
Abstract
Dynamic mechanical disturbances in the aortic wall may lead to progressive aortic dilation and possibly aneurysmal formation. Here, we investigated the previously unexplored effects of aldosterone inhibition on aortic wall viscoelastic properties in hyperlipidemic rabbits. Thirty-six New Zealand male rabbits, fed a standard diet for four weeks, were separated into three groups: control (C; n = 10), standard diet; eplerenone (A; n = 12), hyperlipidemic diet plus 100 mg/kg/d eplerenone (last 4 weeks); and vehicle (V; n = 14), hyperlipidemic diet (no eplerenone). After eight weeks, animals were sacrificed and rectangular strips from the aortic wall, cut in radial and axial orientations, were prepared. Fresh, saline-wetted strips at 37°C were subjected to cyclic sinusoidal elongation from zero to 20% of the resting length at a frequency of 1 Hz. The dynamic biomechanical viscoelastic characteristics, ‘elastin phase’ low modulus (E L), ‘collagen phase’ high modulus (E H) and dissipated-energy index, were determined. Aortic tissue preparations were also examined histologically. Eplerenone increased aldosterone concentrations but did not affect blood pressure, cholesterol or potassium concentrations. There was a significant reduction of E H (from 3.40 to 1.80 MPa; P < 0.01) and E L (from 0.46 to 0.27 MPa; P < 0.05) in group A in the radial direction compared with group C. In the axial direction E L significantly increased in group A compared with group V (from 0.42 to 1.11 MPa; P < 0.01). Energy dissipation was not significantly different among groups, although there was a trend toward higher values in group A for both directions. Histological assessments revealed no significant differences in collagen or elastic fibers among groups. In conclusion, aldosterone receptor inhibition altered the viscoelastic properties of the aortic wall in hyperlipidemic rabbits without detectable microscopic changes in elastic or collagen fibers, an effect that progressively might predispose to dilation and/or aneurysmal formation.
Introduction
The aortic wall is composed of a thin inner layer (intima), a thick middle layer (media) and an outer layer (adventitia) of intermediate thickness. In contrast to smaller muscular arteries, the aortic media contains multiple layers of elastic laminae arranged in a spiral manner that confers maximal tensile strength. 1 It is this tremendous accretion of elastic tissue that gives the aorta not only tensile strength but also distensibility and elasticity, which serve a vital circulatory role. The endothelium-lined aortic intima is a thin, delicate layer. The adventitia contains mainly collagen and carries the important vasa vasorum, which nourishes the outer half of the aortic wall, including much of the media. 1
Aortic wall dynamic mechanical disturbances may progressively lead to conditions such as stiffness and sclerosis or aneurysmal dilation. Various factors have been implicated in the pathogenesis of these conditions, including hyperlipidemia and plaque formation, smoking history and hypertension; there is also a certain degree of genetic predisposition involved. 2 Notably, drugs used therapeutically may also affect the viscoelastic properties of the aortic wall by interfering with the extracellular matrix (glycosaminoglycans, proteoglycans, collagen and elastic fibers) or the cellular components (smooth muscle cells). 3 In particular, certain antihypertensive drugs have been associated with an increase in aortic wall stiffness, collagen turnover, changes in aortic diameter and aortic aneurysm formation. 3 Previous studies have shown that calcium-channel blockers are an independent risk factor for the development of an abdominal aortic aneurysm and are associated with increased aortic wall stiffness. 4 Angiotensin-converting enzyme (ACE) inhibitors, which act by interfering with matrix metalloproteinases (MMPs), are associated with decreased stiffness and increased collagen turnover. 5
The aldosterone receptor inhibitors, spironalactone and eplerenone, have an established beneficial role in the treatment of heart failure and hypertension, 6,7 but their possible influence on the integrity of the aortic wall has not yet been studied. Here, we investigated the effects of aldosterone receptor blockade on the mechanical viscoelastic properties of the abdominal aortic wall of hyperlipidemic rabbits.
