
Abstract
We describe the evolving development of a trigger review process as part of a pilot national safety improvement programme, which enables primary care clinicians to rapidly search electronic patient records to identify latent risks and previously undetected adverse events.
Introduction
In the past decade, the ‘global trigger tool’ method has been implemented in many acute hospitals in the United Kingdom (UK) and worldwide to help estimate the prevalence of adverse events found in these settings using medical record reviews. 1,2 As part of the nascent patient safety agenda in UK primary care, there is growing interest in this approach to measure and monitor harm rates found in electronic patient records. 3 Related development work is ongoing across the UK home countries, although differences in purpose and practical application may be evolving. 4–6
The global trigger tool is commonly associated with the Institute for Healthcare Improvement (IHI), a US-based organization (
Examples of ‘triggers’ and their rationale 8
A&E, accident and emergency department; FBC, full blood count; GP, general practitioner; INR, international normalized raitio; LFT, liver function test; U&E, urea and electrolytes
The original purpose of the ‘trigger tool’ as applied in hospital-based care was to serially estimate ‘rates of harm’ found in small samples of ward-based medical records. In this way external reviewers could ‘objectively’ determine and monitor harm rates across local hospital systems over time and inform clinical teams of progress. The potential disbenefits of this approach are a lack of ‘sharp-end ownership’ of these data which may hamper collective improvement efforts, while additionally there is no attempt to investigate why identified harm events occurred. 2
From a primary care perspective, it is becoming clear that there may be major feasibility and statistical challenges to be overcome if this original measurement purpose is ever to become a frontline reality in this setting. 8,9 However in one sense the focus on measuring harm rates in clinical settings is a distraction, as there are arguably greater risk management benefits to be gained from applying trigger review as a rapid method of audit and feedback.
In this article we describe how the trigger review process is evolving as part of the Health Foundation-funded Safety Improvement in Primary Care (SIPC) pilot programme in Scotland. 10 We also share specific threats to patient safety uncovered by clinicians undertaking structured reviews of electronic patient records as part of the programme. By considering these threats, we believe primary care teams in the UK and internationally can rapidly and feasibly put this learning into practice to identify and mitigate the risks of harm to patients.
Patient safety and primary care
The great majority of patient contacts take place in primary care. 11 High-volume and ageing populations, new technology, powerful medications, imperfect systems, increasing clinical complexity and managing uncertainty are some of the factors which combine to intensify the risks of harm to patients in general practice. 12,13 In the UK, evidence of the key threats to patient safety in this setting is limited compared to acute hospital care, where most related improvement activity was – until recently – concentrated. 14,15
Our restricted knowledge of what goes wrong and how this can impact on the safety of patient care is largely derived from multiple but methodologically limited information sources such as: complaints systems; feedback from patients; medicolegal cases; fitness-to-practise hearings; incident reporting systems; and significant event analyses. 16,17 Taken together it is evident that patient safety is being compromised and perhaps not infrequently. In response, recent policy pronouncements 10 and research initiatives 18 have prioritised the need for concerted action to make primary care safer.
About the SIPC programme
From March 2013, SIPC has ambitions to become the first known programme to implement targeted safety improvements in primary care on a national basis. Its underlying methodology adheres to the short-term learning and action principles which characterize the IHI Breakthrough Collaborative Series. 19 The Phase 1 pilot commenced in May 2010 with recruitment of 20 general practice (GP) teams in three regional health authorities, rising to around 40 practices currently. A key aim was to raise awareness of patient safety concepts and provide training in different improvement methods to selected GP team members at organized learning sets (usually a GP, a GP manager and GP nurse). They then returned to frontline practice to share and implement this learning (during the action period phase) with further aims to reduce incidents of harm and improve the reliability of specific aspects of healthcare delivery. In Phase 1 patients with a diagnosis of heart failure or taking high-risk medication (Methotrexate or Warfarin) were selected as the clinical focus for improvement efforts.
