
Abstract
Introduction
Little is known about the patient safety culture within surgical departments in UK hospitals. What has been done to date is to survey only permanent senior staff opinion of the safety culture in their institution. This study surveyed both consultant and trainee views on perceived patient safety and compared the results between these two groups.
Material and methods
The previously validated Team Work and Safety Climate Questionnaire was configured in Survey Monkey format and sent to all surgical trainees and consultant surgeons in the South West Strategic Health Authority. Two reminders were sent to achieve as high a return rate as possible.
Results
Two hundred and ninety-six replies were received. Forty-four percent of trainees and 30% of consultants responded to the survey. Consultants consistently rated a higher safety culture than surgical trainees. Only 2.9% of trainees believe their patient safety concerns would be acted upon by hospital management. There is notable variation in perceived patient safety culture between hospitals.
Conclusion
This study has suggested that the patient safety culture in hospitals, within a Strategic Health Authority, is variable and sub-optimal when viewed by surgical trainees and their consultants. This study also provides some evidence that the perception of patient safety in an organization varies according to clinical experience. As trainees deliver a great deal of clinical care, surveys of safety culture should include this group. As perceived patient safety culture is correlated to clinical outcomes, validated safety surveys might form part of the assessment of a hospital's performance, along with outcome and patient satisfaction.
Introduction
Medical errors are a major cause of mortality and morbidity. The National Patient Safety Agency (NPSA) estimates that 10% of all hospital admissions suffer an adverse event defined as a medical error that results in harm to the patient. One percent of all admissions die as a result of an adverse event. In practice this means that in England and Wales 300,000 adverse events and 30,000 deaths are recorded every year. This figure of 30,000 deaths a year is a greater number of deaths than the combined annual mortality from colorectal, prostate and breast cancer. 1 Even these striking figures may be underestimating the extent of the problem because recent studies in the surgical literature 2 indicate the adverse event rate could even be as high as 20%. As a result, patient safety is now a national and local priority and most acute trust board meetings in England will have patient safety as their first agenda item.
In 72–80% of adverse events, human factors such as communication, leadership, team-working, decision-making, situational awareness and coping with stress and fatigue are the underlying causes. 2 Furthermore, the number of adverse events within hospitals appears to correlate with clinical outcomes. 3 This suggests that the safety culture within an acute hospital is related to both the number of patient safety incidents, as well as the clinical outcome. 4–10 The Mid Staffordshire NHS Trust Inquiry highlighted the poor safety culture and lack of reporting as the most important factors in poor care and reported excess deaths. 11 If ‘quality’, as defined by ‘High Quality Care for all’, is a composite of ‘safety, effectiveness and patient experience’ then measurements of the safety culture within an organization might be a useful indicator of a hospital's clinical and organizational quality. 12
At present the majority of patient safety efforts have been directed at board and senior doctor level. In the NHS most frontline clinical activities are conducted by medical trainees and junior nurses. It is estimated that 80% of direct patient-related ward-based activity is performed by medical and nursing trainees. 13 Recent restrictions to working hours have left newly qualified doctors managing large numbers of patients on the ward, and managing emergency admissions that includes covering specialties outside their immediate area of expertise. The recent Collins report drew attention to the concerns that many trainees privately voice about their insufficient expertise and absence of senior cover. 14 This might partly explain why some studies suggest that senior doctors and managers overestimate the safety within their institutions as trainees appear to be reluctant to voice their concerns in public. 15 The NPSA issues a series of patient safety alerts e.g. on chest drains and naso-gastric tube insertion, which are sent to the Chief Executives of Trusts who distribute these via e-mail to senior staff. These alerts are not consistently passed on to the trainees' e-mail accounts, and even if they are, anecdotal evidence indicates that trainees do not regularly use their hospital e-mails. Finally, hospitals aim to gather data on the number of adverse events by the use of critical incident forms. Studies show that typically only 2–5% 2 of adverse events are reported using incident reporting systems. Consequently, it appears that many factors contribute to an environment that might fail to accurately identify concerns about the quality of healthcare delivered on the frontline.