Materials and methods
Animal experiments
To achieve adequate aldosterone blockade, we used eplerenone, which is a newer selective aldosterone receptor inhibitor that is as efficacious as the older agent, spironolactone, but has fewer side-effects. 8
Animal studies were performed with the approval of the Institutional Animal Care and Use Committee of the West Greece Prefecture and the University of Patras. Thirty-six New Zealand male rabbits (2.5–2.8 kg), housed at room temperature with a 12-h light–dark cycle, were maintained on a standard diet for four weeks, after which they were separated into three groups: (1) diet control (group C, n = 10), fed a standard diet for eight weeks; (2) eplerenone-treated (group A, n = 12), maintained on a hyperlipidemic diet (1% cholesterol; ELPEN pharmaceutical, Athens, Greece) for eight weeks and administered 100 mg/kg/d eplerenone (a gift from ELPEN pharmaceutical) plus 5% dextrose via gastric tube during the last four weeks; and (3) drug control (group V, n = 14), fed a hyperlipidemic diet for eight weeks plus a 5% dextrose solution (vehicle) via gastric tube for the last four weeks. Before animals were sacrificed, their blood pressure was measured through the central artery of the ear using a SURFLO Flash catheter (Terumo, Tokyo) and transducer. Blood samples were collected and total plasma cholesterol, potassium and aldosterone concentrations were measured. At the end of the study period, all animals were sacrificed and the abdominal aorta was carefully dissected. A piece (1.5–2 cm) from the same site of the infrarenal abdominal aorta was collected from each animal, taking care to avoid excessive distension of and/or injury to the vessel.
Tissue preparation and biomechanical measurements
Abdominal aortic sections were rinsed in normal saline (0.9% NaCl). Rectangular aortic wall tissue strips (2.5 × 20 mm), cut in an axial orientation, and rings (2.5-mm width), cut radially, were tested in a tensile testing machine (ML800 series, Test Resources, Minnesota, USA) suitable for cyclic sinusoidal uniaxial testing. Specialized, custom-made grips were used to secure soft tissue strips in the machine without damaging the tissue (Figure 1). This apparatus has the built-in ability to regulate the initial reference ‘zero length’ of the specimens. Zero length was defined as an initial elongation of the specimens to a length value at which application of a slight tensile force stimulated a corresponding further elongation; both applied force and elongation were monitored in oscilloscope traces in increased-sensitivity mode. This state simulates the physiological pretension state characteristic of all soft tissues, even those in a relaxed state. 9 Starting from this resting zero length, fresh, saline-wetted strips and rings (at 37°C) were subjected to cyclic sinusoidal elongation from zero to a maximum of 20% of the resting length at a frequency 1 Hz. After performing at least 10 preconditioning cycles, force and elongation were measured during each cycle using a 500 N piezoelectric force transducer system (Kistler 9203-5006) and a ±5 mm linear variable differential transformer elongation-measuring device (Lucas-Schaevitz DC-EC-250). Data from five tensile cycles were collected via an analog/digital conversion system at a sampling frequency of 100 samples/s and stored in a PC. The dimensions of the strips (width and thickness) were measured at the resting zero state using a laser micrometer device (micro-epsilon optocontrol 1200-5); zero length was measured using a digital camera and image analysis. Lagrangian stress (force/initial cross-sectional area) and strain (elongation/initial length) were then computed, and the viscoelastic biomechanical characteristics, ‘elastin phase’ low modulus (E L), ‘collagen phase’ high modulus (E H) and dissipated energy index (hysteresis ratio, h), were determined from stress–strain diagrams. 10

Front (a) and side (b) view of a ring-type specimen of aortic wall tissue secured on special grips of the tensile testing machine (A color version of this figure is available in the online journal)
Histological methods
All surgically resected aortas were fixed in 10% formalin and then embedded in paraffin. Five-micrometer-thick tissue sections were obtained from each paraffin block and transferred onto ready-to-use, poly-
Statistical analysis
All values were expressed as mean ± standard error. Continuous data among groups were compared using repeated measures analysis of variance followed by Tukey HSD (honestly significant difference) and Bonferroni tests for pairwise comparisons between group means. P values <0.05 were considered significant. Analyses were performed using SPSS for Windows, release 17.0.0 (SPSS Inc, Chicago, IL, USA).
