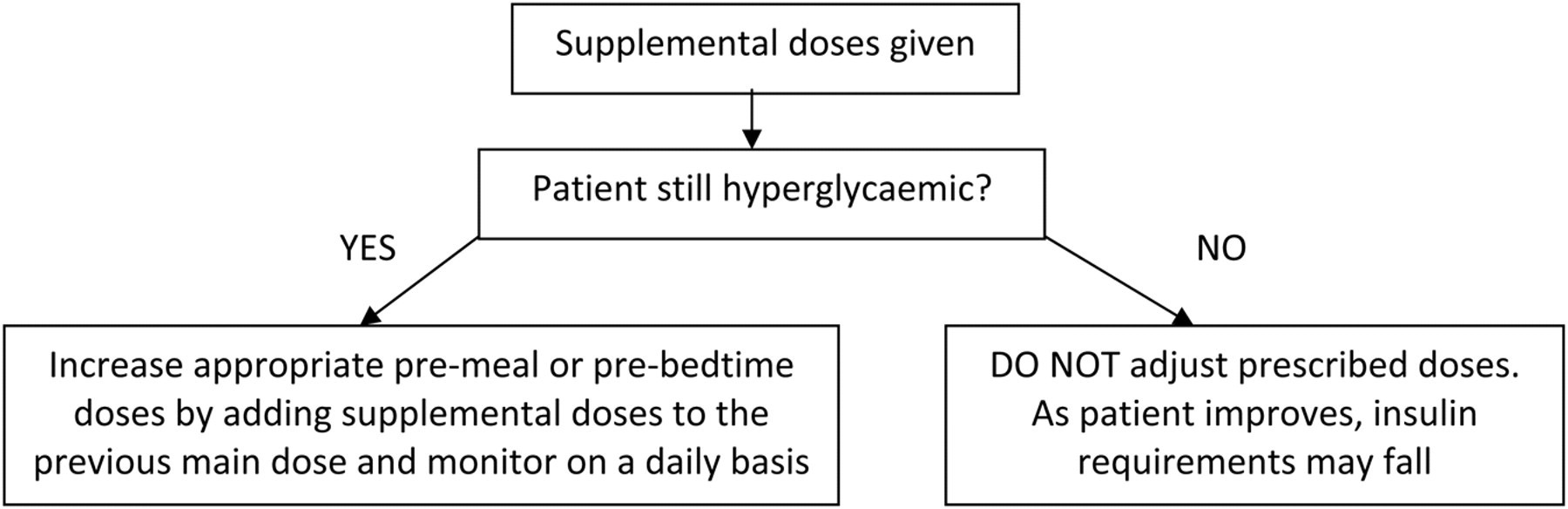
DO NOT JUST REPEAT SUPPLEMENTAL DOSE PRESCRIPTIONS. Incorporate supplemental doses into regimen to ensure optimal glucose control and targets are achieved.
How to be a safer Insulin prescriber:
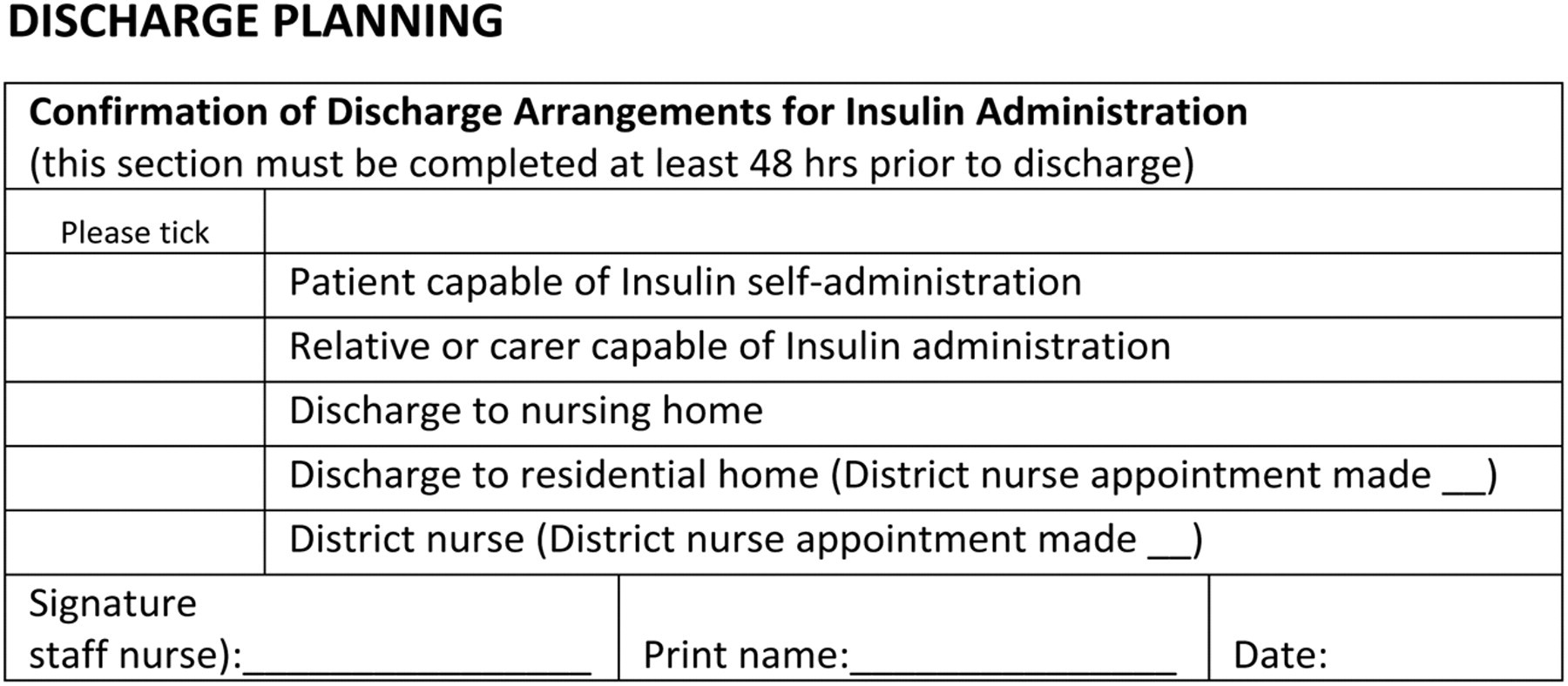
If new to sub-cut insulin therapy, ensure that patients are seen by the DSN prior to discharge.
All patients with diabetic ketoacidosis (DKA)/hyperosmolar non-ketotic state (HONK) should be seen by the Diabetes team prior to discharge to evaluate the precipitating cause of their admission.
Project Evaluation
The ultimate aims of this project are to highlight the issues around insulin prescribing and improve:
Overall quality of care Patient safety Diabetes team utilization Knowledge and awareness among hospital staff Patient satisfaction Staff satisfaction Insulin drug errors Adverse incidents such hypo/hyperglycaemia, deranged glycaemic control Cancelled operations/procedures Complaints Delays in discharge/overall LOS for diabetic patients Inappropriate referrals to the specialist team.
We wish to reduce the following:
The approach to evaluation will be through DATIX (clinical incident) data, further spot audits and the use of structured methods for evaluation.
Many of these recommendations could apply to other high risk medications, but insulin is a good one to tackle first because of the sheer number of the clinical incidents previously reported and the available evidence about making a difference. This project therefore represents a multi-systems approach to tackling the problem of insulin prescribing errors and is aligned with the trust goals of ‘best and safest care’.
Discussion/Analysis
Reducing harm from high risk medications in a hospital environment remains a ‘wicked’ problem. It is not one that can be solved by instructing people to ‘try harder’ or ‘be more careful’. It represents the opportunity to tackle unsafe systems and promote a culture of safety, whereby everything we do is aimed at limiting the risk of serious errors in a vulnerable patient group.
