
Abstract
There is a need for new approaches to supplement the existing methods of taking research from bench to bedside and from bedside to practice. Community-based participatory research (CBPR) is an emerging model of research that enhances ongoing clinical research by involving key stakeholders, including community members and patients. A practice-based research network (PBRN) is a group of primary care practices devoted principally not only to the primary care of patients, but also with a mission to investigate questions related to community-based practice and to improve the quality of primary care. Traditionally, PBRN research has not included patients or community members, while CBPR has excluded health providers as key stakeholders. Typical overlap topics of PBRN and CBPR research are health-care disparities, prevention, chronic disease management and mental health. The inclusion of CBPR within a PBRN has been identified as an important next step with the potential to significantly enhance the research process. This review focuses on bringing together the ideals of CBPR and PBRNs in order to tackle intractable problems such as disparities in health-care access and outcomes and translate these results into practice. Specifically, the CBPR PBRN approach can: (1) guide the research process so that studies more closely match the needs of all stakeholders (including providers, patients and community members); (2) assist in the development of the research protocol and identification of research methodologies so that the study is more amenable to participants; (3) facilitate recruitment of research participants; (4) enrich the data collection and analysis; and (5) allow rapid translation of results from the study back into clinical practice and the community. Once these mechanisms have been clearly elucidated, their widespread adoption will positively impact overall health at both a local and national level.
Introduction
Concerns about the gap between science and medical practice are longstanding. In its landmark indictment of the quality of health care in the USA, in 2001, the Institute of Medicine commented that many proven effective treatments do not become incorporated into everyday care. 1,2 Research findings take an average of 17 years to filter down to practice, and in 2003 the National Institutes of Health (NIH) responded by increasing the emphasis on translation of research into practice by establishing new research networks as a major step in NIH's roadmap for re-engineering the clinical research enterprise. 3 Clinical research is often performed in controlled academic research centers where results are not directly applicable to patients or physicians. The NIH initiative builds clinical research at the primary point of contact between patient and the health-care system. Primary care physicians striving to practice evidence-based medicine are frequently hampered by a lack of evidence to apply to the problems of everyday practice, resulting in dissatisfied patients and providers and prevents optimal health outcomes. 2 The Agency for Healthcare Research and Quality (AHRQ) is a federal agency designateed by law to conduct primary care research. In 2000, Congress asked the AHRQ to identify and support primary care practice-based research networks (PBRNs) as a resource for accelerating the translation of research into practice. Translation of basic and clinical research into improved health allows NIH to recognize the value of primary care research networks. 4
Community engagement has also become a major contributor to medical research during the past 10 years and has become an essential component of the current NIH Roadmap and the Clinical and Translational Science Awards program. 5,6 In the words of NIH Director Elias Zerhouni, ‘as disease burden has shifted from acute conditions to chronic conditions primarily seen in community rather than tertiary centers, new approaches for forging relationships with local and regional community partners will become increasingly critical’. 7 Recognition of the importance of community engagement in the biomedical research process has begun to open up new channels for funding. 8 Figure 1 shows a timeline of growth of PBRNs and the development of the PBRN with community-based participatory research (CBPR) interaction.
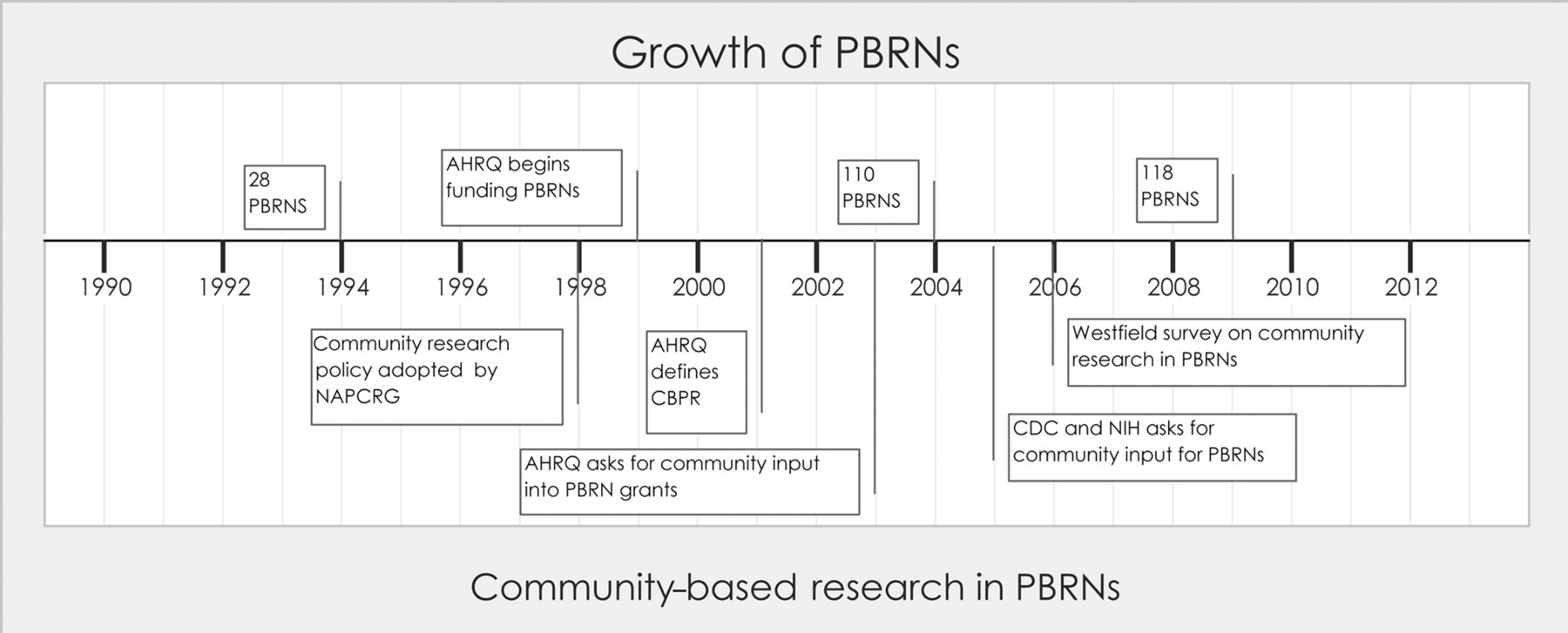
Timeline showing the growth of practice-based research networks (PBRNs) and significant milestones of community-based participatory research (CBPR) within PBRNs. AHRQ, Agency for Healthcare Research and Quality; CDC, Centers for Disease Control and Prevention; NIH, National Institutes of Health; NAPCRG, North American Primary Care Research Group
This review briefly describes the background and development of PBRNs and CBPR and the ways in which they currently function and are envisaged to blend in the future. Typical topics of PBRN research are health-care disparities, prevention, diabetes, hypertension/cardiovascular risk and mental health. 2,9 CBPR, which often has a more local, community-driven focus, addresses research topics such as: environmental hazards; hypertension/cardiovascular; diabetes/human immunodeficiency virus/acquired immunodeficiency syndrome/asthma; prevention; cancer screening; substance abuse; occupational health; women's and seniors' health; disabilities; end of life care; and mental health. CBPR is a research method that focuses on equal partnerships between researchers, clinicians and community members in the research process. In order to demonstrate both potential and actual research overlap between CBPR and PBRNs research, examples will be given of a few common types of research from both PBRNs and CBPR, and also studies where community is already a large component of PBRN research. A discussion of ways to set up a PBRN with community infrastructure then follows.
This review was based on a search of PubMed, Ovid and Google using search terms around Community-Based Participatory Research and Practice-Based Research Networks. CBPR and participatory research were used as MeSH terms within PubMed, and related links were also examined. This literature search was not intended to represent an exhaustive literature survey or systematic review, but rather was based on identifying key research papers that demonstrated how the two fields can be connected and research successfully implemented.