Structured review of electronic patient records
Currently safety incidents are reported by patients, identified directly by clinicians or highlighted by colleagues as part of routine practice (or are not highlighted at all for whatever reason). However, some incident types cannot be detected so palpably. Systematically reviewing medical records for previously undetected incidents and threats can provide the GP team with a whole new perspective on patient safety. 20 It also offers valuable opportunities to take pre-emptive action before harm can occur or pinpoint learning needs where patients were found to be unintentionally but avoidably injured.
By adopting a more structured and methodical approach the trigger review process helps facilitate a quicker, targeted evaluation of the medical record – potentially offering greater cost-benefits than a full open record review which can be time-consuming and cumbersome in comparison. In the SIPC programme, the trigger review process is one of five core interventions being implemented by participating GP teams alongside clinical care ‘bundles’ (to improve the reliability of evidence-based care provision); Plan-Do-Study-Act (PDSA) cycles (to facilitate small, rapid improvements in care processes); safety climate assessment (to help teams build a team-based safety improvement culture); and capturing patient experience (to learn from patients about improving safety). Full details of the method suggested for screening electronic patient records (Figure 1) as part of the review process were recently published. 8,9
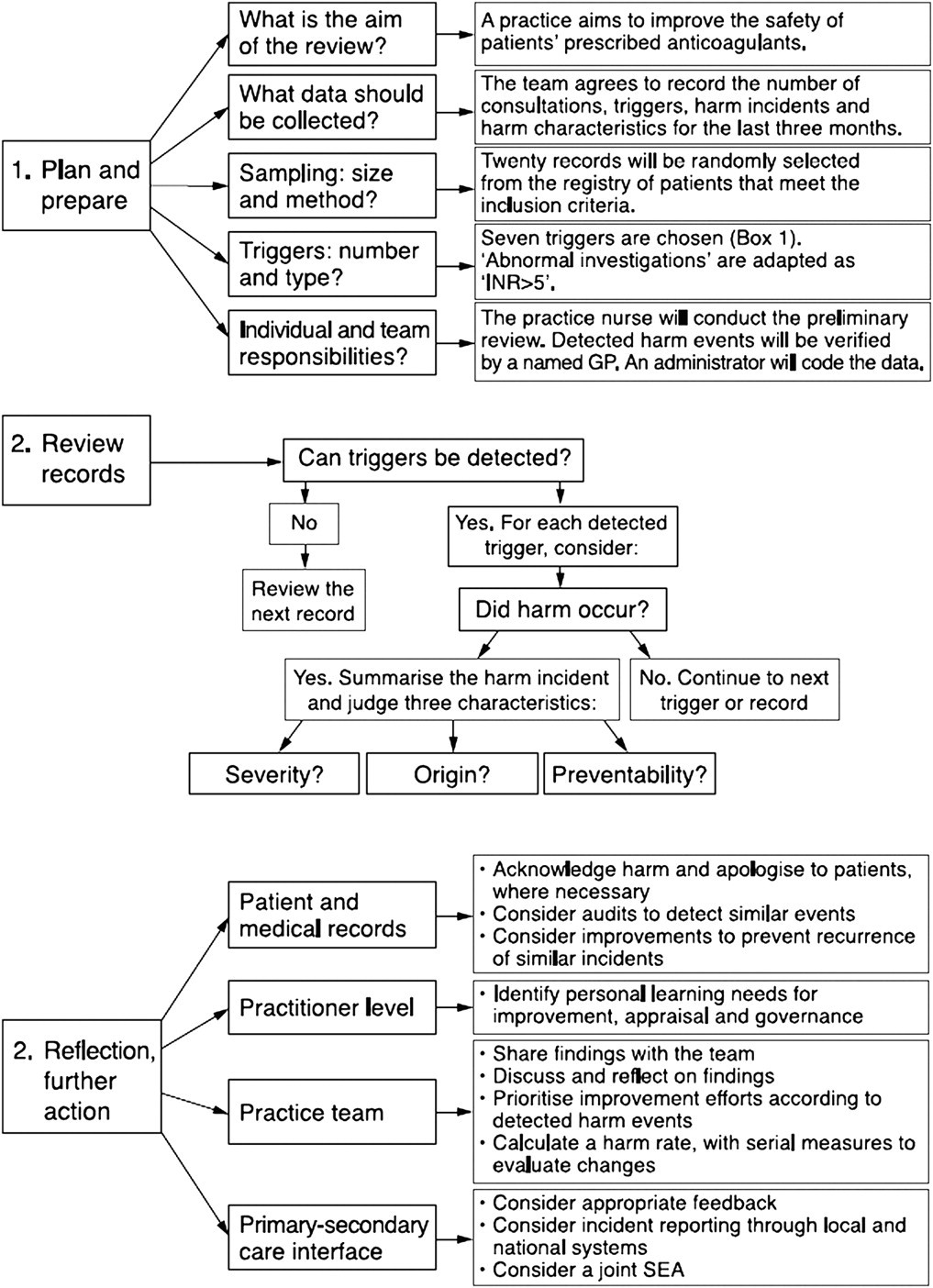
A trigger tool process for primary care 9
At least two clinicians and an administrator from each participating GP team were trained in the trigger review method with follow-up advice and support provided at practice level. Each team applied the process on a minimum of 20 randomly chosen electronic records from a predefined practice population (e.g. patients on the heart failure register) on a quarterly basis for 12 months. Incident data and brief narrative descriptions were uploaded to a spreadsheet and reviewed by programme leaders (NH & JG) and the evaluation team (PB, LH & CdW). We jointly selected and agreed on a small core number of incidents that we judged to be highly important or indicative of recurring themes that would be of strong interest to others.
Threats to patient safety
