
Abstract
Objective
To measure perceptions of Australian medical students and staff about whether key Learning Topics included in the National Patient Safety Education Framework (NPSEF) are being taught and what challenges to patient safety teaching are thought to be operating.
Methods
A cross-sectional survey of medical deans, educators and students was conducted in 2010. Twenty of twenty-one Australian medical schools participated. Using a five-point Likert scale, respondents rated whether patient safety topics were taught in their medical school and challenges to including patient safety in the curriculum.
Results
There were 2413 eligible responses: deans (or nominees) (n = 14); medical educators (n = 98); and medical students (n = 2301). There was most agreement that teaching occurred about communicating effectively (8% neutral or disagreed) and least agreement that there was teaching about adverse events and near misses (35% neutral or disagreed). Deans, educators and students responded positively about available champions and expertise and negatively to the curriculum being too full to include patient safety. There were consistent differences between the responses of the stakeholder groups (P < 0.0005 in a non-parametric test). Deans were more positive than educators, who were more positive than students.
Conclusions
Strong variability between perceptions of Learning Areas reveals opportunities for improvement in teaching about patient safety, especially in the area of recognizing and addressing adverse events and risks. Consistent differences across stakeholder groups reveal disparities in the perceptions of the teachers and their students. The results indicate targets for improving patient safety learning and closing the feedback loop between students and staff.
Introduction
Worldwide, more people die daily from iatrogenic harm in hospital than they do from HIV/AIDs or road traffic accidents. 1 Complex factors contributing to poor patient safety have been identified and strategies implemented to ameliorate these. 2,3 The education of medical students about patient safety is an important step in this context; it may influence the safety of healthcare through preparing future doctors, 4,5 and equipping medical students to act as important resources for error prevention while on placement. 6 Several undergraduate patient safety curricula have been implemented with variable success in changing medical students' knowledge of and attitudes toward patient safety. 5,7–9 Multiple challenges have been identified to the integration of new topics into already full curricula. 5,10
Studies examining the perspectives of medical students and graduates show that some lament a lack of preparation in aspects of quality improvement 11 and patient safety; 12 others consider these topics less important than traditional clinical content. 5 The lack of a champion advocate has also been shown to pose a barrier to the inclusion of topics in curricula. 10
The integration of patient safety into undergraduate medical curricula has proved challenging because of its relative novelty, which can leave medical educators unsure of how to best teach and assess quality and safety. 13,14 To address this challenge the World Health Organisation's (WHO) World Alliance for Patient Safety sponsored ‘the development of a universal patient safety curriculum guide for medical students worldwide’. 15 Development of the WHO Patient Safety Curriculum Guide (PSCG) was informed by the National Patient Safety Education Framework (NPSEF). 16 The National Patient Safety Education Framework is designed to provide a simple, flexible and accessible framework that identifies the knowledge, skills, behaviours, attitudes and performance required by all healthcare workers in relation to patient safety. 17 This tool incorporates seven Learning Areas, for a total of 22 Learning Topics. Teaching of patient safety, which can be either embedded in existing domains of teaching or as a stand-alone topic area, forms part of the accreditation standards for medical schools in Australia. 18
The aim of this study was to measure the perceptions of Australian medical school students and staff with regards to the teaching of patient safety. Gaps between the perceptions of students and staff, as well as variability between topics, can be used to identify current challenges in patient safety teaching and areas for targeted improvement.
Methods
Sample and design
A cross-sectional survey of medical deans (or their nominees), educators and students in Australian universities was conducted in 2010. Ethics approval was granted by the University of New South Wales Human Research Ethics Committee. Participants completed either an online or paper-based questionnaire. Questions were drawn from the 22 Learning Topics and seven Learning Areas in the NPSEF. 18 Participants were asked to indicate the degree to which they agreed that each Learning Topic was taught in their medical school. Four questions sought information on the best time to teach patient safety, and the availability of champions, expertise and space in the curriculum to do so. Participants were also asked if they knew about the tool.