Community-based participatory research
CBPR is an emerging model of research that enhances the relevance and value of ongoing clinical research by involving patients and key stakeholders, including community members. 10 CBPR is a mechanism for improving community health, effecting social change and ameliorating health disparities within disadvantaged communities. 11,12 Equally important goals of CBPR include benefiting the community where the research is taking place and developing valid knowledge that is applicable to other settings. 13,14 In traditional research, academics determine study design and decide how outcomes are used in isolation. In contrast, CBPR is based on shared ownership of the research process as well as shared decision-making. Through commitment to action, CBPR has the potential for improving the health of large numbers of people beyond the partners involved or the target populations. 10 CBPR can employ a wide range of methodologies, 15 but key principles include: fostering trusting relationships with all partners; building on strengths and resources within the community; promoting co-learning and capacity building; utilizing equitable processes and procedures; using cyclic and iterative processes to develop partnerships; disseminating results to all partners; involving key stakeholders in all aspects of the research; and ongoing partnership assessment and improvement. CBPR methodology increases the likelihood of successful implementation because communities are already invested in the research process. 16,17 Sustaining CBPR can be difficult due to barriers such as lack of time and resources, sharing reduced resources and maintaining morale through funding uncertainties. To overcome these challenges, a collaborative approach is essential, involving recognition of the inherent value of all partners' perspectives, fostering open communication, development of shared history and goals with honest exchange of ideas and conflict resolution. Long-term commitment and having organizations as partners rather than individuals allows commitment to be sustained. Champions are long-term members who serve as significant contributors by staying power, facilitating relationships and serving as spokespersons. New relationships need to be built to sustain the partnerships. Partners need to experience personal, organizational and community benefits in order to stay engaged. 18,19
The most basic component of a CBPR process is partnership formation. Research partnerships range across a continuum with partnerships initiated and driven by communities at one end and collaborations initiated and controlled by universities at the other. 15 Methods for forming CBPR – academic partnerships for research projects – are well documented. In one study looking at obesity disparities in native populations, researchers began by recognizing a need to develop academic–community partnerships that aim to achieve balance between ‘scientific rigor and community wisdom’. 20 In order to develop trust, key elements had to be addressed: first, the partnership began with community organizations and academic researchers who had previously collaborated and were interested in research. The authors note that for successful collaborations to proceed, academics should consider the community's attitude towards scientific research, particularly towards mistrust of the intentions of the academic researchers, and collaborations should serve the communities that experience the health disparity they are addressing. They created a guideline/information document to provide a framework for operations and dispute solving. For example, during the experimental design phase, one dispute was that the community felt that no participant should be denied an effective intervention imposed by randomized control experiments. Balance was achieved by giving all study participants a diabetes prevention program for weight loss, then hypothesis testing on the follow-up by randomized participants to either a maintenance program or standard of care phone call. The community partners felt invested in the success of the project by their level of responsibility. For example, community was responsible for collecting and maintained data with only de-identified data given to researchers. 20
CBPR in health-care disparity research
Disparities research is evolving from observation or documentation to understanding causes and mechanisms, to conducting interventional research to reduce or eliminate disparities. 21 Disparities research must be conducted in partnership with communities to ensure that the interventions are community responsive and that the interpretation of results resonates within the targeted community. 21 Disparities are often driven by three factors: multiple risk factors and co-morbidities of patients; inconsistent application of practice guidelines by health-care practitioners due to a limited evidence base for minority and under-served populations; and barriers in the health-care delivery system resulting in poor access to care. 22
For example, rural Hispanics' perceived barriers to accessing and utilizing health care were limitations in health insurance coverage, high costs of health-care services, communication issues involving patients and providers, legal status/discrimination and transportation concerns. 23 Barriers to timely and effective cancer care among Native American cancer patients compared with white patients found more negative attitudes toward cancer treatment, higher rates of advanced-stage disease at time of presentation, lower levels of basic cancer screening knowledge and more negative attitudes about cancer treatment. 24 The authors suggest that these disparity barriers could be addressed using multiple educational and health service delivery policy-related interventions that consider the vulnerable nature of under-served and ethnic populations.