Results
After eight weeks on a high cholesterol diet, the serum cholesterol levels of rabbits increased from 52.4 ± 6.7 mg/dL in the control group (C) to 1206 ± 160 mg/dL in the vehicle group (V) and 1410 ± 203 in the eplerenone group (A). Potassium concentrations were slightly, but not significantly, increased in the eplerenone group (A: 4.5 ± 0.2 mmol/L; C: 4.2 ± 0.4 mmol/L; V: 4.1 ± 0.3 mmol/L). Aldosterone concentrations were significantly increased (by 4-fold) in the eplerenone group (A: 1345 ± 110 pg/mL; C: 280 ± 23 pg/mL; V: 320 ± 28 pg/mL). Blood pressure was similar among groups (A: 107 ± 11/69 ± 3.9 mmHg; C: 115 ± 7.5/71 ± 3.6 mmHg; V: 118 ± 4.5/72 ± 4.1 mmHg).
Biomechanical tests
Table 1 shows the results from cyclic tensile tests in terms of the computed biomechanical parameters, E L, E H and h. Treatment of hyperlipidemic rabbits with eplerenone (group A) resulted in a significant decrease in E H in the radial direction compared with controls (group C) (E H = 1.80 MPa in A, 3.40 MPa in C and 2.60 MPa in V; P < 0.01), but there were no significant differences in the axial direction (E H = 6.40 MPa in A, 6.20 MPa in C and 5.00 MPa in V). E L was also significantly decreased in the radial direction in group A compared with groups C and V (E L 0.27 MPa in A, 0.46 MPa in C and 0.44 MPa in V; P < 0.05). Unlike E H, E L was significantly increased in the axial direction in group A compared with group V (E L = 1.1 MPa in A, 0.55 MPa in C and 0.42 MPa in V; P < 0.01). Neither high nor low modulus elasticity values were significantly different between groups C and V either in the radial or in the axial direction. The energy dissipation index (h) was not statistically different among the three groups, and ranged from 0.23 to 0.25 radially and 0.17 to 0.22 axially, although there was a trend toward higher values in group A for both directions.
Biomechanical characteristics (mean ± SE) of the aortic wall for groups C, V and A in radial and axial directions
High modulus of elasticity (E H) (slope of collagen phase stress–strain curve); low modulus of elasticity (E L) (slope of elastin phase stress–strain curve) and hysteresis ratio (h) (dissipative energy/loading energy). MPa, megapascal
*,**P < 0.05
Histopathology analysis
Standard H&E staining revealed no significant differences in the histological features of aortas among the different animal groups; all three wall layers (tunica intima, tunica media and tunica adventia) were microscopically normal in all samples examined (Figures 2A–C). This finding is consistent with results from histochemical analyses with Masson Trichrome-aniline blue staining, which showed the same structure and distribution of collagen and muscle fibers in all animals evaluated (Figures 2D–F). Similarly, the Weigert Van Gieson method did not uncover any remarkable changes in the elastic fibers of the aorta walls among rabbits in the different groups (Figures 2G–I).