Participants rated each question on a five point Likert scale (1= Disagree Strongly; 2 = Disagree Slightly; 3 = Neutral; 4 = Agree Slightly; 5 = Agree Strongly). Demographic data, including the medical school's name, participant's role and the number of years they had been in this role were collected.
Procedure
An invitation to complete the questionnaire was sent to the deans of all 21 Australian medical schools. Australian medical educators (n = 278) were emailed invitations to complete the survey through the Australian and New Zealand Association for Medical Educators (ANZAME) (now ANZAHPE). At one university, the medical school also chose to distribute an invitation to medical educators. The Medical Student Societies (MedSocs) disseminated invitations to participate to their members (19 universities) and there was a prize incentive associated with participation. At one medical school, the MedSoc representative requested that the School of Medicine distribute the invitation to participate to students. Multiple completions of the survey by the same person were restricted by preventing re-entry into the survey. A search for duplicate names or email addresses was conducted to identify respondents who attempted multiple entries. In the case of multiple entries, the first response was accepted.
Analysis
The analysis was an examination of the perceptions of patient safety learning amongst the stakeholder groups and the variation across the Learning Areas and Learning Topics. Kruskal-Wallis one-way analysis of variance by rank was applied to the Likert scale responses to determine which of the differences were significant. Other than comparing across the three stakeholder groups and the seven Learning Areas, students were compared according to their year-level to look for year-level differences that may explain the results.
Perceptions of challenges in teaching patient safety were determined by groups' responses to questions about the availability of a champion, expertise to teach patient safety and space in the curriculum as well as the best time to teach about patient safety, as were intergroup responses of deans, educators and students and student responses by year of medical school.
Results
Twenty Australian medical schools participated; one declined. Survey responses with duplicate email addresses or duplicate first and second names were removed (n = 85). A total of 2413 responses were included in the final analysis (14 deans or their nominees, 98 medical educators and 2301 medical students). The survey responses represent 13.7% of 16,807 students enrolled in the 20 medical schools that participated in the study. The response rate for deans or their representatives was 70%, and for medical educators (defined by membership of ANZAME), the response rate was 35%. The majority (92%) of respondents, that is, deans (54%), educators (71%) and students (93%) had not heard of the Patient Safety Education Tool.
Perceptions of current teaching
While the majority of students and staff perceived the 22 Learning Topics were being taught in their own medical schools, there was clear variation between the stakeholder groups and across the Learning Areas. In Figure 1, the responses to the Learning Topic questions are illustrated in order, from least positive to most positive. The responses are aggregated for all the stakeholder groups.

The proportions of agreement for the 22 Learning Topic questions for all stakeholder groups. The bars represent the percentage of responses that were Disagree Strongly, Disagree Slightly, Neutral, Agree Slightly, and Agree Strongly (from left to right). Ordering of Learning Topics is from least positive to most positive (top to bottom)
Differences between stakeholder groups and years of enrolment
There were differences between stakeholder groups in their responses to the questions (P < 0.0005). Of the three groups, the deans responded most positively, followed by the educators and then students. The differences between stakeholder groups are illustrated in Figure 2. The interquartile ranges are indicated by the grey bars and the individual responses averaged over 22 questions are also illustrated. When comparing medical students by year, no significant difference was found (P = 0.20) between 448 first years, 551 second years, 449 third years, 389 fourth years, and 462 students in fifth year or above; two students did not provide the number of years they had been enrolled.

The differences across the target groups and the year-levels of students illustrated using mean responses by individuals. Each participant's mean response (22 questions) is indicated by a dot. The interquartile ranges are illustrated as grey bars
Variation across and within Learning Areas
Perceptions varied between Learning Areas, with fewer indicating positively that they perceived Managing Errors, Adverse Events, Risk and Complaints being taught, and a greater proportion indicating that they believe the Communicating Effectively Learning Area was being taught in their medical school (Figure 3). Comparison across Learning Areas (including all stakeholders' responses) showed a significant difference in the perceptions of the Learning Areas (P < 0.0005). Deans, educators and students gave significantly different responses in six of the seven Learning Areas (only Using Evidence and Information produced no significantly different result between the groups).
