
Abstract
This article is an overview of current/evidence-based practice for Induction of Labour (IOL) in the UK. The indications for IOL, risks, benefits and common mistakes with reference to breach of duty are discussed.
Introduction
Induction of labour (IOL) is the process of artificially attempting to expedite the delivery of a baby when the risks of continuing a pregnancy outweigh the benefits. IOL is relatively common; approximately 20% of all deliveries in the UK are induced. 1 IOL carries significant risks to both the mother and baby; therefore, the decision to induce labour should be clinically justified. Induced labours are less efficient and more painful than spontaneous labours, with a doubling of women requiring epidural anaesthesia and an increase in instrumental deliveries and emergency Caesarean sections (CSs). 1 Less than two-thirds of induced labours will result in normal vaginal deliveries, with 15% operative instrumental delivery rate and 22% women requiring emergency CS. 2
The decision for IOL should not be taken lightly. When offering IOL, the reasons should be clearly explained including risks/benefits. Alternative options, where safe, should be discussed/documented if the woman chooses to decline induction. Where and when the induction would be performed should also be discussed, as well as the proposed induction methods, the monitoring required and the fact that induction may not be successful.
The current accepted practice is to obtain verbal consent for IOL. There is a small but increasing consensus that written consent should be obtained before proceeding with IOL, to ensure full understanding of the risks involved.
There are many different indications for IOL, both fetal and maternal, and some of these are discussed below.
Prolonged pregnancy is the most common reason for IOL
Compared with expectant management (i.e. allowing pregnancy to continue beyond 42 weeks), IOL after 41 completed weeks of pregnancy is associated with fewer perinatal deaths. 3 Evidence also suggests that there is a reduction in the number of emergency CS required with IOL between 41 and 42 weeks gestation when compared with expectant management. 4 Women with uncomplicated pregnancies should be offered IOL between 41 and 42 weeks of pregnancy. Due to the increased risk to both mother and baby, failure to offer IOL between 41 and 42 weeks would represent a breach of duty.
Those who decline induction should be offered increased fetal monitoring, for example, twice/thrice weekly cardioto-cograph (CTG) and amniotic fluid measurement by ultrasound scan until labour establishes. The risk of stillbirth increases from one per 3000 ongoing pregnancies at 37 weeks to three per 3000 at 42 weeks and six per 3000 at 43 weeks. 5 There should be careful documentation that the risks have been fully explained if a patient decides to proceed past 43 weeks of pregnancy.
Prelabour Rupture of Membranes at Term
When rupture of membranes occurs prior to labour, but after 37 weeks of pregnancy, women should be offered the choice of IOL or expectant management. It is appropriate to offer IOL approximately 24 hours after rupture of membranes, as within this time period 60% of women will go into spontaneous labour and avoid the risks associated with induction. 6 Women should be informed that expectant management carries a risk of infection and sepsis for both the mother and the baby.
Preterm prelabour rupture of membranes
If a woman has preterm prelabour rupture of membranes after 34 but before 37 weeks, the timing of induction of labour should be individualized for each patient, balancing the risks of sepsis from continuing the pregnancy versus prematurity if inducing before 37 weeks. With improving SCBU/Paediatric support the trend is towards IOL thus avoiding the risk of infection. In many cases steroids are given to aid fetal lung maturity with antibiotic cover for mum followed after 48 hours by IOL.
As each case must be individualized for the 34–37 week gestation, substandard care around such a decision is likely to be hard to prove, both options being reasonable.
Maternal medical condition, for example, pre-eclampsia, diabetes
All patients with diabetes should be offered routine IOL due to the increased risk of stillbirth. The gestation at IOL depends on the type of maternal diabetes. Failure to offer IOL in these women would represent a breach of duty. National and often local guidelines should exist on all units dealing with the care of diabetic women and IOL. Continuous CTG monitoring is mandatory once labour is established.
In women with moderate or severe pre-eclampsia, a condition which only improves following delivery IOL may be necessary to protect the mother's or fetal health. In severe cases of pre-eclampsia, IOL may be necessary even at very premature gestations. These are high-risk pregnancies, and continuous CTG monitoring is mandatory once labour is established.
IOL for Fetal Concern
If a decision has been made to deliver a baby early due to concerns about fetal wellbeing, then consideration should be given to the most appropriate mode of delivery. It may be appropriate to induce the labour of a baby who has mild/moderate growth restriction with no other signs of compromise. However, a severely growth-restricted baby with low liquor volume and Doppler blood flow abnormalities (early signs of compromise/ hypoxia may not tolerate labour) often should not be induced or IOL with caution. A lack of clear documentation/continuity of care on the management of such IOL from senior clinicians is a common finding in litigation. These babies are very likely to develop hypoxia, during hours of contractions leading if unchecked/inadequate CTG monitoring to acidosis in labour. While there is no reliable test to predict the response to IOL of such fetuses, in most cases of severe intra uterine growth retardation (IUGR) an elective CS is the correct option. It is rare; however, the decision to attempt IOL that directly causes hypoxia BUT the failure to manage the subsequent labour as high risk from the start. This requires a lower threshold for intervention with early use of fetal blood sampling and CS for CTG abnormalities as these fetuses are less able to withstand the stresses of labour.