Take for example, the common practice of taking away control of an individual's insulin cartridges and pens when they are admitted to hospital and locking them away in a box next to a patient's bed. This may represent a form of psychological torture in which the patient is far more aware of their glycaemic needs than the busy or poorly trained nursing staff with sub-optimal understanding of the need for regular, timely insulin administration.
The aim of the above multi-system based interventions is to tackle every possible source of error along the line of admission through to prescription and administration. The initial outcome is somewhat surprising and perverse, in that the number of insulin prescribing and administration errors has actually significantly risen following the initiation of this project. Rather than reflecting that the situation has worsened, this suggests that previously the true extent of the problem was even greater than first thought. Healthcare professionals are now more aware of the problems relating to insulin and are therefore more likely to formally report them. We will have to wait until the annual diabetes multi-disciplinary team's hospital-wide in-patient audit, to have a fuller idea of the effect that these changes have made. But at least this will allow an opportunity for the interventions to bed in. A key ideal is to maintain the momentum and ensure that our approach to in-patient drug delivery, not just for insulin, is transformative and becomes a safe and effective system rather than the current unsatisfactory approach.
Footnotes
Acknowledgments
Many thanks to Dr. Nick Vaughan, Dr. Andy Smith, Kate Morel, Josie Wilson, Nikki Robinson, Mark Renshaw, Professor Aidan Halligan, Jatinder Harchowal, Emma Williams, Derek Lington, Dr. Rif Malik, Dr. Anna Crown and Dr. John Quin.