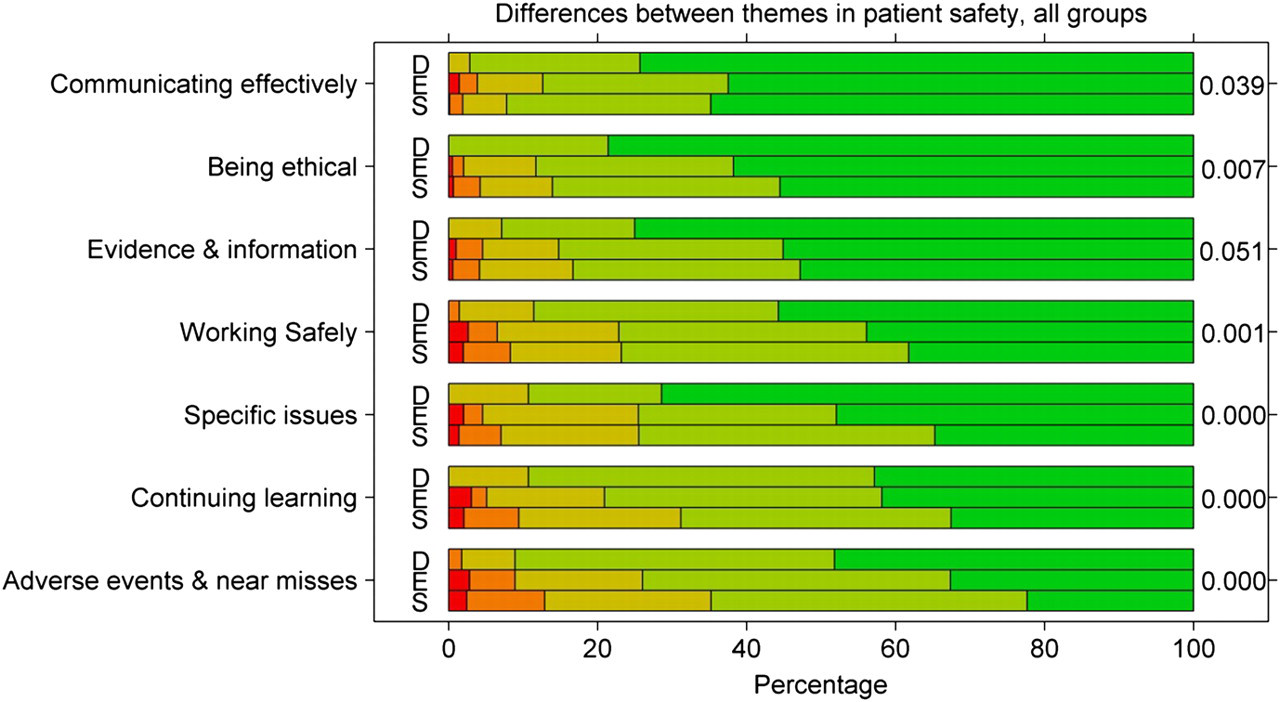
The proportions of agreement by Learning Area, and by stakeholder group illustrated as a series of bars. The Students, Educators and Deans are labelled S, E and D respectively, and the bars represent the percentage of responses that were Disagree Strongly, Disagree Slightly, Neutral, Agree Slightly, and Agree Strongly (from left to right). The order of the themes (top to bottom) is by mean rank from most positive to least positive, and P values are indicated for the level of agreement across target groups for each of the seven Learning Areas (right)
Perceptions of challenges to teaching patient safety
Respondents held that there was a champion available for teaching patient safety (agreement = 49.4%; disagreement = 14.2%; neutral = 36.5%) and staff with expertise in teaching patient safety (agreement = 65.9%; disagreement = 7.4%; neutral = 26.7%). There were significant differences between the responses given by deans, educators and students to these questions (P < 0.0005 in both cases) (Figure 4), with deans more likely to agree or strongly agree with these statements than educators or students.