A few examples of inappropriate reasons for IOL from National Institute for Health and Clinical Excellence
Suspected macrosomia (large for gesational age baby)
Macrosomia is defined as a baby with a birth weight greater than 4 kg. In the absence of another indication, IOL should NOT be carried out simply because the obstetrician suspects that a baby is large for its gestational age. 1
History of precipitate labour
IOL should NOT be offered to avoid a birth unattended by healthcare professionals. 1
Maternal request alone is not an acceptable indication, except in exceptional circumstances
Many women request IOL. Reasons vary from convenience to pain/discomfort. While reasonable opinion varies, arranging IOL (at or after 40 weeks) to enable the partner to be present at birth is acceptable, for example, husband in armed forces and only granted 1-week leave around the estimated delivery date.
Doctors may still offer IOL in such cases, whether this represents substandard care will depend partly on the individual case and on whether documentation that the risks and benefits have been discussed with the patient/couple. While good documentation is not common place, it should be remembered that few patients will decline the offer for IOL!!
Complications
Hyperstimulation
There are many complications associated with IOL. The pharmacological agents used in the induction process may cause the uterus to over contract (greater than 5 contractions in 10 minutes or a single contraction lasting greater than 2 minutes). Such hyperstimulation is usually clear cut, easy to measure and is less often open to interpretation by experts as much as fetal heart rate decelerations.
Vaginal prostaglandins (PG) carry a risk of uterine hyperstimulation which varies between 1% and 5%. 1 They should therefore be used with caution in women who have had a previous CS.
Uterine hyperstimulation may lead to fetal heart rate abnormalities. These heart rate abnormalities are reversible in over 98% of cases if 250 μg of terbutaline (a tocolytic drug) is administered to the mother. 7 CTG improvement usually begins within 5 minutes regardless of hyperstimulation patterns. 7 Failure to use such tocolytics for CTG abnormalites resulting from hyperstimulation would represent a breach of duty.
Cord Prolapse
During the IOL process an attempt will usually be made to perform an artificial rupture of membranes (ARMs). Umbilical cord prolapse may occur at the time of (ARM). To try and avoid this, an assessment of the engagement of the presenting part should be made prior to ARM. ARM should be avoided in the presence of an unengaged head. Further PG or delay ARM/ encourage patient to be upright should be offered.
Failed IOL
If IOL fails, the condition of the woman and baby should be reassessed by a senior clinician. Options for further management should be discussed with the patient. Management options are dictated by the indication for IOL. With significant fetal or maternal concerns a CS will be considered, where less concern a further attempt to induce labour (following a rest period of 24 hours) may be offered.
Uterine rupture
Uterine rupture is a catastrophic event with associated high maternal and fetal morbidity and mortality. It is the most dangerous complication associated with IOL.
Uterine rupture may occur with little warning or substandard care; however, rupture following IOL should be carefully reviewed. The attending clinicians were aware of the IOL and the scarred uterus, that is, these are very high-risk pregnancies, following scar rupture litigation is common.
If uterine rupture is suspected then the baby should be delivered immediately by CS. The classical signs and symptoms of uterine rupture include CTG abnormalities, loss of uterine contractions, abdominal pain, vaginal bleeding and recession of the presenting fetal part.
Previous CS and IOL both increase the risk of uterine rupture. Previous CS is not an absolute contraindication to IOL but the increased risk should be carefully assessed in each case by a senior clinician and consultant input is mandatory. Current range of opinion on IOL with previous CS, some consultants will not consider IOL and elect for CS. Others especially if the patient has a vaginal delivery before or after the prev CS will be more comfortable with IOL. The two best predictors of success are a high Bishops score (see below) and previous vaginal delivery.
All patients with prev CS being induced should be monitored very closely throughout their labour with continuous CTG. Any CTG abnormality on monitoring should prompt urgent medical review/delivery by CS.
The induction process
In order for labour to be successful, first the cervix must undergo a process called ‘ripening’ which involves it softening, shortening and starting to open. Cervical ‘ripeness’ can be assessed using the Modified Bishop Score (see table).
Modified Bishop Score. 8

A cervix which is more ‘ripe’ or ‘favourable’ (e.g. soft, already dilated) will achieve a higher bishop score, while a cervix which is ‘unripe’ or ‘unfavourable’ (e.g. long, hard, closed) will result in a much lower score. The lower the Bishop Score, the harder it will be to bring about the changes required for successful labour.