The factors outlined above led us to examine perceived safety culture in surgical trainees and their consultants. Safety culture is difficult to measure but an increasing body of evidence shows how it can be done. 16–20 In this study we use a common, validated questionnaire to assess the safety culture and team-work within hospitals in the South West Strategic Health Authority. The aim of this study was twofold: to assess the team-work and patient safety attitudes of surgical trainees and to make comparisons with the attitudes of consultants. The purpose of the study was fully supported by the South West Strategic Health Authority.
Materials and methods
The survey was sent to all surgical trainees (CT1 – SpR6) and consultant surgeons in hospitals in the South West Strategic Health Authority. This was achieved using the databases of trainees from the Severn and Peninsula Postgraduate Schools of Surgery and the database of consultants from the Royal College of Surgeons. The previously validated University of Texas Teamwork and Climate Survey was used. 18 Slight modifications were made by ‘anglicising’ the text and two extra questions were added in light of the South West-wide initiative to introduce the WHO Safer Patient Checklist and preoperative patient safety briefings. 8 The questionnaire was formatted using Survey Monkey and sent to all consultants and trainees in the region by e-mail. Two reminders were sent to all potential participants. The responses were tabulated as shown in Tables 1 and 2. Responses were stratified so comparisons could be made between trainees and consultants and between individual hospitals.