CBPR in prevention research
CBPR was established to focus on developing new interventions and moving proven interventions into practice to reduce disease burden and disparities, especially among minority and under-served populations. One network uses the methods of CBPR in areas including primary prevention of cancer through healthy eating, physical activity, sun avoidance, tobacco control and early detection of cancer through screening. Initial foci for the network were increased screening for breast, cervical and colorectal cancers; to promote informed decision-making for prostate cancer screening; and to validate educational materials developed for low-literacy populations. 25 The Network methodology of bringing together the Latino community with the scientific community increased the level of awareness of cancer in the Latino community. 26
CBPR in diabetes research
One 10-year study involved CBPR for providing community-based diabetes management for a native population with diabetes. A randomized control study using a culturally tailored algorithm of evidence-based disease strategies for diabetes management was initiated. This chronic disease management model utilized a trained multidisciplinary home and community care team and results showed improved outcomes. 27
CBPR in hypertension/cardiovascular research
Overweight and obesity, lack of exercise and exposure to tobacco smoke are clearly identified behavioral risk factors for cardiovascular disease. These problems disproportionately affect some communities.
A major study of using community participation to improving health outcomes was designed to reduce adverse cardiovascular outcomes in the North Karelia region of Finland. This project was initiated in 1972 in response to requests from the population to address high levels of coronary artery disease. A comprehensive, community-coordinated intervention was developed to address multiple cardiac risk factors. Blood pressures and cholesterol levels declined community wide, and cardiovascular mortality declined by 75% over 25 years. 28,29
To address problems within one community of under-served Latinos, CBPR was used to design an outreach program involving Latina lay health advisors from the community to teach three classes on healthy nutrition, physical activity and maintaining smoke-free environments. Classes were offered in Spanish to adult Latinos recruited through social networks. A questionnaire on lifestyle behaviors was completed at baseline and one month following the last class. Findings supported using lay health-care workers as a feasible and effective health-care delivery strategy for cardiovascular community health promotion, especially among immigrant populations. 30
CBPR in mental health research
Translating evidence-based mental health interventions into community practice through partnerships between academic and public institutions is a goal of mental health researchers. To improve care for middle-aged and older adults with schizophrenia, one study developed a collaboration between a university research center and a public mental health service system incorporating CBPR and cultural exchange theory. The partnership developed an infrastructure to support research, educational programs and the development of the mental health delivery system. In one project they analyzed mental health service use by clients whose care was transferred to other programs. This project not only provided information that was important for county planning purposes, but it also demonstrated the partnership's ability to evaluate outcomes of a system-wide change in services. 31
Other community research mechanisms
Community-oriented primary care (COPC) bridges the gap between primary care and public health to evaluate and improve the delivery of health care to identified populations. This process was developed to improve access to care for third world countries and likely served as a precursor to CBPR, but can now be used to compliment the CBPR process. 32 The original description of COPC is lacking in community involvement as equal stakeholders. It involved a four-step process: (1) defining and characterizing the community; (2) identifying the community health problems; (3) developing emphasis programs; and (4) monitoring the impact of program modifications. Individual elements of the model may be useful when applied collaboratively with the community. There is little evidence for or against the effectiveness of the COPC methodology as originally described and limited utilization in actual practice. Methods involving community participation in COPC were added later. 32 One study using COPC methods applied to the management of cardiovascular risk factors involved the practice taking responsibility for both community and clinical functions and holding itself accountable to the population served through such means as patient committees, annual reports and meetings. In this study mortality was compared between two neighboring villages; the age standardized mortality ratio was found to be lower in the intervention community than in a neighboring village with similar demographics. The available data were consistent with the hypothesis that whole population care helps reduce mortality. 33,34 COPC has been used to refine health promotion interventions. Low rates of physical activity and healthy dietary patterns invoked strategies to disseminate existing diet, physical activity and physician counseling more effectively, including use of faith-based interventions. 35 Significant improvements for the study population in diet, physical activity and tobacco cessation were shown in a five-year follow-up study. 36
Practice-based research networks