Method of IOL
There are various methods for IOL, including a sweep of membranes, vaginal prostaglandins (PGs), amniotomy (ARM) and intravenous oxytocin infusion (syntocinon). Sweeping of membranes has been used as a method for ‘inducing’ labour for at least the last 200 years. 9 Whether or not a sweep of membranes is an attempt at IOL is controversial. A cervical sweep is offered to women by their midwives and is usually performed in the community. A cervical sweep very rarely leads to fetal compromise and no fetal monitoring is required. The National Institute for Health and Clinical Excellence (NICE) regard membrane sweeping as an adjunct to IOL rather than a method for IOL. 1
Vaginal PG is the preferred method for IOL in the UK, unless there are specific clinical reasons for not using it (e.g. previous uterine hyperstimulation). Alternative routes of administering prostaglandins, such as oral, intravenous, intra cervical or extra amniotic, should no longer be used for IOL, 1 such use other than exceptional cases represents a breach of duty.
Prior to PG use fetal wellbeing must be confirmed by a normal CTG. ACTG records both the fetal heart rate and the uterine activity and is interpreted in the UK according to NICE guidelines. There are four features that are considered when interpreting CTGs and all these need to be normal prior to commencing IOL (see below). Continuing with IOL with a non-re-assuring CTG represents substandard care.
Once fetal wellbeing has been confirmed, a cervical assessment is performed using the Modified Bishop Score. Vaginal PGs are used to improve cervical ripeness and are usually given on a ward or delivery suite. The recommended regimen is as follows:
1
One cycle of vaginal PG tablet or gel – one dose followed by reassessment of cervix after 6 hours and a second dose if required (followed by further reassessment 6 hours later). One cycle of controlled release pessary – one dose over 24 hours.
The aim is to achieve a favourable cervix which will allow an ARM. Following ARM, a syntocinon infusion may be commenced if adequate contractions have not commenced naturally. Timing of syntocinon use after ARM in IOL depends on parity (i.e. whether the mother has delivered a baby before). It is usually started 2 hours from ARM in a multiparous woman if adequate contractions have not started, or 0–2 hours from ARM in a primiparous woman. While NICE does not recommend the use of ARM and syntocinon infusion alone to induce labour, this is still an accepted practice in widespread use as an induction method when the cervix is favourable.
Syntocinon is given as an intravenous infusion to increase the frequency and force of contractions as part of the IOL process. Syntocinon should not be used within 6 hours of vaginal prostaglandin insertion because of the increased risk of uterine hypertonus. Continuous CTG monitoring is compulsory with any use of syntocinon. The documentation of the amount of syntocinon used is extremely important. Syntocinon should be used with caution in multiparous women due to the increased risk of uterine rupture.
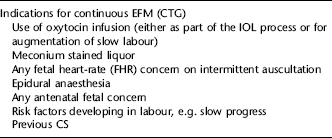
Once regular contractions have commenced, it is necessary to commence a CTG to confirm fetal wellbeing. Following a normal CTG, intermittent auscultation can be used to monitor the fetus, unless there are reasons for continuous electronic fetal monitoring. Some indications for continuous monitoring are shown in the table. The CTG needs to be continuously reviewed by the midwife and any concerns should prompt senior midwifery and/or medical review.
Common themes of syntocinon resulting in fetal compromise/litigation
Increasing oxytocin despite reasonable progress. Increasing oxytocin when contractions are adequate –3–4 in 10 minutes. Using oxytocin with previous CS. Starting oxytocin when CTG not normal. Failure to half or stop oxytocin if CTG abnormal.
Interpretation of CTG. 6

CTGs are assessed using the four criteria explained below, and are then classified into one of three groups.
A CTG should not be interpreted in isolation; the whole clinical scenario needs to be taken into account. In the presence of other risk factors such as a previous CS, pre-eclampsia or a growth-restricted baby, early changes in FHR pattern should raise concern.
Classification of CTG. 6
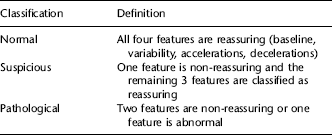
If a CTG is classified as pathological it should prompt either immediate delivery or fetal blood sampling to confirm fetal wellbeing. Delays in recognizing the signs of suspected fetal compromise and/or acting upon them may mean that infants require prolonged resuscitation at birth and may develop hypoxic–ischaemic encephalopathy. This may lead to an increased risk of subsequent cerebral palsy and longterm neurological impairment.
Both national and regional audits have shown that rates of substandard care are high in cases of intrapartum fetal death. In three audits performed in the UK, between 40% and 75% of cases were found to have a significant or major suboptimal care factor.10–12
In the Seventh Confidential Enquiry into Stillbirth and Disability in Infancy more than 75% of cases had evidence of poor care. The most common time for suboptimal care is during labour (70%) and the most common error is the use and interpretation of CTG. 13
Summary
The decision to induce labour is a balance of the risks of IOL to those of continuing the pregnancy. All pregnancies induced other than at 42 weeks should be considered increased or high risk with a reduced threshold for intervention. Failure to recognize this ‘increased risk’ is a common contributor to birth injury/litigation.