Questionnaire results, team-work section, trainee and (consultant) % responses
Questionnaire results, safety attitude section, trainee and (consultant) % responses
Results
One hundred and five surgical trainees (44% response) and 191 consultants (30% response) took part in the survey, giving an average rate of 34%. Although apparently low this compares favourably against other internet-based surveys of surgeons where the response rate was between 14% and 34%. 21,22 Low response rates are a consistent feature in surveys but there is evidence that this does not affect the validity of the survey. 23 A likely explanation for this apparently low rate is the feeling of ‘survey overload’ amongst doctors in the UK, as they receive many e-mail surveys.
The results are displayed in the tables and figures.
Across the vast majority of patient safety domains consultants consistently rate the safety climate as higher than trainees (Tables 1 and 2, Figures 1 and 2). This is particularly evident on questions such as ‘My suggestions about patient safety would be acted upon if I expressed them to management’ (consultants averaged 3.15/5, compared to a trainee score of 2.6/5). Figures 3 and 4 show there is variation within the levels of surgical trainees, but an equivalent variation according to consultant seniority is not seen. Trainees with less experience appear to feel less safe being treated in their own hospitals. Figure 3 shows an apparent reduction in confidence in hospital management as perceived by trainees as they move to their middle years (ST3– SPR4), only for confidence to return in their last two years of training.
