
Abstract
Superficially, screening programmes may seem relatively straightforward to organize. However they are much more complicated than appears at first sight. The UK National Screening Committee, set up in 1996, advises all four nations on the introduction of new screening programmes and the improvement or, less commonly, cessation of an established programme. Most of the established programmes have a Programme Centre which advises on the running of the programme and sets standards. Because true outcomes may be some years hence, these standards usually relate to the process, rather than health improvement. There are many different stages in the programmes from ascertaining the target population to timely diagnosis and prompt management. This means there are a number of places where the system might fail. Therefore, part of the advice offered by the Programme Centres relates to failsafe mechanisms. These are backup systems, designed to make sure that no child slips through the net and all are correctly assigned to high or low risk groups. These systems may be expensive, but are necessary and cost effective. A missed diagnosis causes unnecessary disability to the child and distress to the parents, and may be very costly to the health service.
Introduction
‘Screening is a process of identifying apparently healthy people who may be at increased risk of a disease or condition. They can then be offered information, further tests and appropriate treatment to reduce their risk and/or any complications arising from the disease or condition..’.
1
Screening is different from normal medical care in that it is offered to people who do not suspect they have a disease/condition and have not sought advice about that disease/condition. On the other hand, most medical care is given to people who have sought advice. Therefore, it can be argued that the ethical imperative to get it right is even greater than for other forms of medical intervention. This is even more so, as screenings tests are not usually diagnostic. As Winston Churchill said “The world, nature, human beings do not move like machines. The edges are never clear-cut, but always frayed. Nature never draws a line without smudging it.” 2
The UK National Screening Committee (UKNSC), set up in 1996,
3
advises the Ministers for Health, or their equivalents, in all four nations, on the introduction, continuation (or not) and improvement of all population screening programmes. All new programmes are solidly evidence based and Quality Assurance is an integral part of them. A number of factors have to be considered before approving any new programme:-
The condition in question should cause an important health burden; It should have a known natural history; There should be a presymptomatic stage; There should be an accurate screening test; There should be an effective management option; The screening programme as a whole should be acceptable to the population.
Screening programmes
Current programmes can be divided into those for cancer (cervix, breast and bowel), for vascular disorders (abdominal aortic aneurysm and diabetic retinopathy) and for maternal, neonatal and childhood conditions. Figure 1 shows the maternal and neonatal programmes. 4

Maternal and Neonatal Screening Pathways 4
The main programmes have Programme Centres aligned to them. Each has a number of responsibilities including aiding implementation of new aspects of a programme, setting standards, overseeing national data collection and monitoring adverse events. For the purpose of this article, I will look at newborn blood spot screening in UK. Five conditions are currently screened for (Table 1).
Conditions screened for using the newborn bloodspot sample
*Implementation dates varied across the four UK nations
Phenylketonuria is an inherited condition that affects 1 in 10,000 babies. Untreated, they develop serious, mental disability which is largely irreversible. However, if treated with a special diet they have little if any disability.
MCADD is also an inherited disorder of metabolism, affecting 1 in 10,0000 babies. Untreated it can lead to serious illness or even death. Treatment is aimed at making sure the babies have regular feeds, especially when ill. This precaution has to be observed all through life.
Sickle cell diseases are a group of inherited diseases where the red blood cells are not formed properly. This can cause pain and damage to the body, serious infections and death. Treatment helps reduce the chance of this happening
Congenital hypothyroidism affects 1 in 4,000 babies and is due to a lack of thyroxine, a hormone. Untreated the babies do not grow properly and their development is delayed. Treatment is easy with thyroxine tablets.
Cystic fibrosis is an inherited disorder affecting 1 in 2,500 babies. Untreated it results in poor growth and lung problems. Treatment is complicated but means people with the condition lead longer, healthier lives.
There is a fairly common perception that screening programmes are relatively straightforward. The test is offered and administered, a result obtained and the appropriate action taken. In fact it is much more complicated (as shown in Figure 2).