Practice-based research provides a model that mixes scientific inquiry and community engagement. 37 PBRNs were developed to study health-care topics common in primary care practices. They have been defined as ‘a systematic inquiry, with the collaboration of those affected by the issue being studied, for purposes of education and taking action or effecting change 38 ’. AHRQ defines a PBRN as a group of ambulatory practices devoted principally to the primary care of patients, and affiliated in their mission to investigate questions related to community-based practice and to improve the quality of primary care. 39 PBRNs have access to diverse patient populations needed for clinical and translational research and are able to bring both community and patient needs to clinical research. There are over 100 PBRN networks currently in existence in the USA. On average these networks are young (4–5 years old), affiliated with a university or non-profit organization and most relied on members or outside organization to generate research ideas. 2 For the most part, these research questions are not ones that can be addressed adequately or most efficiently through the traditional approach of randomized controlled trials. Clinically useful answers are more likely to be attained through other research approaches such as observational studies, physician and patient surveys, secondary data analyses, qualitative research, mixed methods research and evaluations of clinical systems redesign. 40 PBRN patients tend to be younger, from a minority group or lower socioeconomic status. More than 600 peer-reviewed articles have resulted from PBRNs. Although community involvement was listed as a strength by one-third of networks, it was also noted to be a weakness by one-quarter. 2 Some PBRNs indicated that they lacked infrastructure to engage the community while others developed a community advisory board (CAB) discussed later. 2 PBRNs are gaining even greater relevance with the incorporation of community members in steering committees as well as CABs. In the following examples of PBRN research, typically no mention is made about the involvement of community. From the point of view of testing the effectiveness of using community in PBRN research, it would be helpful for authors to include this information in the future.
PBRNs in health-care disparity research
One PBRN was established to address disparities in health care by focusing on provider-specific strategies. They used disease-specific registries to identify treatment gaps and facilitate quality improvement processes among practices; developed practice-specific and guideline-based educational messages to promote quality care; engaged physicians for participation in studies; and developed a data repository of all trials that include significant numbers of African-Americans and other under-represented minorities. They anticipate addressing specific gaps in the health care of African-American and other minority patients by promoting quality care among its members and by facilitating participation in approved clinical trials. 22
PBRNs in prevention research
Primary care PBRNs serve as important research laboratories for the study of the practice and process changes that will be necessary to improve disease screening and prevention in primary care practices, where the majority of Americans receive most of their health care. As PBRN clinicians increasingly work at the interface between research and quality improvement, they are proving that networks can then be testing grounds for interventions aimed at improving screening through the use of research methods and evaluation strategies that typically go beyond traditional randomized controlled designs. One PBRN has population-based, longitudinal monitoring of the use of colorectal screening within a managed care population and has studied the occurrence of rare events, such as complications of screening procedures. 40 Nine PBRNs collected common data about cigarette smoking, diet, exercise and perceived physical and mental health. Unhealthy patient behaviors were associated with increased risk of physical or mental unhealthy days, suggesting a further reason that primary care clinicians should address behavior change with patients. They suggest implementing a brief, two-question, quality-of-life screening to target primary care patients with a higher prevalence of unhealthy behaviors. 41
PBRNs in diabetes research
There is a demonstrated clinical benefit to lowering blood pressure for hypertensive diabetes patients, with national guidelines calling for <130/80 mmHg. One recent PBRN study evaluated the clinical decision-making process of providers of diabetes patients with elevated blood pressure. 42 Barriers to achieving these goals are known to include patient compliance, the complexity of diabetes care and provider oversight. Optimal blood pressure control often requires three or more medications, leading to increased costs and rates of adverse drug reactions. Results showed that issues of polypharmacy, cost and the difficulties with complicated medication regimens were found to factor into how clinicians based their decisions. Interestingly, providers were less likely to act if the patient was not taking a medicine for blood pressure. The reasons given by providers for no action may reflect an individualized approach to patient care rather than an unquestioned adherence to guidelines. Although this might indicate an ongoing need for provider education, it appeared that balancing clinical decisions accounted for inaction, not provider knowledge deficits. 42
A PBRN study in New Mexico looked at the association of acanthosis nigricans with type 2 diabetes risk factors and disease in young persons. 43 Using a cross-sectional study among 1133 patients sampled, risk factors for type 2 diabetes were common and acanthosis nigricans was found in ∼20% of patients. Patients with acanthosis nigricans were more likely to have multiple risk factors for type 2 diabetes. This detection of acanthosis nigricans may help clinicians more rapidly identify high-risk individuals for diabetes counseling.
Another diabetic outcome study looked at the care provided by primary care clinicians to their patients using physicians' reports, surveys of patients about their diabetes care and medical record reviews, to determine medications used for diabetes and cardiovascular risk factor control. 44 Only modest numbers of patients were found to achieve established targets of diabetes control.
PBRNs in hypertension/cardiovascular research
In a cardiovascular study, one PBRN showed 22% of survey respondents were identified to have low levels of hypertension knowledge. 45 They concluded that continued efforts are needed to educate the public in lifestyle modifications to prevent hypertension, including the differences between curing hypertension and treating it with medications, and that hypertension usually causes no symptoms. The importance of developing messages that reach minority and low-literacy populations was emphasized.