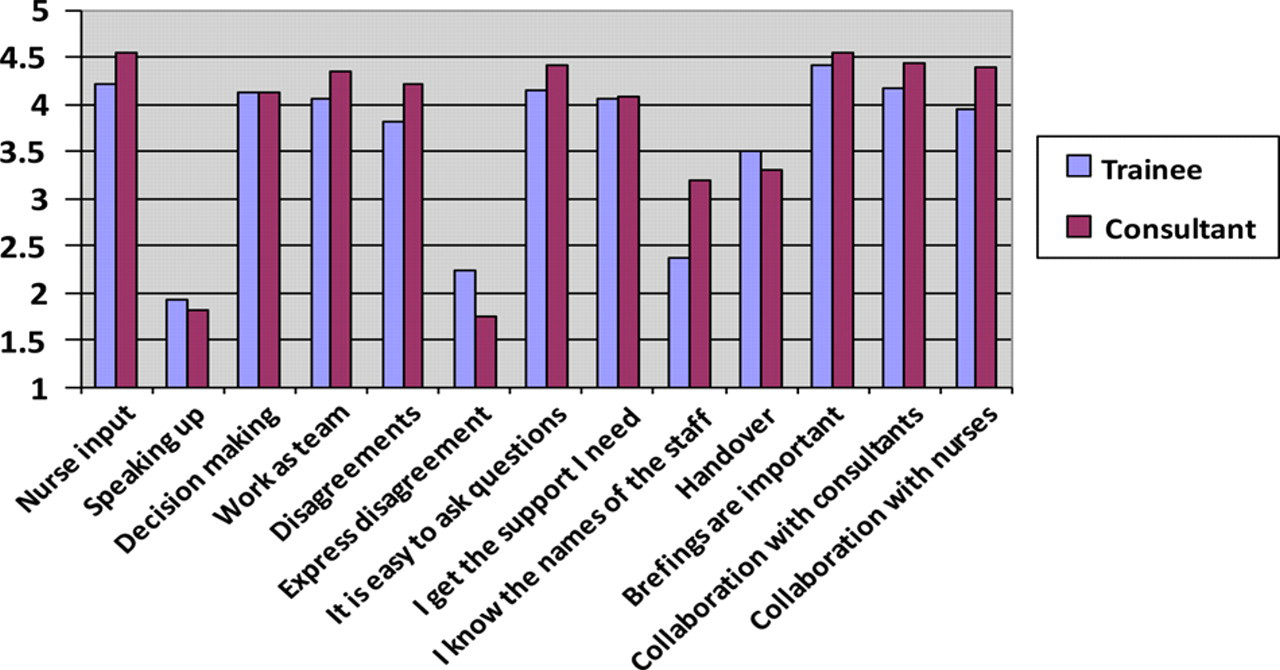
Comparison of consultant and trainee responses to selected team-work questions (5 is agree strongly, 3 neutral and 1 disagree strongly)
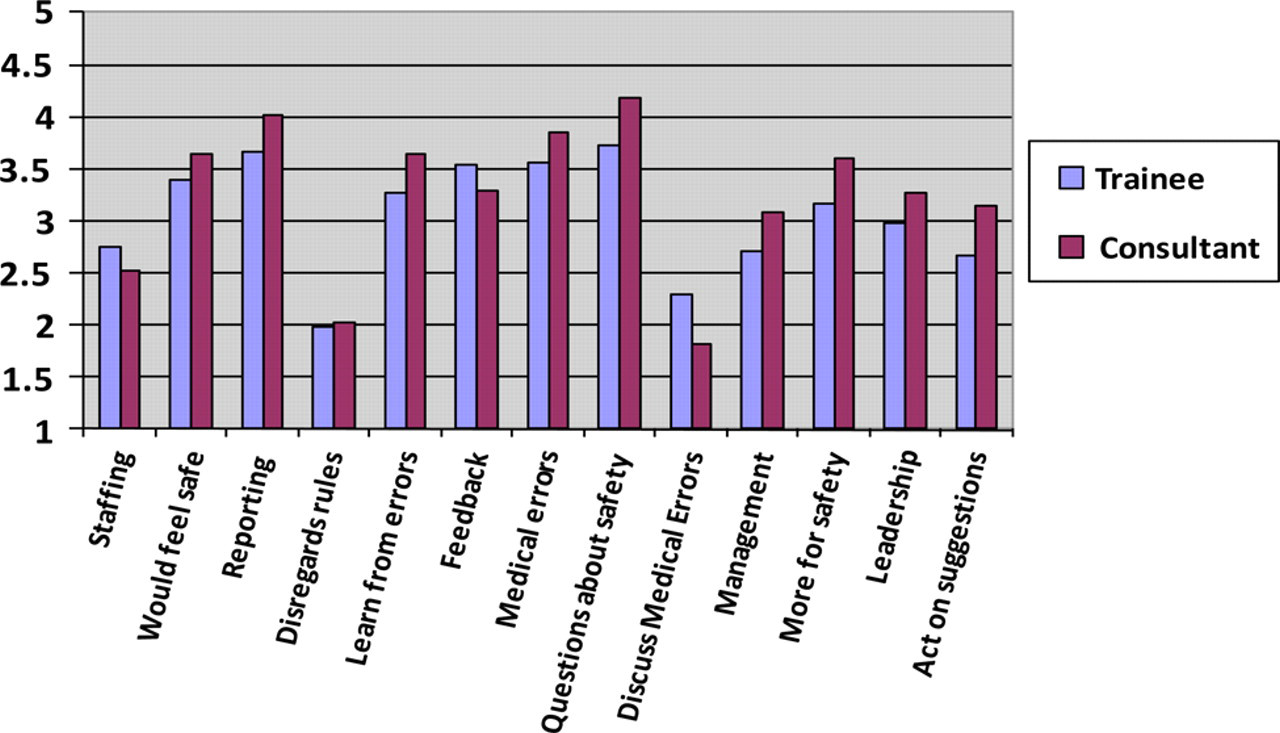
Comparison of consultant and trainee responses to selected safety attitude questions (5 is agree strongly, 3 neutral and 1 disagree strongly)
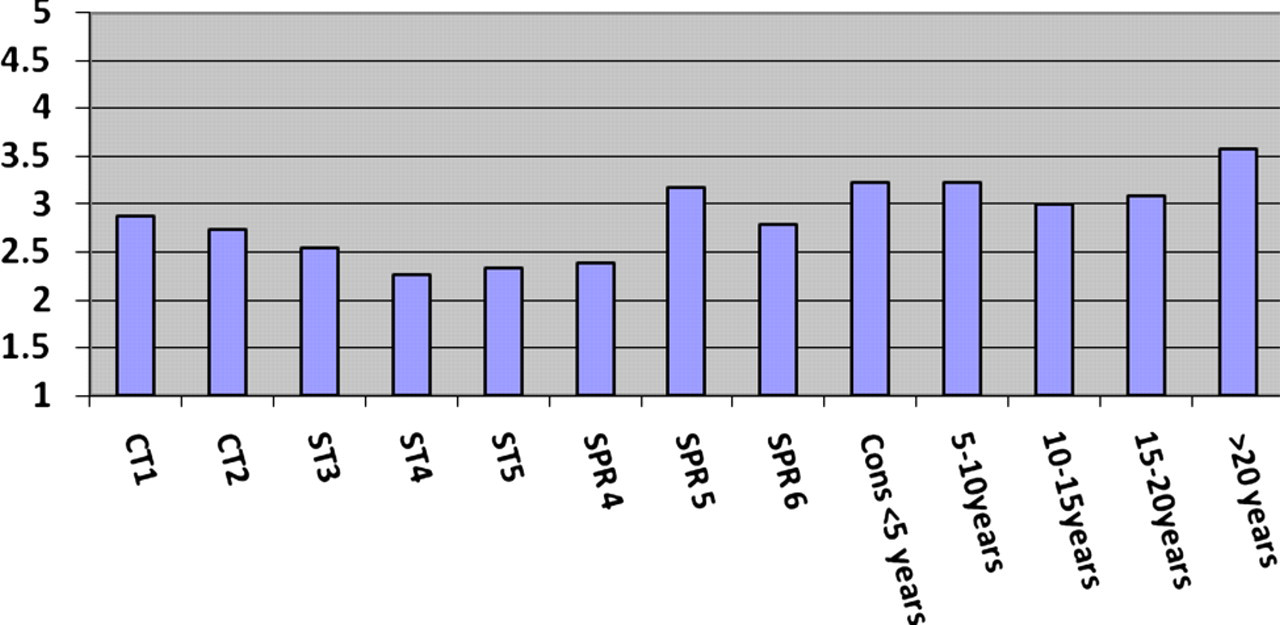
Responses to the question 'My suggestions on safety would be acted upon if I expressed them to management' (5 is agree strongly, 3 neutral and 1 disagree strongly)
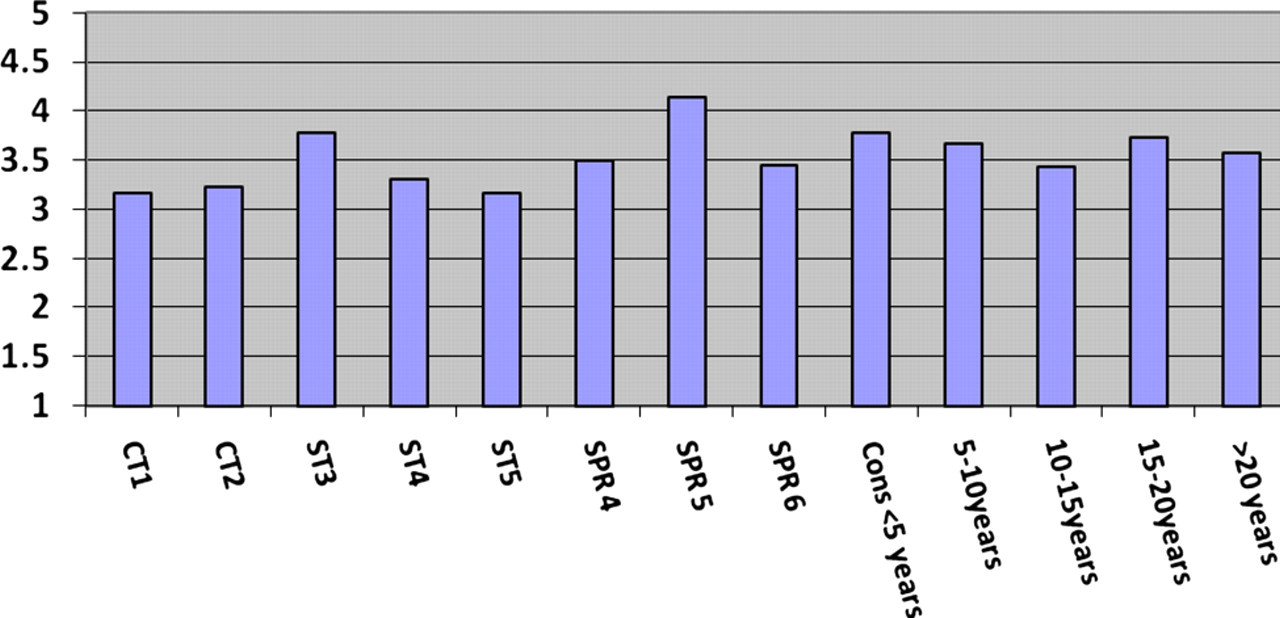
Responses to the question 'I would feel safe being treated here as a patient' (5 is agree strongly, 3 neutral and 1 disagree strongly)
Discussion
The perceived patient safety culture varies between trainees and consultants, with more senior staff evaluating the safety culture to be safer than trainees. This effect is most marked between consultants and trainees but there are also differences within the years of training. A possible explanation is that trainees are more directly involved with incidents that directly affect patient safety and arguably may more reliably estimate the real risk of adverse events. Although this paper cannot prove this it is intuitive that clinicians working in areas where safety incidents occur (generally more junior) are more likely to rate the safety culture worse than those who are at some distance from the specific incidents (more senior doctors and consultants). Studies to date have looked at permanent staff's attitude to patient safety and the findings in this study suggest that more senior staff might overestimate the safety of the clinical environment. 24–26 Perhaps most worrying of all is the response to the question ‘My safety concerns would be acted on if I expressed them to management’. Only 2.9% of trainees agreed strongly with this statement compared to 17.9% of consultants. Surgical trainees might in practice be mistaken in their belief and management would act on their concerns. Nevertheless, if they perceive a reluctance on the part of management to act on critical incidence reports, they might be less likely to report them using hospital reporting systems.
Assessing the safety of hospitals is difficult and is currently not done at a national level in the UK. The National Patient Safety Agency (NPSA) collects incident reports but these are anonymized and so they do not show the rates within hospitals, and even if they did, as only 2–5% of incidents are reported, the data would not be valid. Safety culture surveys are a surrogate for multiple safety-related statistics in hospitals; re-admission rates, adverse events and clinical outcomes. 4–10 As previous studies have shown safety culture surveys can shed light on the safety of hospitals; although clearly rigorous data collection within trusts would be more accurate it is not currently available out of research settings.