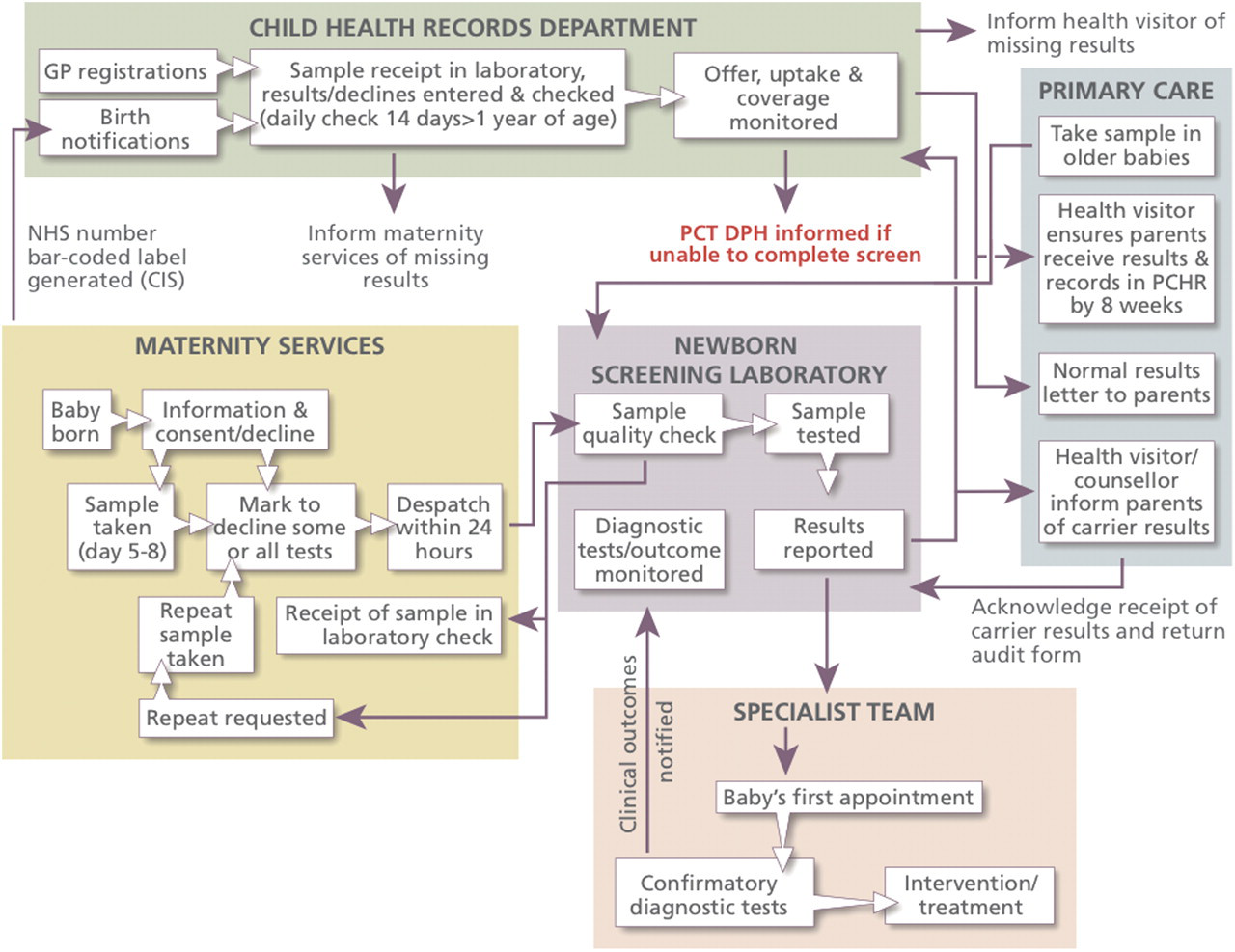
Detailed pathway for newborn bloodspot screening
Many providers are involved in the pathway and it is important that the process is seamless. It should be clear who has responsibility at each stage and that responsibility is not relinquished until it has been clearly passed on to someone else. Each provider should have someone responsible for screening and someone should have oversight of the complete process.
There are numerous places in the pathway that could fail, so it is essential to monitor the programme closely. At one extreme, one could monitor the yield of cases detected.
However, the conditions are uncommon (PKU and MCADD each occur in only about 1 in 10,000 live births and, together, all five conditions are present in about 14 children per 10,000 live births). Using yield, alone, would be a very crude way of monitoring the programme as chance variation each year will mean, especially for smaller units, no cases might be seen one year and twice as many as expected in another. Monitoring of the process is therefore essential as a more accurate early warning system. With this in mind, national standards have been set and are reported on a yearly basis. More recently, Key Performance Indicators (KPIs) have been introduced and will be returned quarterly.
Standards
National Standards for Newborn Bloodspot Screening and Means to Facilitate their Achievement 5
For each of these standards, numerical levels are set which it is expected providers should reach. These are often at two levels - what should be currently achievable and a higher standard to aspire to. A number of initiatives have been instituted to facilitate their attainment, some of which are listed in Table 2.
Failsafe procedures
No system is perfect and so it is important that various failsafe mechanisms are in place. Soon to be rolled out is a national IT system whereby CHRDs and maternity units will be able to monitor the receipt of bloodspot cards by laboratories. If a card has not been received in a timely fashion, the maternity unit will be able to chase it up, so that a sample can be taken before too great a delay.
Also being explored is the potential for laboratories to notify results electronically to those responsible for the care of children. This will be more speedy than post and also more accurate, as transcription errors can be avoided.
One of the most important failsafe mechanisms is to fully inform the parents of what is happening. Parents should be informed that a sample will be taken at 5–8 (ideally five) days. Thus, when the sample is not taken at the expected time, they may contact the midwife or health visitor. The midwife should write in the Personal Child Health Record when the sample is taken and the result should be communicated to the parent when the baby is no older than six weeks old. Almost all positive results will have been communicated by then and it is not acceptable to say that ‘no news is good news’. All normal results must be communicated to the parents, not just those that are abnormal. When a parent has not received a result, they can contact their GP or HV.
Conclusion
Screening programmes are complex, involving many stages and a number of providers. There is a potential for the system to fail at a number of points. However, under national guidance, a number of initiatives are in place to prevent this and the process can be monitored, to ensure that any failures are picked up early. Good co-ordinated oversight is essential, both within and across providers. Parents can and should have an important part to play in this.
Further information
About newborn blood spot screening:
Support about sickle cell and thalassaemia linked antenatal and newborn screening:
About screening in general: