
Abstract
Healthcare is a highly regulated environment. This has driven what could be characterized as a paper-safe approach, whereby organizations are required to demonstrate to a multiplicity of regulators, inspectorates and accrediting bodies that they are paper safe. However, for many organizations, this has not produced a system which is actually patient safe; rather it has in practice operated as a parallel system that does not reflect the true state of safety. This project looks at a quality improvement and patient safety programme and critically asks the question of whether it is flawed because of failure to address issues surrounding Doctors and cultural change. We used Johnson & Schole's cultural web framework to explore the attitudes of junior doctors towards a patient safety and quality improvement programme. Data collection was through the use of focus groups backed up with quantitative data from a web based questionnaire survey. It has been demonstrated that Doctors represent a dominant sub-culture within the NHS and their beliefs, attitudes and value are often at odds or unrecognized by senior healthcare managers. Unless the cultural differences are adequately addressed then transformational change projects such as ‘Best and Safest Care’ are unlikely to succeed. A better understanding of the organizational context allows for more appropriate change interventions to be developed.
Introduction
The notion that hospitals and medical practices should learn from failures, both their own and others', has obvious appeal. Yet, healthcare organizations that systematically and effectively learn from the failures that occur in the care delivery process, especially from small mistakes and problems rather than from consequential adverse events, are rare. The NHS has been slow to learn in comparison with other industries. There have been unprecedented improvements in the safety of air travel, oil exploration and nuclear power which have all occurred because of a cultural change following major disasters. In contrast, hospitals deal with life and death everyday but have been slow to adopt the ideals of the quality improvement movement, which suggests a form of cognitive dissonance when they are so deeply involved with the business of caring.
A central argument in this field is that hospitals don't learn from failure because of two related organizational issues. Firstly, at the frontlines of patient care in hospitals the interpersonal climate often inhibits speaking up with questions, concerns, and challenges that might have contributed to catching and correcting human error before patients are harmed. 1 Moreover, the culture of medicine generally discourages admission of error, thereby greatly diminishing a given hospital's potential to learn from mistakes, both consequential or not. Secondly, features of the work design and culture of most hospitals make workarounds and quick fixes the dominant response to failures, 2 rather than root cause analysis and systematic problem solving, which contribute to organizational improvement and innovation. 3 Much of the literature also suggests that both causes of and solutions to these organizational learning failures ultimately lie in leadership.
The research topic for this project is ‘Best and Safest Care’ which is a patient safety and quality improvement plan and a top priority for a large hospital trust in the south of England. There is concern however about its implementation. Annual staff surveys in the hospital trust in question, rank it in the bottom quartile for putting safety first when benchmarked against other trusts nationally. Complaints and clinical incidents regularly provide examples of where care and treatment could and should have been better, and there is consistent failure to address such issues. Poor communication, bullying, active covering up, inadequate leadership, ineffective team working, racism, lack of respect, intolerance, selfishness and a culture of fear conspire to poison attitudes and behaviours, and result in an unsafe and toxic environment that everyone ‘sees’ but no-one talks about. Worse still, in the field of management, the true nature of these forces is too often regarded as not capable of being openly discussed and is, therefore, rarely addressed.
“We are very good at training clinicians to look after individual patients but fail completely to train them to understand and to look after the system of care”
The dissonance between the espoused ideals of the strategy and its concrete reality are the subject of this project. The aim is to explore issues around whether there is a receptive organizational context for change. Specifically the project will explore the culture of Doctors and how they fit into the strategy. The rationale for studying the trust's interpretation of patient safety improvement is that Best and Safest Care is a crucial, critical strategy, but there is concern that via a top down driven mandate, there is failure to influence the ones who most need to respond to a cultural change and implement the strategy into effective, meaningful operational practice.
What is Culture?
A great deal of the literature on patient safety explores the pervasive barriers embedded in healthcare's organizational systems that make shared or organizational learning from failure difficult. If only it was as easy as the NPSA's guidance suggests;
‘Organizational culture refers to the patterns of beliefs, values and learned
ways of coping with experience that have developed during the course of an organization's history, and which tend to be manifested in its material arrangements and in the behaviour of its members'

Organizational cultures are difficult to assess because their shared beliefs, values, and assumptions are not always explicit. There is increasing international interest in managing organizational culture as a lever for health improvement. In the United States, health policy is directly embracing culture change as a key element of health system redesign 5,6 and many other countries are also focusing on cultural renewal as a potential lever for performance improvement. 7
Approximately one third of NHS organizations in England are currently using a culture assessment tool to support their clinical governance activity, and almost all the instruments used focus heavily on the assessment of safety cultures rather than more broadly on perspectives of quality and performance.