In another PBRN survey on hypertension, 46 data were collected on demographics, diet and exercise for reducing blood pressure. Researchers found that although exercise as a preferred lifestyle change did not differ by race, implementation of such a behavior does. This may be related to differing income levels. When counseling patients, physicians must be prepared to ask what may hinder the adoption of such behaviors and be prepared to offer possible solutions to overcoming such factors.
PBRNs in mental health research
The development and spread of PBRNs in mental health began with a PBRN of over 700 psychiatrists formed in 1993 in order to promote more practice-relevant research in the field of psychiatry. 47 PBRN studies have examined quality of care in mental health treatments. One study showed problems in the treatment of patients with co-morbid depression and substance-use disorders, including potential overuse of benzodiazepines and under-treatment of the substance-abuse disorders. 48 When variations in the use of second-generation antipsychotic medication among African-American and non-Hispanic white patients in a national sample of adults who were treated by psychiatrists was studied, a substantial racial disparity was revealed. 49 Access to care issues for mental health delivery have been highlighted. There is concern that access to psychiatric treatment in public and managed systems of care has been significantly reduced. For example, PBRN research has shown that while most psychiatrists would accept new self-pay patients, only a minority would accept a new Medicaid patient and this rate was even lower for psychiatrists who were white, board certified or graduates of US medical schools. 50
One PBRN researched the evidence base of current psychiatric practices comparing patients seen in typical psychiatric practice with those seen in randomized control trials. Patients seen in usual care by psychiatrists were more likely to have more co-morbid conditions, be female, white and older than patients seen in clinical trials. Findings support the assertion that randomized control trial patients and treatments are not typical of those in clinical practice. In addition, most patients in clinical practice were found to be receiving treatments that did not have direct empirical support. 51 Another study examined what psychiatrists do with schizophrenic patients who are non-responsive to initial therapy with an antipsychotic medication. While most psychiatrists switched medications, in one-third of cases they used the less effective approach of adding an additional antipsychotic medication. The less effective polypharmacy approach was reported to have been more frequently used by psychiatrists who reported more frequent adherence to pharmaceutical-sponsored educational activities. 52
The blending of CBPR and PBRNs
Many PBRNs have already begun using participatory methods to build partnerships with health providers and practices to enhance the translation of research findings back into practice. 2,53,54 However, PBRN research has not traditionally included patients or community members. 2,55 The inclusion of community participation within a PBRN has been identified as an important next step with the potential to significantly enhance the research process by ensuring that the projects undertaken are directly applicable and informed by all stakeholders. 56–58 PBRNs are beginning to push this frontier by incorporating CBPR to expand the researcher clinician partnership and tackle difficult problems in the arenas of health disparities. 1 Practice-based research with participatory methods can be used to: (1) identify the problems that arise in daily practice that result in the differences between recommended care and the actual care patients receive; (2) demonstrate the feasibility of implementing treatments derived from randomized controlled trials; and (3) provide a laboratory for developing process improvements in primary care to maximize the number of patients who benefit from medical discoveries.
PBRNs can provide the environment to help eliminate health disparities by creating true partnerships and blurring the boundaries between clinical research- and community-based interventions (see Figure 2). 37 A survey gauging the interest of physicians in practice-based research showed that most physicians have a strong desire to be engaged in research that would improve care in their own practice, especially if they were recognized as a contributor, PBRN member or could get continuous medical education credit for research efforts. 59 One study on lessons learned from a PBRN-led study suggests that this type of research is best accomplished by: (1) building long-term relationships with clinicians and clinic staff; (2) demonstrating adaptability and flexibility for each practice site; (3) having adequate funding to support consistent data management and statistical support during all phases of the study; and (4) being able to be creative with recruiting patients and practices while maintaining the integrity of the protocol. 60
Involvement of PBRN with community is believed to function most effectively through a CAB or community advisory council (CAC). A CAB is a regularly organized meeting of people, including physicians, community members and researchers, focused on community health-care improvement through research. The composition of members of the CAB should be dynamic to reflect all potential stakeholders, and new members can be invited regularly depending on the research project. Through the CAB, community representatives can be involved throughout, including the needs assessment and problem identification; the formulation of the research question; the choice of methods; study design and implementation; data collection, analysis and interpretation; and finally dissemination of results (see Figures 2 and 3). The needs assessment and problem identification are key steps that will often drive the initial composition of the CAB. During this step, a problem of common interest between all stakeholders is identified. After setting the research question, the CAB assist in protocol development where board members can facilitate improved research design that is culturally acceptable and relevant. The CAB can also assist in data collection and analysis of results. Next, the results of the research must be shared with the community and followed through with incorporating these results into interventions that improve community health. Figure 2 shows the schematic approach to the development of CBPR within a PBRN. A follow-up analysis on the effectiveness of CAB-driven participatory efforts in combination with PBRNs would provide supporting experimental evidence that research outcomes involving CBPR methods can improve community health care.