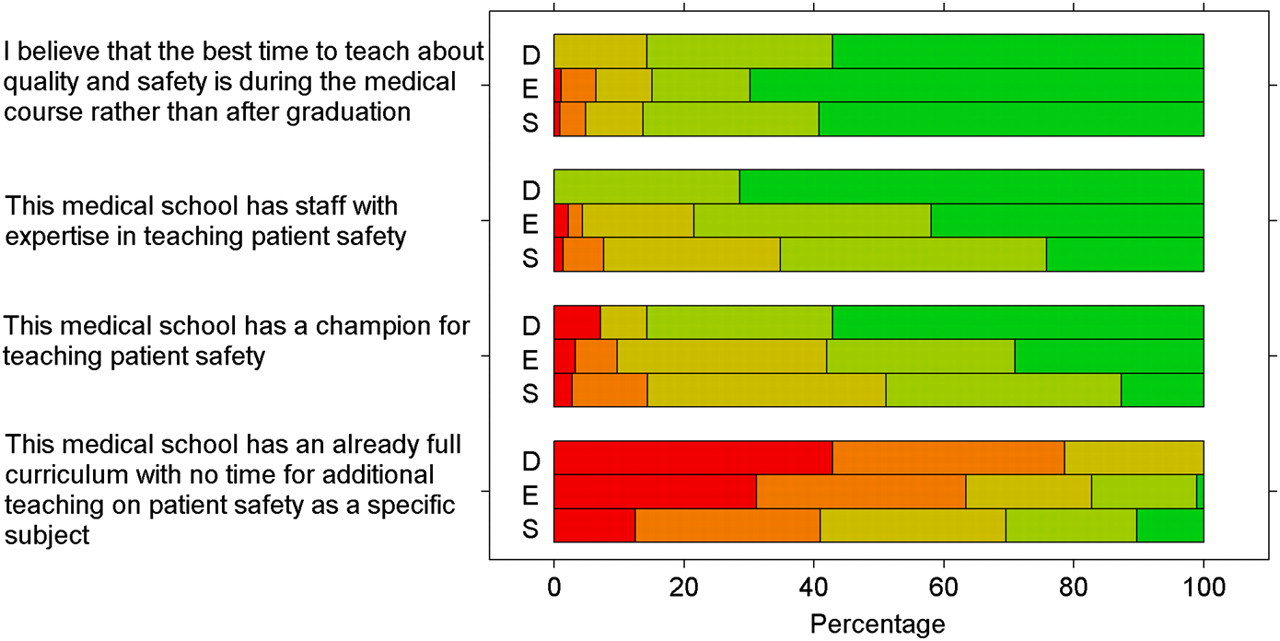
The differences between stakeholder groups for the four questions relating to challenges to inclusion of patient safety. See Figure 3 for the key
There was overall disagreement with the statement that the curriculum was too full to incorporate additional patient safety teaching (disagree or strongly disagree = 41.8%; agree or strongly agree = 29.9%; neutral = 28.2%). There were significant differences between the three groups, with deans and educators more likely to disagree that the curriculum was already full, with no time for quality and safety (P < 0.0005). Each of the stakeholder groups agreed that the best time to teach quality and safety was before graduation, with no significant differences between the groups in response to this question.
Discussion
There are gaps between what students believe they are being taught and what medical educators and deans believe they are teaching. In addition, a greater proportion of the members of medical schools in Australia believe they are learning or teaching about Communicating Effectively and Being Ethical, and fewer believe they are learning or teaching about Managing Errors, Adverse Events, Risks and Complaints, and Continuing Learning. It is acknowledged that components of the National Patient Safety Education Framework may be embedded in routine and practical teaching, or as stand-alone topics, or both. The survey encompasses all three possibilities. However, regardless of whether some topics are taught in a less explicit manner or have become more embedded in the curricula over time, the differences provide a valuable opportunity to address risk in this domain through targeting these specific gaps and improving patient safety learning in Australian medical schools. We note that the majority of respondents had not heard of the Patient Safety Education Tool which might suggest a lack of awareness of the National Patient Safety Education curriculum. Despite this, this survey shows that the Learning Areas described in the NPSEF are perceived to be taught.
Differences between stakeholder groups
While each group tended to agree that patient safety is being taught, there were considerable gaps in the perceptions of deans, educators and students. Similar examples of between-group differences are offered in the literature in relation to: attitudes to aspects of patient safety; 19 perception of presence of attributes of professionalism; 20 and perceived educational needs. 21 In another study, there is evidence of alignment in educators and students' perceptions of student experiences. 22
We found that educators and faculty leaders agreed more often than students that patient safety topics were being taught in their own medical school. This may be a consequence of having more information and experience with the curriculum and its history, or it may reflect a disparity between what is believed to be taught and what is actually learnt. Regardless of the explanation, the divergence identified in the results provides an opportunity to reduce the gap between student and staff perceptions by making learning objectives more explicit.
Differences between Learning Areas
The Learning Area Managing Errors, Adverse Events, Risk and Complaints received the greatest proportion of negative responses from students and staff. While there is evidence of effective integration into some patient safety curricula, 23 studies continue to identify gaps in students' understanding of aspects of medical error. 24
A plausible explanation for differences between Learning Areas may come from how established the Learning Areas are in the Australian curriculum. For example, the importance of effective communication on the quality of healthcare has long been acknowledged, with a growing literature on patient-doctor communication and methods for teaching communication. 25 The Learning Area Communicating effectively received the most positive responses. However, Communicating honestly with patients after an adverse event (open disclosure) was the sixth most positively rated Learning Topic. This is noteworthy given identified gaps in trainees' appropriate disclosure practices in the literature. 26
Challenges to inclusion of patient safety in the medical curriculum
An already full curriculum has been identified as a barrier to the inclusion of new topics. 10 In contrast we found that respondents rarely believed a crowded curriculum was an obstacle to patient safety education. Deans and educators felt that patient safety was an important inclusion but students were largely grouped around the neutral response to this question. The greater tendency of students to respond neutrally may reveal uncertainty about the logistics and implications of having to cover more during their degree.
The instrumental role that local champions play in advocating for change and implementing initiatives has been acknowledged in both clinical and educational areas within healthcare. 27 Our respondents supported the view that there was a champion for, and staff with expertise in, teaching patient safety at their school. Deans were significantly more likely to agree with this proposition than educators who in turn were more likely to agree than students. This may signal a lack of information about what expertise in teaching patient safety entails or an inability to identify who the champion might be. Champions advocate their cause to those who can influence change, in this case their colleagues and the Dean. The student body may not be party to such negotiations, nor witness the process. Faculties should identify local champions to help address the difference between the ‘rhetoric’ expressed by the deans and the ‘reality’ as reported by the students.
Limitations
Relatively low response rates were a limitation of the study. Although we have no reason to believe there may be an unreported bias, the response rates of students and staff may produce bias along dimensions that were not measured during the survey.
The survey was not piloted, which is a limitation because there may be questions in the survey for which the specific jargon used does not correspond to the jargon used in the curriculum throughout medical schools in Australia. While this is a limitation of the study, using the NPSEF as a basis for the wording of questions was deemed appropriate considering that accreditation of Australian medical schools requires that new medical graduates have ‘the skills needed to work safely as an intern, as outlined in the National Patient Safety Education Framework developed by the Australian Council for Quality and Safety in Health Care’.18:3
Conclusion
We have identified significant variability in the perceptions of patient safety teaching in Australia between NPSEF Learning Areas, and between students and staff. We recommend an increased focus on identifying, preventing and managing adverse events and near misses, which may benefit from being made more explicit in the curriculum, as a risk management strategy. While different vantage points of the curriculum, as a whole, offer one explanation for significant differences between stakeholder groups' perceptions, the recognition of this gap provides opportunities to address it in a targeted manner.
Footnotes
Acknowledgments
We gratefully acknowledge the assistance of Professor Ian Wilson in facilitating the distribution of the survey to ANZAME (now ANZAHPE) members and the MedSoc representatives in facilitating the distribution of the survey to medical students. We are grateful for the enthusiastic response of the medical deans, educators and students who participated in this project and for the comments of anonymous reviewers.