The trigger review process helped to identify important risks to patient safety in medical records that may have remained undetected unless specific action was taken to screen for them (see Table 1). We readily acknowledge that most primary care clinicians will be acutely aware of the risks of harm associated with the threats that we highlight. However, it is arguably unlikely that many will have considered the real possibility that evidence of these threats might currently reside in their own records, or that their local systems may be at significant risk.
Selected safety incidents and threats identified by the trigger review process during the first 12 months of SIPC
Suggested recommendations
We believe it is possible that a significant proportion of general medical practices will find confirmatory evidence of at least one of the latent risks or undetected patient safety incidents that we highlight. The recommendations we outline in Table 1 to help mitigate these potential hazards can be implemented for the most part without additional training or resources using existing practice improvement systems (e.g. significant event analyses, team briefings and meetings, medication reviews, chronic disease audits and routine clinic appointments).
Proactively screening for each incident risk is a relatively speedy task and potentially offers practice teams important learning opportunities to make patient care safer. We would suggest that GP teams choosing to implement some or all of the recommendations will find it practically feasible, highly relevant to the safety agenda and educationally beneficial. For those who are inexperienced in this domain, participation in this type of exercise may be a first step in openly acknowledging the patient safety problem and beginning the process of building a safety culture within their team and organization.
Spectrum of patient safety incidents
The evidence thus far suggests that the typology of safety incidents and latent risks uncovered by structured reviews of medical records tends to differ in general terms from those highlighted by complaints, significant event analyses, proto-incident reporting systems, medicolegal claims, feedback from patients and other methods. There appears to be limited crossover in how these incidents and potential risks come to the attention of the primary care team. If we are to take patient safety seriously in primary care then perhaps a linked multi-method strategy may be necessary to make more sense of the spectrum of safety-related incidents that can and do occur. For example, previously undetected incidents highlighted by record review might necessitate a significant event analysis being undertaken by the care team to learn more about why this circumstance arose, or act as a necessary prompt to conduct a more orthodox criterion-based audit study to quantify the extent of the initial problem highlighted.