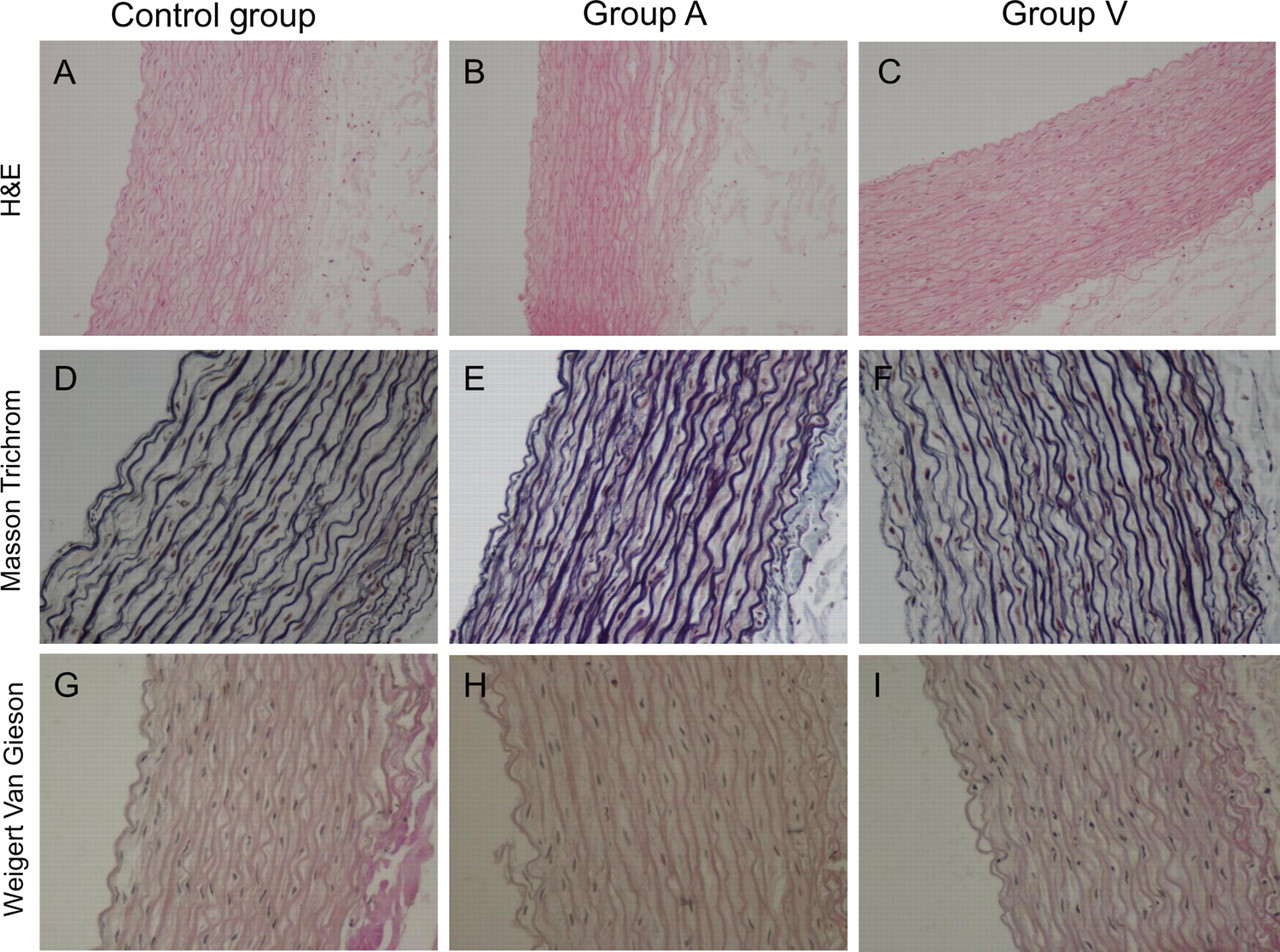
Hematoxylin and eosin (H&E) staining (A–C), Masson Trichome with blue aniline (D–F) and Weigert Van Gieson staining (G–I) revealed no remarkable differences in the structural and morphological features of the aortic wall among the experimental groups (A–C: original magnification ×20; D–I: original magnification ×40) (A color version of this figure is available in the online journal)
Discussion
Several studies have shown that various antihypertensive drugs may affect the integrity of the aortic wall. 3 Specifically, calcium channel antagonists may potentiate elastase activity and can increase the growth of aneurysms in animal models. 4 Furthermore, some MMPs implicated in the metabolism of elastin and collagen depend on zinc for their activity. 5,11,12 Because ACE inhibitors such as captopril bind to zinc at the active site of ACE, 12 these agents may increase collagen turnover.
To the best of our knowledge, no studies have addressed the influence of aldosterone receptor inhibition on the viscoelastic properties of the aortic wall. Our findings from biomechanical testing showed a loosening of the aortic wall following hyperlipidemia. This was not unexpected since hyperlipidemia causes vascular remodeling in association with upregulation of transforming growth factor-β1, MMPs and elastase, increased collagen turnover, infiltration of macrophages and a decrease in the number of smooth muscle cells – the main source of glycosaminoglycans (GAGs) and proteoglycans. 13 This remodeling decreases the strength of the aorta, which becomes vulnerable to dilation. Notably, we found that the degree of aortic wall loosening continued to increase and became statistically significant in hyperlipidemic animals treated with the aldosterone antagonist, eplerenone. This conclusion was based on the observed reduction in E H and E L values. E H, the slope of the stress–strain curve in the second linear region (i.e. the higher strain range) reflects the resistance of collagen fibers to strain. E L, the slope of the first linear region of stress–strain curves (i.e. the low strain range), on the other hand, mainly reflects the ability of the elastin fiber network to resist strain in the direction of testing. 14 Reduced E H and E L values, found mainly in the radial direction, may be explained as a reduced ability of the aortic wall to resist dilation in the radial direction. The observed viscoelastic changes in the aortic wall could lead progressively toward established degeneration and ultimately to dilation and/or aneurysmal formation.