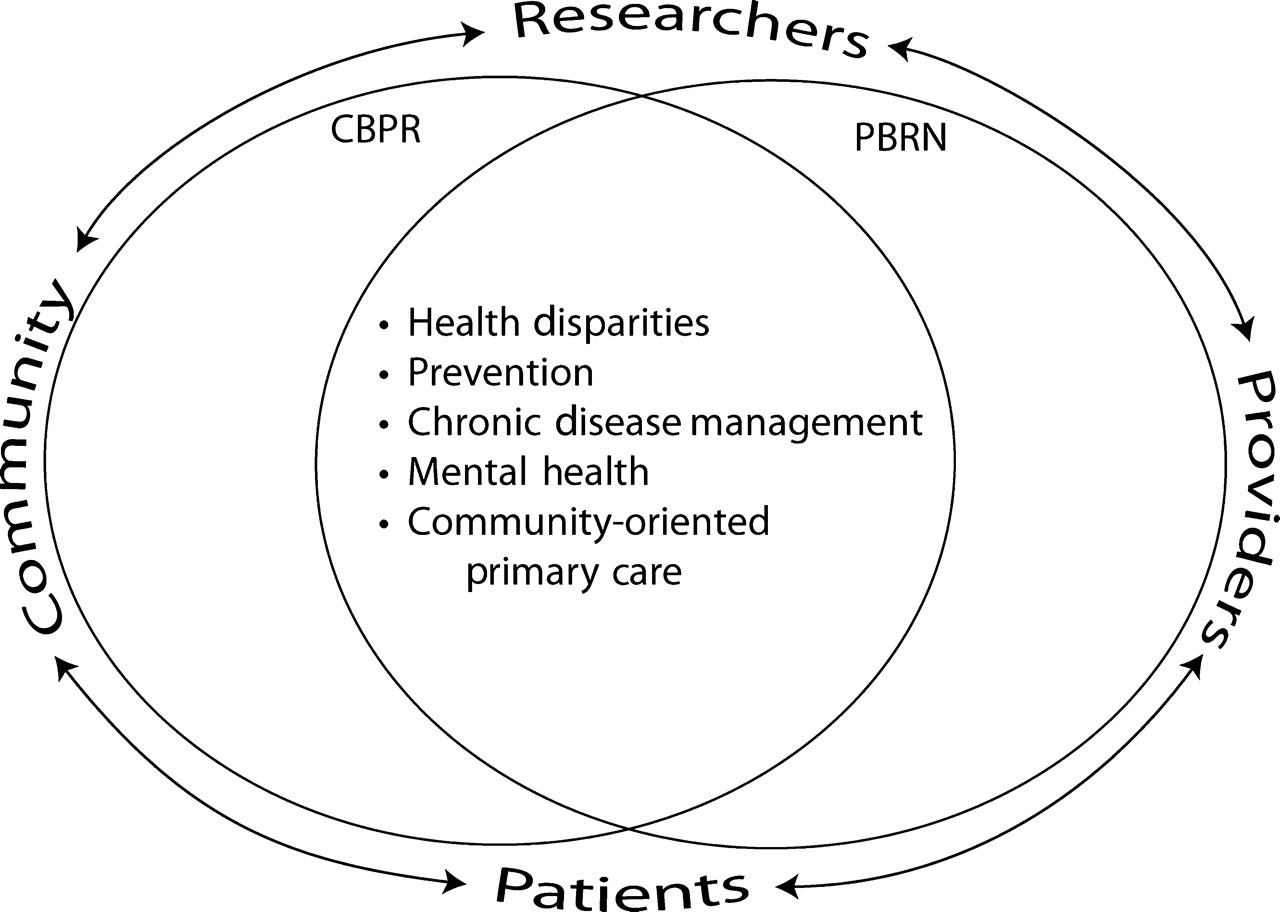
Research overlap between practice-based research networks (PBRNs) and community-based participatory research (CBPR)
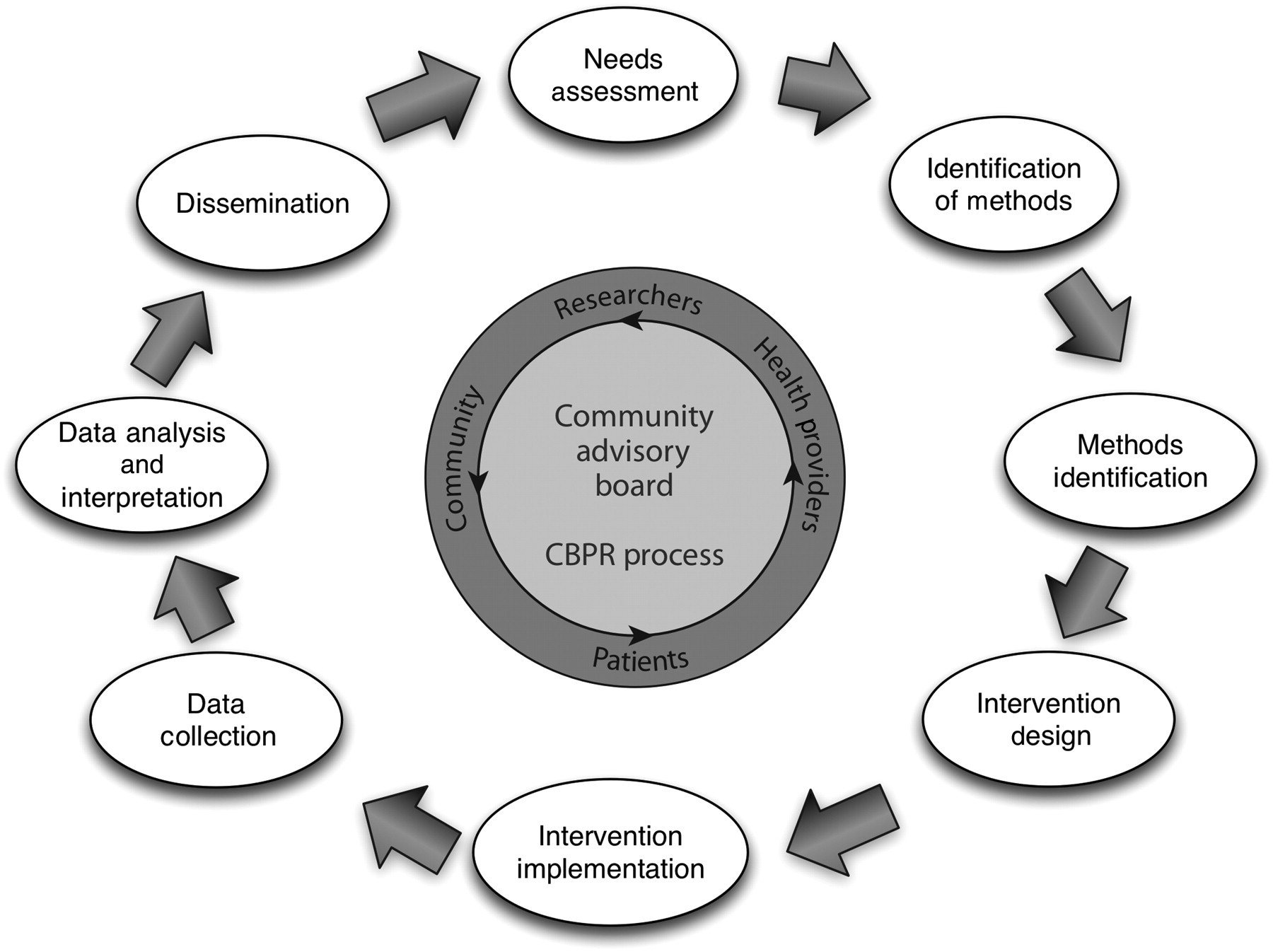
Theoretical process flow of research projects within the community advisory board of a practice-based research network (PBRN) operating with principles of community-based participatory research (CBPR). Research usually begins with a needs assessment, setting up of the community advisory board, and then follows along with methods identification, intervention design and implementation, data collection analysis and dissemination. The CAB meets regularly and is integral to the process. CAB, community advisory board
A recent study examined the use of CBPR within research networks. 55 Out of 46 participating PBRNs, 11 reported having a CAB or CAC, but only one network reported that the committees generated research ideas or assisted with data analysis. Barriers for community involvement were lack of interest, confidentiality issues, travel, language issues and a fear of not living up to community expectations. 55 Other significant barriers include the difficulty involved in defining the community (i.e. is the community defined using geography versus demographics or other variables) and matching community priorities with the scientific interest and ability of the PBRN. 8
Recently, the Mecklenburg Area Partnership for Primary Care Research (MAPPR) was set up to evaluate the health-care needs of under-served community members. Community leaders interested in collaboration were identified and invited to join the research network. Four key elements were built into the network to help optimize community participation. First, a research topic was chosen that was of interest and importance to all of the network members (i.e. health-care utilization and access for the Hispanic community). Second, the research project was designed to be relatively easy to accomplish, but still capable of generating information that provided insight for all participants into the community's health-care needs. This information was provided in the form of community maps that are easy to read and understand. The data were used by the network members to generate hypotheses regarding access patterns and naturally led into the next steps of designing interventions to ameliorate current problems. Third, a system of communication that closely connected researchers to community members and clinicians was designed. This included CAB meetings taking place at community sites and clinics on a rotating basis. Fourth, the steering committee for the organization has representative membership from both individual community members and community advocacy organizations and from providers' representative of each clinic site. Additional barriers to this type of collaborative research can be the need to educate Institutional Review Boards (IRBs) about community-based research and the need for all participants to adhere to Health Insurance Portability and Accountability Act laws and Good Clinical Practice regulations. For MAPPR, discussion with the IRB is an ongoing process leading up to each IRB submission. The MAPPR network conforms to the IRB requirements by treating all data that might be collected (including minutes from advisory board meetings and community forums) as potentially identifiable information. All data are kept confidential until the research team has reviewed it carefully and insured that no potentially identifiable data are present. In addition, when possible, data are collected without identifiers, and standard confidentiality practices are strictly maintained, including the safe keeping of data on secured computers that require password protection and in locked offices. When geographic information systems are used to analyze data, all identifiers but address are stripped from the data, and mapping of individual addresses is prohibited. When maps are shared all data are averaged into the nearest census tract, and additional safeguards are used to insure that no individual or group of 50 or fewer individuals could be identified. Often, waivers of consent are provided by the IRB for patient surveys and interviews where the potential exists for more confidential information to be collected from a signed consent than from the research itself. It is important to have the IRB process for participatory research because it helps to build trust with the community, allowing the community to feel safe in participating with this assurance of confidentiality.
Another PBRN that has successfully brought together the ideals of CBPR within a PBRN is Research Involving Outpatient Settings Network Net. This network formed a CAB and used this relationship to initiate an elegant study examining patient–provider communication about traditional, complimentary and alternative medicines. 8,61,62 Results showed that patients responded to an accepting, non-judgmental physician attitude before being open to discussion, while physicians often had reservations about using alternative therapies because of lack of knowledge about the efficacy, costs and safety of the therapies. The network found that adoption of a CBPR approach improved data collection and enhanced data analysis, and they conclude that for both ethical and practical reasons PBRNs should begin to embrace CBPR methodology.