Johnson & Scholes' Cultural web
8
represents culture as an interlinked set of organizational subsystems in which the paradigm drives the visible manifestations of culture (Figure 1). It has been used in the NHS as well as by organizations as diverse as Shell, KPMG, Castrol, the UK Labour Party and as part of high profile education programmes at Manchester Business School, Cranfield School of Management and Lancaster University Management School.
Johnson & Schole's Cultural Web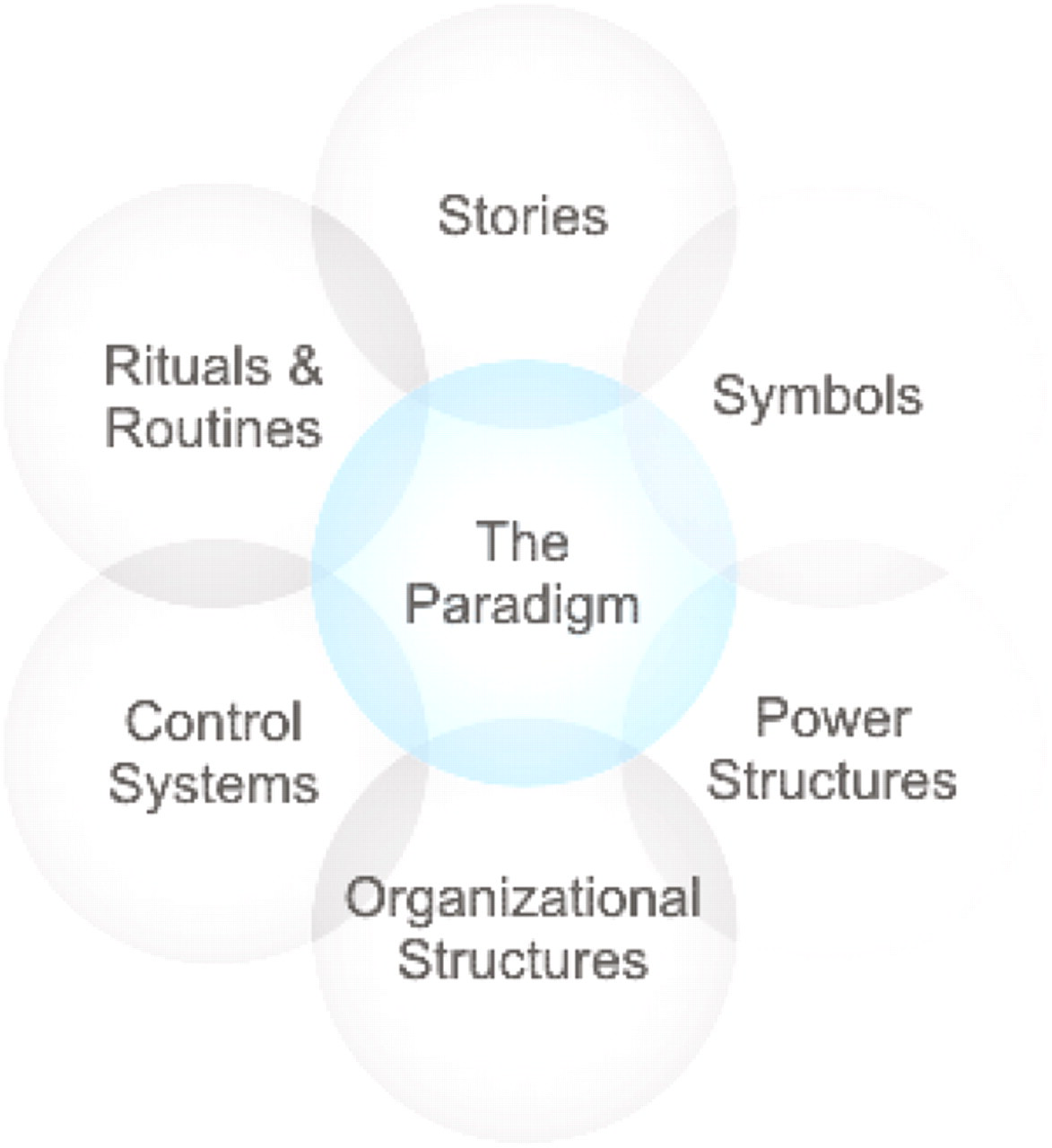
The advantages of this model are that it is relatively straightforward to use, has a long history of use in the business world with empirical results to back it up, it is comprehensive and holistic, and forces one to consider aspects of culture that one may not normally contemplate, such as the differences between the designed and the emergent culture. It is also easy enough for employees to comprehend it by themselves and perform their own analysis.