Evidence is emerging from SIPC pilot implementation sites suggesting that some GPs much prefer the trigger review approach over SEA and are in favour of one technique replacing the other (Lyn Halley, Personal Communication). We may need to educate the primary care team about the full spectrum of patient safety incidents that can occur in routine practice if only to counter the false impression that structured record review is a ‘magic bullet’ in patient safety improvement terms.
Wider application of trigger review
Given that trigger review of records is a key part of the Scottish Government's patient safety programme for primary care to be implemented nationally from March 2013, it makes sense that current GPs and future medical leaders have opportunities to learn about the technique and apply it in practice.
A core element of a planned pilot safety and improvement programme for general practice specialty training (GPST) in the West of Scotland Deanery is the expectation that GP trainees and their educational supervisors test out this approach to reviewing medical records to identify patient safety-related learning needs. The main aim of the pilot is to investigate the feasibility of applying the method in the specialty training environment and shed some light on the educational and improvement impact of such an approach. Similar pilot work is also planned around how trigger reviews can inform the GP appraisal system in Scotland.
Other than GP nurses, who have the same access to records as their medical colleagues, the potential for a structured review of records to be undertaken by other clinical groups (e.g. community pharmacists or community nurses) is predicated on the depth and completeness of the patient information contained in the records they hold and access. It is unclear whether there is enough information in the records to justify this type of audit approach.
Implementation challenges
A potential advantage of the trigger review approach in primary care compared to hospital settings is one of local ownership. In hospital care external reviewers (normally ward nurses or occasionally junior medical staff) are often deployed to measure and calculate rates of harm in the records under review using a proforma and ‘tick box’ method. Frontline hospital clinicians may lack ownership and a willingness to act on findings, while there is also concern about the robustness of the statistical method employed. 21,22 Whereas in the SIPC process it is applied (internally) by clinical reviewers to identify and make judgements on incidents of preventable harm – our experiences suggests that accurate and reliable measurement is too complex, although others may disagree – providing an opportunity for them to engage in the activity and identify problems and improvement opportunities in their own setting. Paradoxically, this goes beyond the complexities of measurement and may involve a greater degree of active reflection, cognitive input and team-working on the part of the primary care clinician - it may be more problematic to ‘teach’ this mindset than to instruct individuals on how to follow a tick-box protocol.
A number of other challenges are still to be resolved. Can ‘any' GP or practice nurse conduct such a trigger review? Early indications are that this may not be the case, as there appears to be varying ability to link individual triggers identified (Box 1) with sub-optimal care found in the record. In terms of training the relevant clinical workforce, how do we build the necessary capability to achieve a critical mass? So far, training has involved short awareness-raising sessions coupled with one-to-one teaching, which is clearly not sustainable on the scale required. A short e-learning module and train-the-trainer course options are under consideration, but these may not be sufficient either.
Similar to clinical audit and significant event analysis there will be variation in the standard of trigger reviews undertaken by clinicians. We may need to consider how best we can assess the quality of this activity and provide meaningful feedback. Also, if we assume that this approach is a valuable patient safety intervention, we need to research the benefit (if any) of ‘structured review’ compared to simply asking GPs and others to ‘openly review' electronic patient records without the use of predefined ‘high yield’ triggers. Finally, it is currently unclear but important to know what the opportunity cost and added value would be in terms of participating in this process compared with other patient safety-related activities.
Conclusions
As the trigger review process is adapted and further refined it is clearly evolving from its original ‘measurement’ purpose to a less contentious and potentially more informative method of identifying patient safety-related learning needs for the primary care team. Our early programme findings suggest that the review process is uncovering largely known but undetected adverse events and latent risks that are of high relevance to GP teams in the UK and elsewhere.
We acknowledge that our descriptive list of incidents and recommended actions is a limited technical device which only provides a potential means to discover these possible risks and adverse events, rather than offering concrete solutions to the issues identified. It is vitally important to recognize that successfully reducing some or all of the established risks goes well beyond unearthing local evidence that they exist, and will be heavily dependent on overcoming many of the socio-cultural barriers to learning and improvement prevalent in general practice and wider primary care. 23