One final example of a successful merging of PBRN research with CPRB principles is a PBRN that utilizes advanced practice nurses to deliver primary health care with the aim of reducing health disparities. This PBRN has successfully established a multisite, multistate collaboration for CBPR that will ultimately inform practice, education and health policy. 63 One study used a time-series design across eight different community nursing centers. Topics included food categories and nutritional content; principles of stretching and exercising; relationship of disease, such as hypertension, to diet and activity; and methods of stress reduction. Participants practiced safe exercises and used workout plans and walking routes. Data were collected and analyzed from chart audits; end-of-program telephone interviews, weekly and end-of-course participant satisfaction surveys; and preintervention and postintervention assessment. 63,64 This network identified key lessons learned with the use of CBPR principles, including maintaining vigilance for grant funding; determining ownership of data and dissemination plans at the outset; ensuring consistency of interventions across sites using videoconferencing; not assuming that providers will take on the role of principle investigator or being expected to maintain independent roles in the research process; having well-defined communication channels between all research team members; and understanding the intricacies and variability on the IRB processes. 65
Barriers and potential limitations of the CBPR–PBRN collaborative process include an inherent disconnect between academicians, physicians and community members. This gap can lead to a lack of trust and is part of the cultural and social class differences, divergent perspectives and research priorities, financial disputes, differences in sharing of power and resources, conflict resolution and balancing scientific rigor with physician needs and community acceptability. Effective strategies to overcome these barriers include: (1) building collaboration between community and physicians through an advisory board using established protocols to manage conflicts and encourage partnerships 66 and (2) using networking, methods training, on-the-job experience and community education strategies to build community relationships. 67 Indeed, the relationships between all key stakeholders are at the foundation of success for CBPR–PBRN projects, and time must be allocated for relationship building as reflected in participation in community events, demonstrating cultural humility and sharing power and resources. 15 Ideally, projects involving CBPR are a negotiated process between community, physicians and researchers, and when conflicts arise researchers should be open to reframing the research question through the partnership, and working collaboratively through mutually agreed principles built in to the advisory board to deal with conflict. 15 To maximize the chance that PBRN–CBPR will lead to tangible, lasting health benefits for communities, researchers will need to balance rigorous research with ways that balance scientific rigor and community acceptability. 68
Conclusion
In conclusion, CBPR has the potential to significantly advance PBRN research. Specifically, the PBRN–CBPR approach can: (1) guide the research process so that studies more closely match the needs of all stakeholders (including providers, patients and community members); (2) assist in the development of the research protocol and identification of research methodologies so that the study is more amenable to participants; (3) facilitate recruitment of research participants; (4) enrich the data collection and analysis; and (5) allow rapid translation of results from the study back into clinical practice and the community.
These benefits outweigh the potential challenges that accompany the adoption of CBPR methods; however, PBRNs should closely consider some of the potential downsides of the CBPR approach that include: (1) the loss of autonomy and power of the research team, especially the once revered principle investigator; (2) added time is required as many decisions about the research process may need to wait on community input and large amounts of time may go into debating seeming small concerns that do not change the overall research process; (3) data collection and analysis take on significantly increasing complexity that has the potential to become overwhelming; and (4) the research team must remain dedicated and have a continuous presence in a community that can often change rapidly in both composition and health-related needs.
Fortunately, researchers working within PBRNs often have the experience from working within complex practices to overcome the challenges of using CBPR methods. Indeed, CBPR might be considered by some as a natural extension of practice-based research – just with an expansion from the inclusion of only health providers to the addition of all stakeholders including patients and community members as research partners.
The key steps towards the adoption of CBPR within a practice-based research have been identified. These initial steps include:
The identification and/or definition of the targeted community. With the application of CBPR with a research network, health providers are considered to be key stakeholders and community members; The development of a representative CAB. This board should provide equal representation among all stakeholders and provide a framework for developing partnerships between all participants as well as providing a means of shared decision-making and conflict resolution; Working with all partners to complete a needs assessment.
Once the community's needs are clear, the network can take on research projects that address this deficit and are felt to be important by all participants. The initial project undertaken using these methods should be relatively easy to complete and will help build confidence of the participants. Next, clear mechanisms for communication between community members, researchers and providers need to be established along with procedures for decision-making and data sharing. Finding additional methods for getting input from participants such as focus groups and community surveys should be considered for selecting projects, identifying research methods and for data analysis and dissemination. Research projects should strive to assist in developing the human capital and community capacity. Finally, researchers need to be flexible and approach each project with an open mind and a willingness to learn.
Researchers will find that using CBPR methods greatly enriches their work and enhances their insight into the community. However, additional work is still needed to specifically show the benefit of using CBPR methods within PBRNs in terms of direct patient and community-level outcomes. This is particularly true given the potential of the application of CBPR within the PBRN framework to demonstrate novel mechanisms that can rapidly translate research findings back into practices and into the community. Once these mechanisms have been clearly elucidated, their widespread adoption will positively impact overall health at a both local and national level.
Footnotes
Acknowledgements
This work was funded by grants from The Robert Wood Johnson Foundation (#65236), the Agency for Healthcare Research and Quality, (RO3HS016023-01), and the Charlotte-Mecklenburg Health Services Foundation.