Eplerenone is a well studied aldosterone antagonist that may alter the extracellular matrix remodeling and collagen turnover. In a substudy with 476 patients of the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study, eplerenone significantly reduced the procollagen type I and III aminoterminal peptide concentrations after six months of follow-up. 15 Similarly in 44 patients with preserved systolic function heart failure, eplerenone attenuated the increase in pro-collagen type-III aminoterminal peptide at 12 months, while no significant impact had been observed at six months. 16 Interestingly, it has been shown by in vitro studies that pretreatment of rat mesangial cells with eplerenone prevented aldosterone-induced cell hypertrophy, actin polymerization, increase in alpha-smooth muscle actin expression and the increases of mRNA levels of collagen type I, III and IV in rat mesangial cells. 17 As a result eplerenone inhibited myofibroblastic transdifferentiation in the mesangium, a process that plays a pivotal role in other diseases also, such as atherosclerosis and calcific aortic stenosis. 18
Recently, Savoia et al. 19 reported that hypertensive patients treated promptly with eplerenone had reduced arterial wall stiffness after one-year follow-up due to decreased collagen/elastin ratio. On the other hand, there is limited data regarding the influence of eplerenone on the aortic wall of normotensive subjects. In this study, despite the differences in the mechanical properties among the three groups, we did not uncover any differences in the quantity of elastic or collagen fibers of the aortic wall at the microscopic level. This prompted us to hypothesize that the observed biomechanical differences are caused by changes in the macromolecules that link and stabilize cells and the extracellular matrix. Collagen cross-links stabilize collagen fibrils, preventing slippage of adjacent molecules in response to an applied tensile stress. 20 By promoting formation of end-glycation products, aging, hypertension and diabetes are prominent contributors to increased arterial stiffness. 21 In elderly subjects with systolic hypertension, drugs with collagen cross-link-breaking properties significantly reduce arterial stiffness and pulse pressure without altering mean pressure. 22 These compounds provide evidence that arterial stiffness can be reduced independently of mean pressure and without modifications in collagen density or content. GAGs possess viscoelastic properties by virtue of binding to sodium and water, as well as through calcium cross-linking of the helical chains. 23 In a previous study on bovine pericardial tissue, we showed that a reduction of GAGs, even by as little as 30%, is accompanied by a reduction of tissue viscoelastic characteristics. 10 Other adhesion molecules, such as integrins, fibronectin and proteoglycans, have also been reported to modify wall stiffness. Fibronectin matrix polymerization increases the tensile strength of model tissue. Quantitative studies of aortic fibronectin suggest that an increased number of attachment sites between smooth muscle cells and the extracellular matrix may be responsible for increased arterial rigidity. 24 Similar results have been observed with a high sodium diet or chronic administration of aldosterone. 25,26 Conversely, the loss of cell–matrix attachments between α1 integrin receptor and its ligand, fibronectin, is associated with a reduction in wall stiffness at any given value of wall stress. 27 Aldosterone blockade with either spironolactone or eplerenone reverses arterial wall stiffness by interfering with collagen cross-links and cell–matrix attachments. 25,26,28,29 Although this is obviously a desirable effect, it is reasonable to hypothesize that the continuing action of chronic aldosterone blockade might lead one step further: from reversing wall stiffness to loosening it to below normal levels, rendering the wall susceptible to dilation. This would occur when deactivation of cross-links, adhesion molecules and cell–matrix attachments exceeded a critical threshold; neither the threshold values nor the time required to reach them have been precisely characterized. Consequently, changes in wall tensile strength can be achieved without microscopic modifications in the main structures. Further studies are needed to determine the functional and structural modifications of these cross-links and the attachments between matrix and cells.
In conclusion, aldosterone antagonism alters the viscoelastic properties of the abdominal aorta of hypercholesterolemic rabbits, increasing its vulnerability to dilation and, with continued progression, to aneurysmal formation. These changes may be caused by local changes in the attachments and cross-links of arterial skeletal components. Although eplerenone has an established beneficial role in heart failure and hypertension, 7 these findings should be taken into consideration for the long-term treatment of patients.