Ultimately, as Machiavelli suggests, it doesn't necessarily matter which particular tool you use just so long as you demonstrate that you have taken a long hard look at the issue;
9
“the clue to successful statecraft lies in recognising the force of circumstances, accepting what necessity dictates and harmonising one's behaviour with the times”
Method
The focus will be on strategy, change and culture in order to best answer the research question. This project will use the Cultural Web to study aspects around ‘Best and Safest Care’. It will provide information regarding:
The strategic context of the organization The change context itself e.g. culture, competence and the current situation. To help determine the appropriateness of any change approach for a particular context The design choices available to the change agents i.e. selecting an appropriate change approach.
Process
This project will use focus groups of junior doctors in order to produce primary qualitative data. The focus group data will then be used to populate the elements of the Cultural Web. This was then used to design a web based questionnaire and sent out to all 850 junior doctors in the trust for confirmation. This quantitative back up, allows validation of the qualitative data. It also means that the data will be authentic, current and statistically more powerful. With the above data in hand, more appropriate design choices within the cultural context can be completed.
Focus Groups
Focus groups are special discussions exploring a specific set of issues. They are distinguished from both individual and group interviews by the use of interaction to generate data. Focus groups are good for exploring people's experiences, opinions and concerns. It also allows us to tap into the tacit knowledge that quantitative methods would struggle to unearth. Ultimately focus groups are ideal for examining how knowledge, ideas, story telling, understandings and dynamics operate in a given cultural context. 10
Random sampling was used to encourage diversity. All summaries and transcripts were read by EN and MM (independent research assistants), who identified any issues describing management styles by iterative examination. We discussed themes as they emerged and explored them using the cultural web as an interpretive framework where appropriate.
Questionnaires
Focus groups can also be combined with quantitative methods such as questionnaire surveys. This use of mixed methods is complementary and expands the amount of data available for analysis. We used a web based questionnaire (Survey Monkey) and invited all junior doctors in the trust (850) to participate. Questions were based on the emergent themes from the focus groups. To enhance the reliability and validity of the questionnaire it included some relevant, validated questions from the Manchester Safety Framework, which is a facilitative educational tool. 11 It aims at providing insight into an organization's safety culture and how it can be improved among teams.
Results
Table 1 (above) contains key themes which emerged from the focus groups about the current organizational culture at the hospital, supported by a trust wide questionnaire (with a return /completion rate of 66%). Alongside are the elements which make up the future organizational paradigm of Best and Safest Care.
Key themes from the focus groups and elements identified for Best and Safest care
Discussion
What does the cultural web therefore say about the organization as a whole? The results demonstrate that the trust has a large body of committed, autonomous professionals who have strong identity and who are primarily present for the best interests of the patient. The medical profession is theoretically more in line with patient needs and there is little corresponding truck with strategic initiatives because the necessity, the drivers and the likelihood of success do not come into their sphere.
Mapping the Differences between the Current and Idealized Cultures
Cultural strengths highlighted by analysis of the current culture: Doctors are hard working professionals with a strong tradition who work well in teams. There is already a structure in place to monitor their professional development and training. There is a strong element of socialisation due to the long hours, job complexity and emotional commitment. Their core value is the patient in front of them. Factors hindering the strategy or which are misaligned with one another: Doctors are not used to or do not see the need to engage with the wider organization. The goals of the trust are seen as different from their own. A case of the ‘doer and the done to’.
12
If there is a felt need for change, then there is lack of an empowerment to initiate change and to engage junior doctors. Preservation of the medical hierarchy and power bases. Non-whistleblowing culture. Tradition of focusing on the individual and deferring to seniors. Factors affecting encourage and reinforce: Support the engagement of junior doctors who wish to get involved with patient safety and change management programmes. The use of ongoing junior doctor evaluation to include performance management and the formation of personal quality accounts. Factors affecting change: Attitudes to the medical hierarchy. The feeling that junior doctors cannot effect change. The understanding that junior doctors have of the trust's goals. Greater engagement with multidisciplinary teams. To develop the service as well as treat the individual patient. Organizational culture is often very difficult to change because it is so ingrained. This is especially the case with professional bureaucracies such as Medicine, as has been previously commented on by Mintzberg.