All trainees are invited to take part in an annual survey of training by the Post Graduate Medical Education Body (PMETB), now part of the General Medical Council (GMC). This is an extensive online survey covering many aspects of training. However, there is little focus on patient safety, domain 1 of the GMC standards for training. Only a small proportion of the current survey questions address patient safety and infer conclusions about patient safety by proxy data such as ‘handover’ rates and supervision. As this is such a significant issue to patients' lives, their wellbeing in hospital and a primary political priority, then arguably the format of the questionnaire should change, and explicitly and clearly focus on ‘patient safety’. Whilst this data would only be a surrogate for safety within specific hospitals it could highlight areas that should be investigated futher.
Shortcomings of this survey
The response rate was low, which was disappointing given the importance of the topic. As many surveys are sent to trainees and consultants, it may be that ‘survey overload’ contributed to the relatively low response rate. Can one make judgements about the differences between those that contributed to the survey and those that didn't? Not easily, but it could be argued that this survey will overestimate the perceived safety culture as respondents who think safety surveys are important comply with the request. Judgements about whether this group perceive their institutions to be safer or otherwise than non-respondents is not possible, but as stated before low response does not necessarily affect the validity. 23
Human factors
Human factors such as team-work, communication, coping with fatigue and stress, decision-making and situational awareness appear to be the crucial areas which need to be addressed if we are going to reduce harm. There is good evidence to show that training in these areas reduces harm and improves outcome. 8,27 Does this affect mortality? Although a direct link between mortality and improved team-work has proved difficult to demonstrate, a recent multi-centred trial of communication and team-work training, together with the introduction into theatre protocols of briefings and checklists did demonstrate a reduction in both deaths and morbidity in surgical patients. 8 There is a growing belief that more effort and time needs to be focused on patient safety in undergraduate and postgraduate training. For example, the South West Strategic Health Authority Patient Safety and Quality Improvement Programme now mandates that all Foundation Year One doctors received a half-day training session, delivered by trained experts in human factors, as part of their induction week. All core surgical trainees in the Severn Deanery have a day course in human factors and team training but there is still a long way to go before such training is considered adequate.
Interhospital variation
One surprise in analysing the data was the great variation in perceived safety culture between trusts. Figure 5 shows the summed (i.e. both trainees and consultants) responses to the question ‘I would feel safe being treated here as a patient’. 5 would mean that the respondents ‘strongly agreed’, 4 ‘slightly agreed’, 3 ‘neutral’ etc. As can be seen the average response is 3.6, somewhere between ‘slightly agree’ and ‘neutral’.

Combined results filtered by hospital (1–14), to the question ‘I would feel safe being treated here as a patient’ (5 is agree strongly, 3 neutral and 1 disagree strongly). Highest score 4.46, lowest score 2.3
There appears to be significant variation between safety cultures in participating hospitals. Whilst the majority of responses cluster around a mean of 3.6 there are clearly some outliers (highest score 4.46, lowest score 2.3). What this means for hospitals that score poorly is not clear, but at the very least it suggests that there might be a serious problem in terms of critical incidents.
Conclusion
This study suggests that the perceived safety culture in hospitals within a single Strategic Health Authority is sub-optimal and there are noticeable differences in responses between surgical trainees and their consultants. It is a cause for concern that all surgical staff have significant concerns about patient safety in their institution and there is a case for including patient safety culture surveys as part of the data routinely collected when measuring a hospital's performance. At the very least such surveys are highly likely to shed light on hospitals or departments that might be a cause for concern. Why more inexperienced doctors perceive their institution to be less safe than their senior colleagues warrants further investigation, but prompts two responses. Firstly, that there is a case for more specific questions about patient safety than exist at present in the GMC annual survey of trainees. Secondly, all patient safety surveys should look to be more inclusive and recruit replies from front-line medical and nursing staff if a true picture of the safety culture is to emerge.