13
Beliefs and behaviours to promote: Patient centeredness. Patient before the team. Trust goals have value and relevance. The belief that junior doctors are empowered and will be supported to bring about successful change. Doctors need to be able to complain about system failures rather than to be adaptive conformers and just maintain constant quick fixes and workarounds.
Doctors tend to work for a different value – that of the individual patient, rather than the abstract, perceived irrelevant goals and strategies of senior management or of the organization. Whilst however, this is believed to be true, the fact that there has been such a surge of interest in Clinical Leadership from junior doctors means that within the next generation, there is a bubbling frustration with the way that the health service is run and organized. Not all Doctors are leaders, and not all will be interested in adopting strategic goals but it may only require a committed few to ‘lead’ others in the right direction to bring about convincing change. This perhaps is the focus that management needs to include: get some committed junior doctors who are interested in patient safety and let them undertake some high profile projects with the full support of management. This will allow both role modelling and spread the message that doctors and managers are on the same side and working towards the same end.
Cultures are notoriously difficult to change because they cannot be controlled in the way that work can be organized because a culture is not something that an organization completely owns or develops in a certain way. Different functions within the same organization, for example a team of junior doctors, have a very different culture from a team of accountants. In a large hospital, there are several overlapping cultures. Some aspects of culture can act as a barrier to change. Junior doctors for instance, wish to preserve their distinct identity, which is traditionally separate from the ‘dark side’ of management (an oft repeated term), focus on their main value (the patient in front of them) and maintain their firm's position in the medical hierarchy (which is a separate, contrarily non-corporate part of the wider organization). However, things are not all disparate, the 3500 year old medical tradition is dedicated to patient care, so by being able to understand which features of the culture help to support change and which hinder it, then management will be in a better position to influence improvements in the direction of ‘Best and Safest Care’.
Conclusions
Cultural change is not something that can be achieved at the flick of a switch. Cultures develop through social interactions in fields of practice. Everyone becomes aware of what types of thinking and behaviours are broadly acceptable. Change cannot happen without some form of disruption. Managers and clinical leaders must therefore recognize their role in preparing people for the disruption of change and consider the many ways in which progress towards an improvement, even one that brings many benefits, impacts on individual lives and improves the experience of care. This project has demonstrated that this is not occurring in the trust in question. Despite a strong vision, it has not been communicated adequately (if at all), the sub-culture of the medical profession has not been acknowledged and the design choices have not taken junior doctors into consideration. This seems both surprising and frustrating in the context of a significant change management programme.
Rethinking the project using an understanding of the cultural context provides better design choices:
‐ policies and procedures updates (of relatively minimal value), ‐ need to undertake a staff survey and patient satisfaction survey, then using the views of staff and patients provides powerful evidence for persuading the workforce that change is necessary. Lever is to generate readiness for change in the workforce through the communication of survey findings. ‐ Performance management; checklists, appraisals, personal quality accounts ‐ Generate interest in Best and Safest care through regular communications updates; emails and newsletters ‐ Bring in after action review for greater reflection in practice ‐ Nominate patient safety champions ‐ Hospital awards with a focus on patient centeredness ‐ Re-launch the Leadership development programme in line with best practice
The above outline therefore provides a more appropriate, context sensitive approach to introducing Best and Safest care as a trust wide improvement programme. The data that we have gathered suggests that the existing approach is fundamentally flawed in that it does not take into consideration the underlying organizational culture both as a whole and specifically with regards to the medical profession. Culture change is difficult and changing individuals requires considerable investment, for example in communication, education, training and support etc. But the use of the cultural web has given us a fresh, relevant insight into the implementation of strategy.
The secret of care for the patient is to care for the patient. The challenge for management is to extend this as care for the service, or the wider organization. 14 No amount of regulation, process improvement or reimbursement can change this fundamental fact. It's about the people, not the policy.
Footnotes
Acknowledgments
Many thanks to Professor Aidan Halligan from UCLH, Tove Steen Sorenson-Bentham and Barry Lee Scherer of Brighton Business School, Clare Penlington of KSS Deanery and Stephen Morris, Jan Nawrocki, Des Holden and John Quin of RSCH, Brighton.